|
| |
This assay detects the presence of circulating fragments (FDPs) of fibrinogen and soluble (non-crosslinked) fibrin that are produced by the action of plasmin on these substrates. Plasmin acts on these 2 substrates similarly, producing an initial cleavage product called fragment X. Plasmin then acts on fragment X, cleaving it into a transient fragment Y, and fragment D. Further cleavage of fragment Y, produces the terminal fibrin(ogen) degradation products, fragment D and E. Thus from one molecule of fibrinogen or soluble fibrin, 2 terminal FDP fragments D and one terminal fragment E is produced (as shown below).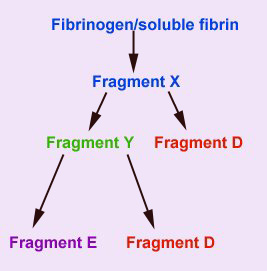  Two mls (as little as 0.5 mls can be used if the patient is very small) of blood from the patient is put immediately into one of the tubes provided with the test kit (see image on the right). Serum from the tube is diluted 1:5 and 1:20. A small volume of each dilution is mixed on a plate with an equal volume of the antibody-coated latex beads. Positive and negative control sera are assayed concurrently. Agglutination of the beads at the 1:5 dilution indicates an FDP concentration of 10-40 µg/ml, whereas agglutination at both 1:5 and 1:20 dilutions indicates an FDP concentration >40 µg/ml. Either positive result is abnormal and indicates a higher than normal rate of degradation of fibrinogen and/or fibrin by plasmin or decreased clearance of these products. Two mls (as little as 0.5 mls can be used if the patient is very small) of blood from the patient is put immediately into one of the tubes provided with the test kit (see image on the right). Serum from the tube is diluted 1:5 and 1:20. A small volume of each dilution is mixed on a plate with an equal volume of the antibody-coated latex beads. Positive and negative control sera are assayed concurrently. Agglutination of the beads at the 1:5 dilution indicates an FDP concentration of 10-40 µg/ml, whereas agglutination at both 1:5 and 1:20 dilutions indicates an FDP concentration >40 µg/ml. Either positive result is abnormal and indicates a higher than normal rate of degradation of fibrinogen and/or fibrin by plasmin or decreased clearance of these products. There are newer latex-agglutination kits that are based on monoclonal antibodies that do not cross-react with intact fibrinogen and can thus be used on citrated plasma samples. This is advantageous compared to serum FDP assays, as a specialized collection tube for FDP assay is not required and a single citrated blood sample can be used for all coagulation tests. This is the procedure performed by the Clinical Pathology laboratory at Cornell University and it has only been validated for the dog. The plasma FDP assay is performed similarly to the serum FDP assay, except dilutions of 1:2 and 1:8 are made, with results being reported as < 5 µg/ml, 5-20 µg/ml and > 20 µg/ml. Results > 5 µg/ml are abnormal. | |
 | |
|
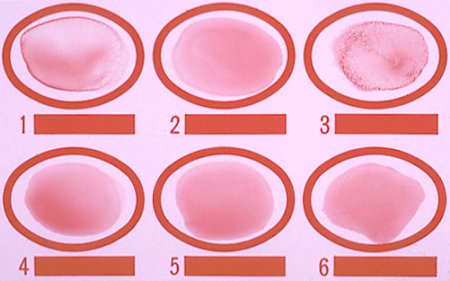
Illustration of a plasma FDP assay: Positive and negative controls are in wells 1 and 2. Agglutination is evident in well 1 but not 2, indicating correct functioning of the test. Two canine patient samples are being tested concurrently. The first patient plasma is in wells 3 (1:2 dilution) and 4 (1:8 dilution), the second in wells 5 (1:2 dilution) and 6 (1:8 dilution). Agglutination is only observed in well 3. This is compatible with a positive plasma FDP result of 5-20 µg/ml for patient 1 and a negative plasma FDP result (< 5 µg/ml) for patient 2. | |
| The FDP assay is used with the other coagulation tests to characterize bleeding disorders more completely. The results should never be interpreted alone, without evaluation of clinical signs and results of other coagulation tests. Any cause of pathologic intravascular coagulation (the most common of which is DIC), thrombosis, or severe internal hemorrhage (see below) can produce FDP's. In addition, any condition causing decreased clearance of FDPs by the liver and monocyte-macrophage system, e.g. severe liver disease, can also result in increased FDP values. A negative FDP result does not rule out these processes. Note that coagulation can also occur in extravascular tissue spaces
and high FDPs have been associated with fibrin(ogen)olysis occurring
in protein-rich or hemorrhagic effusions into body cavities. Indeed,
horses with colic due to gastrointestinal disorders have higher FDPs
in blood and peritoneal fluid than healthy control horses. Although
the high FDPs in the blood of these colic horses are compatible with
DIC (which is often subclinical in horses and results in thrombosis
rather than hemorrhage), the FDP values in their peritoneal fluid were
higher than in blood, suggesting extravascular production of the FDPs
(probably secondary to inflammation-induced tissue factor expression
and fibrinolysis in the peritoneal cavity). This could have partly contributed
to the high blood FDPs.
|