This 33-year-old woman has established essential hypertension with evidence of end-organ effects (mild retinopathy, S4) along with other cardiac risk factors (borderline hyperlipidemia, family history of premature cardiac disease). Drug therapy is warranted. Because the patient could become pregnant, one should select an agent that can be safely administered during the first trimester of pregnancy.
ACE inhibitors are contraindicated in pregnancy because they are associated with fetal growth retardation, congenital malformations, neonatal renal failure and death. Atenolol has recently been shown to affect fetal hemodynamics as well as fetal growth. Data concerning the use of other ß-blockers during pregnancy is inconsistent, although many experts avoid using ß-blockers in pregnant women.
Methyldopa, labetalol and nifedipine are the preferred agents to manage chronic hypertension in pregnant women. Methyldopa is the drug most often used in randomized trials to treat chronic hypertension in pregnant women because of its established record of not affecting fetal outcome. In randomized trials, labetalol compares favorably with methlydopa in not affecting fetal outcome. Experience with calcium channel antagonists is limited, but they appear to be safe and are often used to manage severe preeclampsia. However, calcium antagonists may interfere with labor. Hydralazine has also been used safely in pregnancy. Diuretic therapy in pregnancy is associated with lower-than-normal degree of plasma volume expansion and the issue of continuing therapy during pregnancy is controversial. The National High Blood Pressure Education Program Working Group recommends that therapy be continued in women already receiving a diuretic prior to conception.
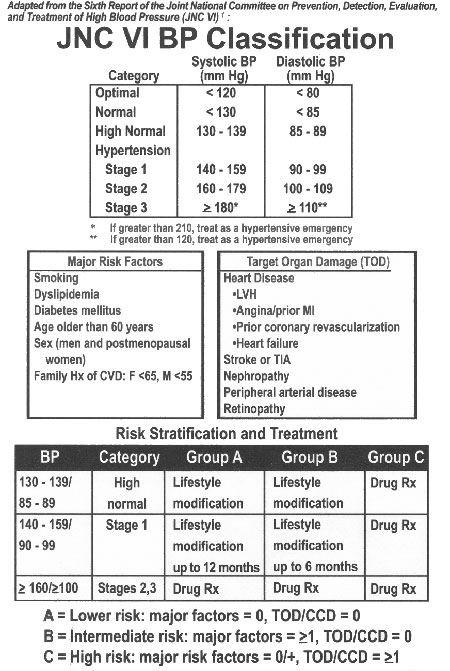
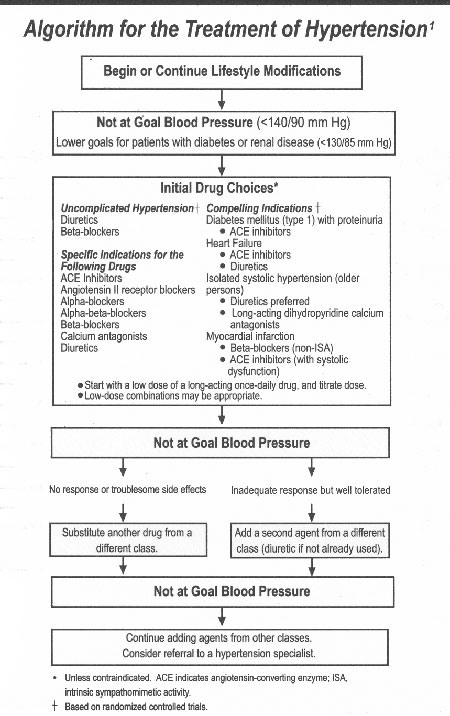
Being able to select the appropriate blood pressure lowering agent for the right patient can be difficult. To assist you please refer to the following algorithms from JNC VI :
References:
![]()