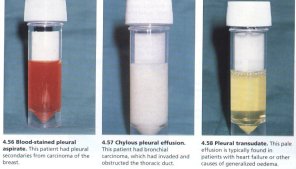
The first question that must be answered whenever a pleural effusion is discovered is whether it is a transudate or exudate. Direct visualisation of the fluid can be of some help:
To serve as guides (to supplement clinical suspicion) , an exudate is defined as meeting any one of the following three criteria, while transudates meet none (1):
Approximately 80% of exudative pleural effusions are caused by pneumonia, pleural malignancy, or thromboembolism. When this is accompanied by an elevated pleural fluid amylase the differential diagnosis centers on malignant pleural effusions due to a primary lung or metastatic adenocarcinoma, pancreatitis, a pancreatic pseudocyst, or esophageal rupture. Your clinical suspicion based on clinical features should be paramount. The literature is filled with case reports of transudative effusions with malignancy and exudative effusions with benign conditions.
The presence of weight loss and a unilateral pleural effusion should raise your concerns about a possible malignancy. The finding of a hemorrhagic (>100,000), mononucleocyte-predominant further supports the diagnosis. Negative pleural fluid cytology does not exclude malginancy since it is positive in only 50-60% of patients with malignant pleural effusions. Approximately 10% of malignant pleural effusions have an elevated pleural fluid amylase, which interestingly is salivary rather than pancreatic isoenzyme.
Pleural effusions secondary to pancreatitis or pancreatic pseudocysts typically have pleural fluid amylase levels above 1,000 and are more commonly left-sided. Early on in pancreatitis, the pleural fluid amylase may mildly elevated, but the pleural fluid leukocyte count would be neutrophil predominant and an erythrocyte count >100,000 would not be found. A pleural effusion due to a ruptured esophagus is neutrophil predominant and associated with abdominal findings and most often has a low pH (at least <7.30 and typically <7.00). Tuberculous pleurisy is not associated with elevated pleural fluid amylase; it is excluded with pleural fluid findings of pH >7.40 and mesothelial cell count greater than 5% of total cells.
References:
![]()