
|
|
RENAL CASTS Contents of This Section (All links are to subsections within this file.) Origin and Composition of Casts Composition—The Tamm-Horsfall protein is a glycoprotein isolated from normal urine by Tamm and Horsfall in the early fifties. This protein is excreted by the thick ascending branch of the loop of Henle and the first part of the distal tubules. Normal daily excreted quantity ranges from 25 to 50 mg. The protein has a huge molecular weight of around 7 millions Daltons, with 25% to 40% of its weight being carbohydrates. This protein is the major fraction of the uromucoprotein. Properties—The TH protein has characteristic properties. This protein precipitates as a gel in a 0.58M NaCl solution, and redissolves in deionized water, or in an alkaline buffered solution. If albumine is added to a pure water solution of TH protein, the latter will precipitate and form a gel, taking the shape of the glassware used. Because of this property, casts are believed to dissolve readily in diluted or alkaline urine. Transposing an in-vitro experiment in a real physiological situation is sometimes hasardous. Other factors could stabilize the cast, so that a slight alkalisation (bacterial growth) of the urine does not necessarily mean cast dissolution. Tamm-Horsfall protein and casts—It as been demonstrated that, hyaline cast, cylindroids, and mucus threads, are all made of Tamm-Horsfall protein fibrils. Casts are elements of the urinary sediment, formed by the polymerisation of the Tamm-Horsfall fibrils, taking the shape of the site of its formation (casting). Casts are formed, after the loop, in the late section of the distal tubules and the early section of the collecting tubes. The formation site is the nephron's section where the dilution is maximal. As mentioned earlier, fibril's formation is inhibited by a low ionic strenght, and the precipitation is promoted by the addition of albumin. This scheme is quite similar to the environment where casts formation occurs. The Tamm-Horsfall protein is the cast fundamental substance. It is believed that all the elements needed for cast formation are in place. Some factors (found in abnormal urines) seem to promote casts formation while others (found in normal urines) have an inhibiting effect. Casts are formed when the equilibrium between promoters and inhibitors is broken. Factors known to be promoters of cast formation are:
Addis has described many different types of casts, and has established the relation between these casts, and clinical conditions. He has also proposed an evolution scheme for casts. In his proposal, cellular casts degenerate as coarsly granular casts, which degenerate in finely granular casts, and finally become waxy casts. Haber has demonstrated that the waxy casts were made of an amorphous material, associated with Tamm-Horsfall fibrils. This structure does not support the evolution theory of Addis. On the other hand, Lindner has demonstrated that type II granular casts (finely granular) are related to the granular cytoplasm of degenerated renal tubular cells. Some relation between the different casts is demonstrated, but the complete evolution theory of Addis was presented as, and remains, a speculation. Lindner's mechanism of cast formation—The casts matrix is formed of uromucoprotein fibrils and is builded by a mechanism described by Lindner. The mechanism has four steps: initiation, growth, maturation, and evacuation. Initiation—The first fibrils are fixed to the distal, or collector tubular walls, forming a porous sponge like lattice. Since the initial cast has large pores, urine and small debris pass through. These initial fibrils are made of Tamm-Horsfall protein. This stage could correspond to the early hyaline cast described by Lindner. Growth—As time goes, more and more elementary fibrils, and maybe other proteins, are added to the initial structure, making the pore smaller. The declining pores size reduces the urine flow through the structure. The flow will eventually stop. Maturation—After complete obstruction of urine flow, the cast matrix is modified by the tubular activity. The maturation period depends on the nephron activity, especially at the blockade region. Proteins, probably originating from the surrounding tubular cells, are added to the structure. Evacuation—Because of the surrounding cells activity and the hydrostatic pressure, a time comes where the cast loses its adherence to the tubular wall. The casts are then evacuated by the urinary flow. There is no widely accepted rules for the cast nomenclature. The names used to report casts should consider the following facts. Facts
Rule of third—It has been proposed that, if more than one third of a cast is filled with an element, then the cast takes the name of the element. On the opposite the term "hyaline ..element cast" should be used. This term should be used with care since it could be interpreted by some as a less pathological cast, which is really not the case. Using the term hyaline..element in a report, where there is also mentioned, the "element cast", should be avoided. Reporting "hyaline element cast" and "element casts" one the same report gives a longer report without any benefit to clinical significance. In this context, the report should mention hyaline casts and element casts. Mixed cast—As mentioned earlier, there is no segregation mechanism in cast formation. Many casts are made of mixed elements. Some use the term "mixed element1-element2" to report these casts. The term mixed, without further precision, should not be used since it says nothing. Care should be taken with the mixed casts in routine urinalysis; the report must not look like a grocery list. An easy way to overcome this potential problem, is to split the mixed cast into its element and reporting two casts; element1 casts, and element2 casts. This solution as the advantage of shortening reports without any loss of clinical significance. The casts seen in the urinary sediment can be made of a typical hyaline or a typical waxy matrix. But many casts have a matrix that seems to be an intermediate between these two. Casts having a different matrix at one end are not rare. To our view, the cast matrix can vary from the perfectly hyaline to the perfectly waxy. The matrix type is the result of the intratubular maturation time. A cast evacuated shortly after is formation will have a hyaline matrix. A cast remaining for a long period in the nephron will have a waxy appearance. This situation is encountered in conditions of low urine flow. Waxy casts were at a time called renal failure casts. From this view, any element cast can have a hyaline to waxy matrix. Usually the term "waxy" is reserved to the typical waxy cast.
Lindner has demonstrated changes in the aspect of the hyaline cast, in time ordered specimens, after a strenuous physical exercise. Shortly after exercise, the first hyaline casts "Early" seen are difficult to see in bright field microscopy. These are more easily observed in phase contrast microscopy. Under scanning electron microscope "SEM", these have an empty appearance. These casts are believed to be in an unstabilized state, making them readily soluble. The second type are the ""Typical"" hyaline casts. Compared to the early form, the typical hyaline casts have a homogeneous filled structure. These casts are in a stabilized state less subject to dissolution. The third form is the "Wrinkled" hyaline casts. This type has a wrinkled matrix, probably due to unequal internal tension within the matrix. The last form observed in the experiment is the "convoluted" hyaline casts. It seems that this form is due, again, to internal tensions creating a helix like structure. Variations in shape and texture of the hyaline casts are, for the moment, of no clinical value.
To our view, waxy casts represent a long time maturation of the convoluted cast. With time, the matrix gets more dense and proteins are added, resulting in typical waxy matrix. The clinical meaning of a waxy-element cast is dictated by the element and not by the matrix, and should be reported as an element cast. The term waxy cast is reserved to the typical inclusion-free or slightly granular waxy casts.
Width (The large cast)— Casts can be classified, on a width basis, as normal, enlarged and large. Enlarged casts (1.5 x normal) are formed in a dilated tubule. In acute tubular necrosis of ischemic origin, casts are frequently enlarged. Enlarged casts should not be confused with the true large casts. The large casts are usually related to a chronic renal failure state. In this specific situation, the remaining functional nephrons try to take over. These will have an oversized glomerule and large tubules. Casts formed in these nephrons have a width of four to ten times the normal size. The large waxy casts were, at a time, called the end stage renal failure casts. Large casts should be reported as large.
Blood casts are of prime clinical significance. Even a rare finding is indicative of renal "glomerular" bleeding. This finding can obsolete the need for invasive urologic tests to determine the origin of the hematuria. Blood casts are mostly found in glomerulonephritis. Since the final diagnosis of GN is obtained through a biopsy, precaution is a rule before reporting blood casts. Finding blood casts in the routine batch is a rare event. Everyone should be concious that over identification of blood casts is as bad for credibility as failure to recognize them. Blood casts are usually found in a context of a proteinuria (slight or heavy), and hematuria. The hematuria is characterized by a high percentage of red cells dysmorphocytosis. Specimens with these figures, especially dysmorphocytosis, should systematically be scanned for blood casts. In some cases of GN, the proteinuria is minimal. Like any natural coloration, the orange red color (Burnt sienna), typical of the blood casts, is best seen at low power field (obj.10x). At higher magnification, colors have a faded tint.
It seems that the true blood casts are a bit more specific to glomerular hematuria than the red blood cells casts. The cast inclusions are made of hematine arising from red cells degeneration, and from fibrinolysis of microclots. Distinction between the true blood casts and the red blood cells casts is not always obvious. We are using a simple rule: if the matrix is hyaline, the cast is reported as a red blood cells cast, and if the matrix is waxy, the cast is reported as a true blood cast. Since both casts have a nearly indentical clinical value, this simplification is acceptable.
Hemoglobin casts and myoglobin casts are hyaline casts having a protein pigmented matrix. In these cases, the pigmentation is acquired through the incorporation of the pigmented protein not by a breakdown process. The myoglobin or hemoglobin reaches the urinary space through filtration. This situation does not necessarily imply a glomerular disease. Myoglobin casts can be seen in massive muscular breakdown (crush syndrome) while hemoglobin casts can be seen in intensive intravascular hemolysis as, in malaria and catastrophic transfusion error. The dirty brown casts (heme degradation products pigmented granular casts) are sometimes difficult to differentiate from the blood casts or the hemoglobin casts. These casts are treated elsewhere. In a routine urinalysis, the term cellular cast means a cast having a hyaline or waxy matrix with inclusion of cells. The most frequent cells are the collecting tube cells. Other possibilities of cells exist but, as already mentioned, it is unlikely that one could distinguish them without staining.
A very few hyaline RTC casts or RTC casts can occasionally be encountered in a healthy person's urinary sediment. In this context, these casts have no more clinical meanings than the hyaline casts. The renal tubular cell casts are not associated to a precise pathology, but are found in multiple conditions that affect the renal tubules. The RTC casts are non specific. Among pathologies associated with the presence of these casts let us mention: the acute interstitial nephritis, acute transplant rejection, and tubular necrosis. Necrotic RTC casts are seen in acute tubular necrosis and in nephrotoxic tubular diseases. The typical renal tubular cell casts are described as hyaline matrix casts, showing two rows of well delimited tubular cells. The two rows criteria is not reliable because the white blood cell casts can also appear with this particularity. Sequestrated tubular cells in a hyaline matrix is possible, but studies on the subject seem to indicate that the majority of casts of this type are formed of cells fixed to the surface of the casts. White blood cell casts in routine urinalysis refer to a hyaline matrix cast bearing neutrophil inclusions. This simplification is justified by the fact that the neutrophil is, by far, the most frequently seen cell in these casts. With a PAP staining, other leukocytes can be identified within WBC cast. Except for the lymphocytes, all the other leukocytes casts have been described in the literature. In our view, it is reasonable to think that this cast exists in certain clinical conditions. Plasma cell diseases, infiltrating the tubular interstitial tissue, can be expected to give lymphocytes casts.
White blood cell casts are found in renal diseases when the complement factor C3 is activated, thus generating an inflammation process. Pyelonephritis (cortex), acute allergic interstitial nephritis, and some glomerulonephritis are diseases activating the C3 factor. The identification of the polynuclear cells is possible by the demonstration of specific enzymes. The Naphtyl AS-D chloro-acetate esterase is found in the granulocytes, the mastocytes, and in some macrophages. This staining method can demonstrate the presence of polynuclear cells sequestrated in a cast matrix (hyaline WBC cast). This method allows a much greater sensitivity toward the detection of white blood cell casts. With this high sensitivity, one can find a hyaline cast with only one or two leukocytes within the matrix. The problem is the clinical meaning of this otherwise undetected figure. Some think that this finding is significant and represents a low or a silent nephritis.
Bright field identification of unstained cellular casts is not an easy job. The two pictures shown are illustrating this difficulty. The use of the Naphtyl AS-D chloro-acetate esterase staining procedure has permited us to positively identify the first casts as an RTC cast and the second as a WBC cast.
Urinary eosinophiluria (> 7% of WBC) is found in acute allergic interstitial nephritis and in other conditions. White blood cell casts containing eosinophils can exclude an extrarenal origin for the eosinophiluria. These eosinophil casts can be demonstrated with the Hansel stain. Unfortunately, the smear stain version has a low recuperation with casts. Cytospin specimen should be used. The acetate filter PAP staining method is also a good option. The presence of monocytes within casts has been demonstrated using the monoclonal antibodies of the FMC series. This finding is associated with acute allergic interstitial nephritis, and with rapidly progressive glomerulonephritis.
The oval fat body casts are special. Identification of these cells is easy with the use of polarized light. The fat droplets are typically birefringent with a maltese cross interference pattern. Since oval fat bodies are often of macrophage nature, oval fat body casts are considered as special cases of macrophages casts.
The oval fat body casts are associated with the nephrotic syndrome. The urinary context will be one of a high proteinuria. If the specimen has a dipstick reaction positive for blood, then, the presence of blood casts is expected. The clinical significance of the hyaline fatty casts is unknown. These casts were found twice in apparently healthy persons. We haven't found any explanation or outcome in the literature about this situation. On the otherhand, this figure is frequent and considered as moreless significant in feline. (http://128.253.82.7/block3/ua-sed/fatty.htm)
The texture varies from finely granular to coarsely granular. The granules size is often the same for all the casts on a specimen or on different specimens of the same patient, but is variable from one patient to another. Examples of this variation is shown in our picture collection. Coarse granules do not seem to be more clinically significant than the fine granules and are probably due to different synthesis conditions. These granular casts are non specific and represent a degradation of the tubular epithelia environments. A rare finding of these casts is considered physiological. Lindner, Haber, and others have described the type I granular casts as a cast embedding cellular debris. This type I cast has a variable size granulation with a clumpy distribution. The leukocytes origin of the debris is suspected, but our attempt to stain these casts with the Naphtyl AS-D Chloro-acetate esterase gave deceiving results. We think that these casts are made of cellular debris of different kinds including degenerated leukocytes. The term "cellular debris cast" would be more appropriate and less confusing than the type I granular casts.
The dirty brown color is due to pigments present within the granulation. These pigments seem to be oxydative degradation products of hemoglobin like methemoglobin and other products. The color is quite similar to air-exposed dried blood.
The presence of large brown colored casts, alone, without any other anomaly, is suspicious. The context is very important in identification. Dirty brown casts are normally accompanied by hematuria, cellular casts, several tubular cells, often necrotic and pigmented and, if stasis is not recent, waxy casts. These casts must not be confused with plain hyaline casts rolled in amorphous urates. The dirty brown casts are associated with acute tubular necrosis. This tubular necrosis is often of ischemic nature. These casts can also be seen in cases of massive intravascular hemolysis leading to renal failure.
Yeast—Schumann, using the PAP staining procedure, has demonstrated the importance of the identification of the yeast casts. These casts are usually found in specimens of immunosuppressed patient. Yeast casts are also a very important finding in the diabetic patients. With immunosuppressed patients the route of introduction is usually the blood. Reflux with a yeast infected urine is also a possible route of entry, specially with the diabetic patient. The "Candida" casts are described, by Schumann, as casts with a rather waxy matrix with yeast inclusions. As for bacteria casts, cell inclusions, specially white blood cells, are expected. Crystal casts are defined as a hyaline matrix casts with inclusions of crystals. The presence of these casts indicates an intratubular crystallization. This crystallization can provoke renal damages. These damages can be created by an inflammation process or by obstruction. The sediment with crystal casts will usualy show other figures like renal tubular cells and other casts.
This section is dedicated to special rare casts. Fibrin thread casts—These casts are hyaline casts embedding, within their matrix, fibrin threads. These threads originate from the passage in the urinary space, of the coagulation proteins (fibrinogen and others). Once in urine, the fibrinogen coagulates and forms fibrin threads. These casts are strongly indicative of glomerulonephritis.
|
||||||||||||||||||||||||||||||||
 The
hyaline matrix—The hyaline matrix is by
far the most frequently observed. Hyaline casts, that is hyaline
matrix casts without inclusion, are seen in numerous conditions.
Some of these conditions are the results of a pathological
process, but many are results of a normal physiological activity.
Hyaline casts can be seen after a strenuous exercise. Hyaline
casts are considered as physiological casts. A count of 1000
or less hyaline casts in a 24-hour specimen is a normal value.
The
hyaline matrix—The hyaline matrix is by
far the most frequently observed. Hyaline casts, that is hyaline
matrix casts without inclusion, are seen in numerous conditions.
Some of these conditions are the results of a pathological
process, but many are results of a normal physiological activity.
Hyaline casts can be seen after a strenuous exercise. Hyaline
casts are considered as physiological casts. A count of 1000
or less hyaline casts in a 24-hour specimen is a normal value.



 The
waxy matrix—The waxy casts owe their name
to the opaque waxlike matrix. Waxy casts have square ends and
have frequent notch like cracks perpendicular to the long axis.
This matrix is related to a long period urinary stasis affecting
some nephrons. Waxy casts are usually without inclusion or
slightly granular, but waxy casts with inclusions are occasionally
seen. An example of a waxy cellular cast is shown in this link
pictures collection. We think that all the inclusions seen
in a hyaline matrix are possible within the waxy matrix.
The
waxy matrix—The waxy casts owe their name
to the opaque waxlike matrix. Waxy casts have square ends and
have frequent notch like cracks perpendicular to the long axis.
This matrix is related to a long period urinary stasis affecting
some nephrons. Waxy casts are usually without inclusion or
slightly granular, but waxy casts with inclusions are occasionally
seen. An example of a waxy cellular cast is shown in this link
pictures collection. We think that all the inclusions seen
in a hyaline matrix are possible within the waxy matrix.

 Red
blood cells casts are described as hyaline casts, containing
ghost red blood cells, or as hyaline casts filled with numerous
orange red erythrocytes. The unpigmented form of red blood
cells casts is more frequent. Care must be taken not to confuse
red blood cells casts with RBC coated mucus threads mimic casts.
This situation will usually also show similar structures with
completely different shapes.
Red
blood cells casts are described as hyaline casts, containing
ghost red blood cells, or as hyaline casts filled with numerous
orange red erythrocytes. The unpigmented form of red blood
cells casts is more frequent. Care must be taken not to confuse
red blood cells casts with RBC coated mucus threads mimic casts.
This situation will usually also show similar structures with
completely different shapes. The
true blood casts have a matrix resembling to the waxy casts;
the square ends and the typical notchs are frequently seen.
The color is the typical orange red, and the texture is homogenous
and rather granular. Identifiable red blood cells are rare.
In typical cases, it is not rare to see cast fragments that
would easily be unnoticed in some other situations.
The
true blood casts have a matrix resembling to the waxy casts;
the square ends and the typical notchs are frequently seen.
The color is the typical orange red, and the texture is homogenous
and rather granular. Identifiable red blood cells are rare.
In typical cases, it is not rare to see cast fragments that
would easily be unnoticed in some other situations. The
tubular cells seen in casts are usually from the collecting
tubes, but cells originating from the proximal tubules or any
other sections (prior to the collecting tubes) of the nephron
is possible. With the PAP stain, Schumann subdivides renal
tubular cell casts in RTC cast and necrotic RTC casts.
The
tubular cells seen in casts are usually from the collecting
tubes, but cells originating from the proximal tubules or any
other sections (prior to the collecting tubes) of the nephron
is possible. With the PAP stain, Schumann subdivides renal
tubular cell casts in RTC cast and necrotic RTC casts. For
the microscopist, the identification of white blood cell cast
is often a challenge. Casts of this type are often mixed and
the plurilobulate of cells is not always visible, even in phase
contrast. Because of the clinical significance of these casts,
it is necessary to make some identification efforts, like using
special stains. As for the distinction between the cellular
casts and the renal tubular cell fragments, it is sometimes
difficult to establish if we are dealing with a real leukocytes
cast or with a cluster of leukocytes distributed as a cast
(pseudocasts). The presence of a matrix is a criterion.
For
the microscopist, the identification of white blood cell cast
is often a challenge. Casts of this type are often mixed and
the plurilobulate of cells is not always visible, even in phase
contrast. Because of the clinical significance of these casts,
it is necessary to make some identification efforts, like using
special stains. As for the distinction between the cellular
casts and the renal tubular cell fragments, it is sometimes
difficult to establish if we are dealing with a real leukocytes
cast or with a cluster of leukocytes distributed as a cast
(pseudocasts). The presence of a matrix is a criterion.


 Macrophages
containing casts is not a rare figure. The casts are often
reported as cellular casts. The main reason is due to the fact
that macrophages are rarely recognizable. These casts are frequent
in the urinary sediment of hepatic patient. In this context,
the cells are large (too large for RTC) and stained by the
bilirubin. Staining with the naphtyl AS-D chloroacetate esterase
method will demonstrate some large positive cells definitively
not leukocytes.
Macrophages
containing casts is not a rare figure. The casts are often
reported as cellular casts. The main reason is due to the fact
that macrophages are rarely recognizable. These casts are frequent
in the urinary sediment of hepatic patient. In this context,
the cells are large (too large for RTC) and stained by the
bilirubin. Staining with the naphtyl AS-D chloroacetate esterase
method will demonstrate some large positive cells definitively
not leukocytes.

 Granular
casts (type II) are described by Lindner as hyaline matrix
casts filled with granules similar to cytoplasmic degeneration
granules. There is a relation between the structure of these
granules and the granular cytoplasm of the degenerating tubular
cells. The causes of this degeneration are unknown, but a proteinuria
is a usual finding. A protein overload could be responsible
for the granular degeneration of the tubular cells. The cytoplasm
granulation could then be integrated in a cast as free granules,
as cytoplasmic fragments, or as complete cells.
Granular
casts (type II) are described by Lindner as hyaline matrix
casts filled with granules similar to cytoplasmic degeneration
granules. There is a relation between the structure of these
granules and the granular cytoplasm of the degenerating tubular
cells. The causes of this degeneration are unknown, but a proteinuria
is a usual finding. A protein overload could be responsible
for the granular degeneration of the tubular cells. The cytoplasm
granulation could then be integrated in a cast as free granules,
as cytoplasmic fragments, or as complete cells. Many
of the granular casts, when stained with PAP method, will show
some nucleus remnants and therefore, can be considered as a
cellular cast. These nuclear residues are not visible with
unstained specimens under bright field microscopy. In this
condition, the cast shows a homogenous granular texture typical
of the type II granular cast.
Many
of the granular casts, when stained with PAP method, will show
some nucleus remnants and therefore, can be considered as a
cellular cast. These nuclear residues are not visible with
unstained specimens under bright field microscopy. In this
condition, the cast shows a homogenous granular texture typical
of the type II granular cast. These
coarsely granular casts are special by their dirty red-brown
colorations (burnt umber). The casts are rather large and heavily
pigmented from brown to almost black. The matrix is hyaline,
with frequently one end larger than the other.
These
coarsely granular casts are special by their dirty red-brown
colorations (burnt umber). The casts are rather large and heavily
pigmented from brown to almost black. The matrix is hyaline,
with frequently one end larger than the other. The
dirty brown color is not always easy to distinguish from the
orange red color of blood casts. The drawing is an attempt
to show the color difference between these.
The
dirty brown color is not always easy to distinguish from the
orange red color of blood casts. The drawing is an attempt
to show the color difference between these.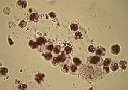



 Does
someone have any idea about this cast? Casts like this one
were observed a few times in patients with acute renal failure.
Cellular casts, waxy casts, and many tubular cells were also
found in all the cases.
Does
someone have any idea about this cast? Casts like this one
were observed a few times in patients with acute renal failure.
Cellular casts, waxy casts, and many tubular cells were also
found in all the cases.