Ed Friedlander, M.D., Pathologist
scalpel_blade@yahoo.com



Cyberfriends: The help you're looking for is probably here.
Welcome to Ed's Pathology Notes, placed here originally for the convenience of medical students at my school. You need to check the accuracy of any information, from any source, against other credible sources. I cannot diagnose or treat over the web, I cannot comment on the health care you have already received, and these notes cannot substitute for your own doctor's care. I am good at helping people find resources and answers. If you need me, send me an E-mail at scalpel_blade@yahoo.com Your confidentiality is completely respected.
 DoctorGeorge.com is a larger, full-time service.
There is also a fee site at myphysicians.com,
and another at www.afraidtoask.com.
DoctorGeorge.com is a larger, full-time service.
There is also a fee site at myphysicians.com,
and another at www.afraidtoask.com.
Translate this page automatically
 |
With one of four large boxes of "Pathguy" replies. |
 I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
Numbers in {curly braces} are from the magnificent Slice of Life videodisk. No medical student should be without access to this wonderful resource. Someday you may be able to access these pictures directly from this page.
Also:
Medmark Pathology -- massive listing of pathology sites
Freely have you received, freely give. -- Matthew 10:8. My
site receives an enormous amount of traffic, and I'm
handling about 200 requests for information weekly, all
as a public service.
Pathology's modern founder,
Rudolf
Virchow M.D., left a legacy
of realism and social conscience for the discipline. I am
a mainstream Christian, a man of science, and a proponent of
common sense and common kindness. I am an outspoken enemy
of all the make-believe and bunk that interfere with
peoples' health, reasonable freedom, and happiness. I
talk and write straight, and without apology.
Throughout these notes, I am speaking only
for myself, and not for any employer, organization,
or associate.
Special thanks to my friend and colleague,
Charles Wheeler M.D.,
pathologist and former Kansas City mayor. Thanks also
to the real Patch
Adams M.D., who wrote me encouragement when we were both
beginning our unusual medical careers.
If you're a private individual who's
enjoyed this site, and want to say, "Thank you, Ed!", then
what I'd like best is a contribution to the Episcopalian home for
abandoned, neglected, and abused kids in Nevada:
My home page
Especially if you're looking for
information on a disease with a name
that you know, here are a couple of
great places for you to go right now
and use Medline, which will
allow you to find every relevant
current scientific publication.
You owe it to yourself to learn to
use this invaluable internet resource.
Not only will you find some information
immediately, but you'll have references
to journal articles that you can obtain
by interlibrary loan, plus the names of
the world's foremost experts and their
institutions.
Alternative (complementary) medicine has made real progress since my
generally-unfavorable 1983 review linked below. If you are
interested in complementary medicine, then I would urge you
to visit my new
Alternative Medicine page.
If you are looking for something on complementary
medicine, please go first to
the American
Association of Naturopathic Physicians.
And for your enjoyment... here are some of my old pathology
exams
for medical school undergraduates.
I cannot examine every claim that my correspondents
share with me. Sometimes the independent thinkers
prove to be correct, and paradigms shift as a result.
You also know that extraordinary claims require
extraordinary evidence. When a discovery proves to
square with the observable world, scientists make
reputations by confirming it, and corporations
are soon making profits from it. When a
decades-old claim by a "persecuted genius"
finds no acceptance from mainstream science,
it probably failed some basic experimental tests designed
to eliminate self-deception. If you ask me about
something like this, I will simply invite you to
do some tests yourself, perhaps as a high-school
science project. Who knows? Perhaps
it'll be you who makes the next great discovery!
Our world is full of people who have found peace, fulfillment, and friendship
by suspending their own reasoning and
simply accepting a single authority that seems wise and good.
I've learned that they leave the movements when, and only when, they
discover they have been maliciously deceived.
In the meantime, nothing that I can say or do will
convince such people that I am a decent human being. I no longer
answer my crank mail.
This site is my hobby, and I presently have no sponsor.
This page was last updated February 6, 2006.
During the ten years my site has been online, it's proved to be
one of the most popular of all internet sites for undergraduate
physician and allied-health education. It is so well-known
that I'm not worried about borrowers.
I never refuse requests from colleagues for permission to
adapt or duplicate it for their own courses... and many do.
So, fellow-teachers,
help yourselves. Don't sell it for a profit, don't use it for a bad purpose,
and at some time in your course, mention me as author and KCUMB as my institution. Drop me a note about
your successes. And special
thanks to everyone who's helped and encouraged me, and especially the
people at KCUMB
for making it possible, and my teaching assistants over the years.
Whatever you're looking for on the web, I hope you find it,
here or elsewhere. Health and friendship!
God is great, God is good,
-- Bart Simpson
Give a little love to a child, and you get great deal back.
We have enough youth. How about a fountain of SMART?
Learning Objectives
Define the following terms, and supply them given a definition:
Cite the principal factors that we believe are responsible for small-for-gestational-age infants.
Explain why immature lungs are unsatisfactory for gas exchange.
Mention two reasons why otherwise-healthy newborns are often jaundiced. Cite two diseases from
this unit that present as severe or prolonged neonatal jaundice. Mention the upper "safe" bilirubin
levels for term babies (20 mg/dL), and the effect of prematurity on this level (lowers it).
Recognize the common types of birth injury. List factors contributing to, and kinds of, head injuries
during birth.
Distinguish deformations and malformations, and recall that they affect 2% and 3% of newborns
respectively. Recall malformations as the major non-preventable cause of infant mortality in the
U.S.
Name the two viruses that are held responsible for many congenital malformations (CMV, rubella).
Recall deafness, cardiac malformations, and cataract as "rubella syndrome", and recall the first 16
weeks after conception as the risk period for rubella infection.
Explain the mechanics of "uterine constraint" during the 35th-38th weeks.
Describe hydrops fetalis and some of its causes.
Describe neonatal asphyxia and list the major factors that cause it.
# Give a complete account of hemolytic disease of the newborn, and identify ABO incompatibility
(not Rh) as its most common cause today.
Describe in some detail the pathogenesis, diagnosis and treatment of phenylketonuria. Describe its
effects on intelligence, and explain the hypopigmentation.
Describe the pathogenesis, abnormal anatomy, clinical picture, diagnosis and treatment of
galactosemia (transferase deficiency). Recognize galactokinase deficiency as a mild form producing
cataracts.
Give a complete account of cystic fibrosis ("mucoviscidosis"). List its mode of inheritance, its
frequency among whites and non-whites, and the location of the gene. Describe the fundamental
defect, the pathophysiology of the sweat test, the nature of meconium ileus, and the effect of the
disease on the sweat, lungs, exocrine pancreas, and hepatobiliary system. Describe the effect of
cystic fibrosis on the whole person, and give the current life expectancy.
# Briefly describe the following tumors and tumor-like conditions of the young:
hemangiomas
# Recognize the common childhood tumors for various ages. Recall acute
lymphoblastic leukemia as causing more death in children under age 15 than all other cancers
combined.
Recognize the following under the microscope:
pancreas in end-stage cystic fibrosis
NOTE: We will discuss RDS and SIDS under "Respiratory".
QUIZBANK Pediatric (all)
Year II's: I know much of this is repetitious from other lectures and other courses. This creates a
dilemma for me -- I don't like repeating material from other courses, and I don't like leaving you
with chunks of "objectives" for which there is no handout text. Items with a "#" are those that
I
believe you already know from this or other courses, or will hear about at length in "Obstetrics" and
"Pediatrics", but that you might profitably review at this time.
 I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
Pathology Education Instructional Resource -- U. of Alabama; includes a digital library
Houston Pathology -- loads of great pictures for student doctors
Pathopic -- Swiss site; great resource for the truly hard-core
Syracuse -- pathology cases
Walter Reed -- surgical cases
Alabama's Interactive Pathology Lab
"Companion to Big Robbins" -- very little here yet
Alberta
Pathology Images --hard-core!
Cornell
Image Collection -- great site
Bristol Biomedical
Image Archive
EMBBS Clinical
Photo Library
Chilean Image Bank -- General Pathology -- en Español
Chilean Image Bank -- Systemic Pathology -- en Español
Connecticut
Virtual Pathology Museum
Australian
Interactive Pathology Museum
Semmelweis U.,
Budapest -- enormous pathology photo collection
Iowa Skin
Pathology
Loyola
Dermatology
History of Medicine -- National Library of Medicine
KU
Pathology Home
Page -- friends of mine
The Medical Algorithms Project -- not so much pathology, but worth a visit
National Museum of Health & Medicine -- Armed Forces Institute of Pathology
Telmeds -- brilliant site by the medical students of Panama (Spanish language)
U of
Iowa Dermatology Images
U Wash
Cytogenetics Image Gallery
Urbana
Atlas of Pathology -- great site
Visible
Human Project at NLM
WebPath:
Internet Pathology
Laboratory -- great site My team:
My team:Ed Lulo's Pathology Gallery
Bryan Lee's Pathology Museum
Dino Laporte: Pathology Museum
Tom Demark: Pathology Museum
Dan Hammoudi's Site
Claude Roofian's Site
Pathology Handout -- Korean student-generated site; I am pleased to permit their use of my cartoons
Estimating the Time of Death -- computer program right on a webpage
Pathology Field Guide -- recognizing anatomic lesions, no pictures

St.
Jude's Ranch for Children
I've spent time there and they are good. Write "Thanks
Ed" on your check.
PO Box 60100
Boulder City, NV 89006--0100
More of my notes
My medical students
Clinical
Queries -- PubMed from the National Institutes of Health.
Take your questions here first.
HealthWorld
Yahoo! Medline lists other sites that may work well for you

We comply with the
HONcode standard for health trust worthy
information:
verify
here. 

![]()
Get me through my childhood!
Adults are obsolete children.
-- Dr. Seuss
-- John Ruskin
-- Anonymous
 Georgetown Med School
Georgetown Med School
Pediatric Pathology
Lots of cystic fibrosis
# anencephaly
aniridia / WT-1 complex
# "appropriate for gestational age" (i.e., not large or small)
# brachydactyly (i.e., short fingers / toes)
bronchiectasis
caput succedaneum
cephalhematoma
# Coombs test (direct, * indirect)
# D (major Rh isomorphism)
deformation
# erythroblastosis fetalis
# hydrops fetalis (i.e., massive edema of fetus)
# hypospadias
infancy
# kernicterus (i.e., brain damage from baby jaundice)
"large for gestational age"
major malformation
malformation
meconium ileus
neonatal period
# neural tube defect ("spina bifida")
oligohydramnios sequence
perinatal (neonatal) asphyxia
polydactyly (i.e., extra fingers / toes)
post-term
pre-term
# Rhogam (anti-D immunoglobulin)
"small for gestational age"
# syndactyly (i.e., fused fingers, did you see Danny DeVito as "the Penguin"?)
 Cite the leading causes of death during the neonatal period, infancy, 1-4 years, and 4-15 years.
Cite the leading causes of death during the neonatal period, infancy, 1-4 years, and 4-15 years.
lymphangioma ("cystic hygroma")
sacrococcygeal teratoma
vaginal adenosis and adenocarcinoma
peripheral smear in hemolytic disease of the newborn
Pancreas #'s 1-8 (cystic fibrosis)
From childhood's hour I have not been
As others are; I have not seen
As others saw; I could not bring
My passion from the common spring.
From the same source I have not taken
My sorrow; I could not awaken
My heart to joy at the same tone,
And all I loved, I loved alone.
Thus, in my childhood, at the dawn
Of a most stormy life, was drawn
From every spring of good or ill
The mystery that binds me still...
-- Edgar Allen Poe, fragment
INTRODUCTION
|
|
|
|
Embryo: An unborn child / product of conception with child parts for the first eight weeks after the
moment of conception
Fetus: An unborn child / product of conception with child-parts (rather than just placenta), between
eight weeks after conception and the moment of live birth ("all-the-way-out with a beating heart" for
our lawyer friends).
Neonate: A child in the first four weeks of life after birth.
Infant: A child in the first year of life after birth. Infant mortality: For a population, how many of
its people per 1000 live births die before their first birthday.
In the US during the 1990's, it was about 7 out of 1000 babies (CMAJ 163:
497, 2000). In the mid-1900's, in the "developing world", which was most places,
infant mortality rates were around 300-400 per 1000. Today there are only 16 nations
where it is above 100; Mozambique is highest with 199, and Afghanistan is fourth with 142 (CIA 2004)
The scandal of infant mortality in the U.S., especially among poor black people: NEJM 327: 1022,
1992. Ten percent of babies born to black mothers receiving no prenatal care are very-low birth
weight (see below). Wall St. J. tells it like it is 1/20/92, quoted in Pediatrics 92: A74, 1993.
Overall neonatal mortality is dropping, but the racial disparity remains:
Am. J. Epidem. 154: 307, 2001.
Worldwide, reported infant and child mortality figures ("ten million children
die each year, almost all of them poor": Lancet 362: 323, 2003) are likely to be
much lower than the real numbers,
because deaths are not reported. The governments do not care, and do
not want the stigma of a high number, since it's obvious that they are not
providing the simple interventions that could prevent most of the deaths
(Lancet 362: 65, 2003).
Pre-term: Born before 37-38 weeks. About one
birth in ten in the US is preterm. Review Am. Fam. Phys. 57:
2457, 1998)
The etiology is often obscure. There are many statistical correlations,
few "why"'s that make sense...
Right now, a "usual suspect" is corticotropin releasing
hormone ("from stress")
causing prostaglandin production that in turn
causes the uterus to empty. CRF levels are probably high long before
the preterm labor. This makes sense, and might
explain why glucocorticoid administration seems to help stop the process.
See Am. J. Ob. Gyn. 186: 257, 2002;
Science 304: 666, 2004.
A group of pathologists has finally gotten up a
study of placentas from preterm deliveries, and not surprisingly
discovered that babies
whose placentas display ischemia or infection
did worse than babies with "idiopathic preterm labor"
(Ob. Gyn. 94: 284, 1999).
Nowadays a child born at 22 weeks will almost certainly die in the first six months.
A child born at 23 weeks might survive but will almost certainly be profoundly brain damaged.
A child born at 25 weeks has about a 3/4 chance of making it to six months and a better-than-half
chance of not having gross brain damage on ultrasound (don't believe me, read all about it in NEJM
329: 1597, 1993).
Even preterm children born later are very likely to have serious
disabilities as a result: NEJM 343: 378, 2000.
Today's neonatologists are now talking about ethically unjustifiable
interventions that maintain life without awareness (we may hope) or any
ability to interact with others (obvious). Yet it is still
common for children to be kept alive into the teenaged years,
often on respirators and requiring round-the-clock nursing,
often in status epilepticus. The economics of all of this is complicated,
and ideology gets involved.
The story of the far-right
Baby Jane Doe laws, which were eventually overturned
by the Supreme Court, makes disturbing reading.
In the US, during most of the 1900's, such a child would impoverish the family,
and earn lots of third-party money for the hospital.
Nowadays,
physicians here and overseas point out that these
children consume resources that could go for children with better
prognosis (or for profits), and are even making veiled criticisms of
parents who demand that such
children be kept alive (Lancet 355: 2112, 2000).
Post-term: Both after 42 weeks.
Small for gestational age ("small for dates"): Below 10th percentile on the charts. The child did not
grow properly in the uterus, and the organs will have extra problems once the child is born....
Problems with the unborn child itself
Chromosomal problems
Congenital infections ("torch")
Toxoplasmosis
Other (syphilis, etc.)
Rubella
Cytomegalovirus
(Herpes, the "H", is usually not an intra-uterine infection)
(Listeria, which like syphilis passes through the placenta,
is less likely to produce actual deformities, though it can be very
deadly)
Other congenital anomalies
Being conceived by the new reproductive technologies (?? doubles the risk
even when you control for twinning ?? NEJM 346: 731, 2002)
Problems with the placenta or uterus
Infarcts
Tumors
The thrombophilias (clots in the spiral arteries and between the
villi of the placenta): Big news. NEJM 340: 9, 1999.
Etc., etc.
Problems with Mother
Cocaine ("crack babies")
Tobacco
Opiate abuse
Alcoholism
Toxemia and other hypertension
Large for gestational age: Above 90th percentile on the charts. Think of maternal diabetes.
Low birth weight: As it sounds; a mix of "small for gestational age" and
"preterm". Caring for tiny
babies is expensive, and the outcomes uncertain; statistics are hard to find, but . At school age,
surviving low birth-weight children still show signs of damage in all health parameters except
happiness (JAMA 267: 2204, 1992; same findings JAMA 289: 3264, 2003).
Low birth weight: <2500 gm
Very low birth weight: <1500 gm
One third of infants that die are very low birth weight infants. Another third are low birth weight
infants. The remaining third are of normal weight (NEJM 327: 1022, 1992).
Although survival of low-birthweight kids has improved tremendously (thanks largely to surfactant
administration), there has been no decrease in the numbers of these kids, and it remains closely linked
to underclass status (Am. J. Pub. Health 85: 909, 1995). Survivors often need expensive long-term
care (lung failure, brain damage).
*The Oregon Plan ranked extraordinary life support for very-low birth-weight Medicaid babies as
the second-from-the-bottom on a list of "where does the health care dollar do the most life-enhancing
good". Due to right-wing political pressure, the Bush administration decided (1992) that this
constituted "discrimination against the handicapped", and the rest is history (Hastings Center
Reports 22(6): 21, Nov.-Dec. 1992).
Nowadays, even conservative sources talk freely about "societal
concerns about the ethics and justification of intensive care for
these infants" (JAMA 281: 799, 1999).
*You will often hear the claim that "prenatal care prevents low-birth-weight". Lately a group at
Ann Arbor studied women in the U.S. (where there's bureaucratic red-tape for a poor pregnant
woman to get care) and Canada (where care's basically free and expected.) Poverty (i.e.,
underclass behaviors), not care, was
the overriding risk factor for low-birth-weight (Am. J. Pub. Health 84: 986, 1994); I wish they'd
sorted out the pre-term and the small-for-gestational-age kids.
Uterine constraint to some extent was experienced by most of us beginning around our 35th week of
intrauterine life. It's likely to be bad if the uterus is small, bicornuate, or loaded with fibroids, or if
we shared quarters with a twin, had oligohydramnios (i.e., too little amnionic fluid, i.e., no kidneys,
placental insufficiency, or a slow leak), or if we were positioned badly.
If we were molded out of shape as a result of uterine constraint, we suffered a deformation (as
opposed to a "malformation", and generally not so ominous; 2% of kids get a significant
deformation). Most famous is oligohydramnios sequence, with squashed ("Potter's") face and badly
bent limbs.
Arthrogryposis ("joint claws") usually refers to
a congenital situation with muscle contractures present at birth,
is a relatively common, non-progressive symptom that can
result from uterine constraint, CNS disease, or failure of
certain muscles to develop.
A variation on the theme of uterine constraint is the typical
deformities (club feet, withered arms, Mobius)
caused by uterine contractions in Latin American
women who take
prostaglandin because abortion is illegal (Lancet 351:
1624, 1998).
Malformations result from chromosomal problems, genes of large effect, deletions of chunks of a
chromosome, polygenic problems, or "just happen". They range from familiar, correctable problems
like mild hypospadias to dread, lethal conditions like anencephaly.
Occasionally the cause is more or less clear; timing is important. Around 3% of kids have a
malformation that's at least of serious cosmetic importance (i.e., "a major malformation").
The syndromes caused by deletions of chunks of chromosome are just now being characterized.
Worth remembering: WT-1 complex (* formerly WAGR): Wilms' tumor, aniridia (no iris), growth
problems).
Here's a list of the common congenital malformations and their
approximate frequencies:
Hydrops fetalis is severe edema of the fetus.
Neonatal asphyxia is an important cause of death and brain damage in babies.
Causes:
Placental problems
Placenta previa (i.e., a low-slung placenta overlying the os)
Abruption (i.e., a big bleed between placenta and uterine wall)
Cord problems
Compression (around neck, breech delivery, etc., etc.)
Other (poorly-understood)
Toxemia
Prolonged rupture of the membranes
Chorioamnionitis
Etc.
In fatal cases, the pathologist looks for squamous cells in the alveoli, meconium staining of the skin,
and hyaline membranes in the alveoli (rather than the terminal bronchioles), as well as evidence of
the exact mechanism in the cord, placenta, or dead child.
Birth injuries:
Cephalhematoma: Hemorrhage under the scalp
("subgaleal hematoma"). Trivial; no known risks worth remembering.
Caput succedaneum: Edema of the scalp where the head was pressed against the opening cervix.
Trivial; no known risks worth remembering.
Intracerebral hemorrhages from dural sinuses or brain substance. The most important birth injury.
Devastating.
{17430} intracerebral hemorrhage (this was a bleed into the ventricles from the subependymal
germinal plate)
Upper extremity injuries: Fractured clavicle, brachial plexus injury (Erb's palsy, etc., etc.), fractured
humerus
Facial nerve injury: Often from forceps (happened
to Silvester Stallone)
Skull fractures often result from prolonged labor where there is cephalopelvic disproportion, or from
precipitous labor, or from inexpert use of the forceps.
Eight hours to two days: Some skin slipping and peeling
Two to seven days: Extensive skin peeling. There may be red-stained
pleural and peritoneal effusions.
More than seven days: Liver is yellowish; body may be mummified
CHILDHOOD MORTALITY
In the U.S., around 1 newborn in 60 does not reach age 15. The majority of these are due to birth
defects and prematurity. A significant minority (around 1 in 300) will die in an "accident"; the true
number of deaths from "SIDS" and child abuse is probably similar (one kid in 6 coming to the
emergency room is there because of injuries inflicted by an adult). Cancer kills around 1 child in
2000.
Child abuse may be reasonably defined to be harsh treatment of a child sufficient to interfere with
the child's functioning.
Everybody knows about the cycle from generation to generation. Of child abuse victims, 1/3 will
never abuse their own children, 1/3 will abuse their children with little provocation, and 1/3 may
abuse their children when they, themselves, are stressed. It is simplistic to say either "it's willful
misbehavior" or "it's society's fault". Am. J. Psych. 150: 1315, 1993.
There are about 900 child-abuse murders in the US yearly; 65% of the
assailants are men, 62% of the assailants are biological parents,
and
black children are killed at three times the rate of while children (JAMA 282:
463, 1999).
Here are the twelve most common explanations offered by abusers, as compiled
by the late Robert Kirschner MD of Cook County:
What concerns me about this list that it's just possible, in any particular
case, that the explanation could be true. This is what makes prosecutions
so problematic. Thankfully, there are usually other inconsistencies and/or other
evidence of abuse.
* Pathologists may estimate the duration of the
abuse by studying the
thymic cortex ("stress"). See For. Sci. Int. 53: 69,
1992.
The table in "Big Robbins" lists statistics that may be misleading. Here's what you need to know.
The major killers of neonates and infants are prematurity and birth defects. Around 1.3% of US
newborns die from these causes. The U.S. is around 18th in the world; the 17 nations that do
better have fewer % poor / underclass and better access to health care. Among our own underclass, infant
mortality was actually during the 1990's; it's now dropping some.
Birth defects cause death in abound 1 in 350 kids during the first
year of life (Ob. Gyn. 98: 620, 2001). Numbers from around the world
are variable; abortion of defective babies has dropped the overall infant
mortality rate in Canada by about 20% (JAMA 287: 1561, 2002).
In-vitro fertilization / intracytoplasmic sperm injection
is reported to double the risk of a major birth
defect: NEJM 346: 725, 2002)
Also worth noting: "Sudden infant death syndrome" kills up to 0.5% of infants during the first year
of life; the rate varies tremendously from community to community and from pathologist to
pathologist.
The real prevalence of infanticide is unknown and controversial; at least some are overlooked as
"accidents" or "SIDS". The incidence is probably even higher in the Third World (even among
"noble savages", and some cultures make no attempt to conceal it, even from the U.S. Left:
Science
261: 987, 1993). Killing of little girls in Mainland China ("the people's paradise"): Child.
Psych. 23: 53, 1992. At least 1 child in 50,000 in the U.S. is killed or abandonned
at birth by their mothers: JAMA 289: 1425, 2003; society is starting to notice
and to respond with Safe Haven laws.
The perinatal autopsy: JAMA 273: 59, 1995.
Ages 1-14: "Accidents" are the leading cause of death, outranking each category of disease by a
substantial margin.
Child abuse and neglect (apparently included among "other" in "Big Robbins") is an important killer
among children. Again, the true prevalence is unknown and is controversial -- at least some are
overlooked ("accidents" or "sudden infant death syndrome").
{39145} sirena ("mermaid baby"; lower extremities are fused)
Older teens: The ranked causes of death...
Males: (1) "Accidents"
(2) Homicide (this might be first now)
(3) Suicide
Females: (1) "Accidents"
(2) Cancer
(3) Homicide (this recently surpassed suicide)
Most sources will give you these or similar statistics.
During the past quarter-century, the homicide rate for kids increased about 70%; this is almost
entirely teens shooting other teens (Pediatrics 97: 791, 1996;
JAMA 280: 423, 1998; Acad. Emerg. Med. 4: 248, 1997).
This is largely
but not entirely among African-Americans and Hispanic Americans; rates
have dropped by almost half
since the mid-1990's: Prev. Med. 27: 452, 1998.
Suicide remains rampant among American Indian teens
(Soc. Sci. Med. 53: 1115, 2001; Lancet 355: 906, 2000;
Arch. Ped. Adol. Med. 153: 573, 1999).
IMMATURITY: Please review the section in "Big Robbins" if you are interested in knowing how
newborns' tissues differ from other folks'.
Lungs:
20 weeks: The large airways end in blind pouches, never reaching the mesenchyme where alveoli
will form. This sets the famous "lower limit" on the age at which a child can survive outside the
womb.
26 weeks: Alveolar type epithelium (type I and II pneumocytes) starts to form
Kidney: Remember you'll see glomeruli still forming under the capsule in a term infant. (Future
pathologists: Look closely at this "blastema"; Wilms' tumor will recapitulate it.)
Brain: Very soft in the newborn, but adequate for homeostasis. Preemies have trouble coordinating
their autonomic nervous system functions. Even in the term infant, the gyri are still forming, and
many centers lack myelin.
Liver: Getting born jolts the liver into activity after a few days, but during the process, newborns
almost all become a bit jaundiced (inadequate glucuronyl transferase at birth). This is worse in
smaller babies and especially preemies.
Adrenal: Don't expect to see the usual three cortical layers in a newborn. It's mostly the "fetal zone",
which involutes during infancy.
GALACTOSEMIA
Two autosomal recessive inborn errors of metabolism, one mild, one severe. Both feature elevated
blood galactose. These are often confused, and tend to get missed during classical pathology
courses, and are discussed here.
The not-so-bad kind of galactosemia is caused by lack of galactokinase. Kids get cataracts only
(probably from galactitol, by analogy with the sorbitol cataract of the diabetic).
{18241} galactosemia cataract
The bad kind of galactosemia is caused by galactose-1-phosphate uridyl transferase deficiency.
Probably it's galactilol that causes the cerebral edema
and brain damage (J. Ped. 138: 260, 2001).
Fortunately this is rare (maybe 1 in 40,000 kids), and all 50 states
screen newborns.
The classic story is a child is born normal, is fed milk, and fails to thrive. Jaundice, diarrhea,
vomiting, and sleepiness develop. They are followed by enlargement of the liver and spleen, failure
of the liver (biopsy shows fatty change, cholestasis with the liver cells arranged around bile plugs
like flower petals, and eventually cirrhosis) and by the development of cataracts. Finally somebody
notices that "Clinitest" shows "sugar in the urine", but "the dipstick" doesn't.
{20137} liver in galactosemia, architecture isn't normal
Eventually, there is multi-system failure. The proximal tubular cells fail ("Fanconi syndrome", with
aminoaciduria), and the leukocytes fail to control bacteria, with gram-negative sepsis a common
mechanism of death. In adults who survived galactosemia, the ovaries tend to have atrophied.
Affected kids are taken off milk, with improvement in their labs and liver histology, and arrest of the
disease. There is not, unfortunately, reversal of the brain damage that has already occurred.
The allele itself seems to have at least as much to do with the
severity of the long-term brain damage as does the effort made to keep
the disease under control after diagnosis. See Arch. Dis. Child.
83: 248, 2000.
* Distinctive for survivors is "verbal dyspraxia", i.e., the inability to coordinate the elements of
speech ("nose" may be pronounced "zone", "music" may become "mukis", and words are
scrambled). Read about it in Pediatrics 88: 346, 1991.
CYSTIC FIBROSIS ("CF", "mucoviscidosis"; Lancet 361: 681, 2003)
This common white-peoples' genetic disease (1/2500 births) is caused by homozygous lack of a
membrane component essential to proper chloride transport across membranes of the mucus-producing exocrine glands and eccrine
sweat glands in response to cAMP.
The disease is named for changes in the pancreas and mucous salivary glands, which have their
ducts plugged by viscous mucus. "Cysts" form behind the plugs, and "fibrosis" ensues after years of
obstruction.
Heterozygotes have minimal symptoms (i.e., they are a bit more wheezy than normals, on the
average; see Thorax 42: 120, 1987), and it's been known for years
that they enjoy a relative
resistance to chloride-secreting gram-negative intestinal infections, allowing natural selection for the
gene. And surprise! CFTR is the typhoid
bug receptor, homozygotes are completely immune, heterozygotes
much protected Nat. Med. 4: 663, 1998).
The disease is rare in black or oriental children.
The locus for the disease (chromosome 7q), its normal product, and their place in biology have
recently been discovered (Science 245: 1059, 1066 & 1073, 1989; Thorax 45: 46, 1990; Science
256: 774, 1992).
In health, increasing cAMP levels open ("activate") the apical chloride channels in the airway
epithelium. This causes chloride to flow out, and water follows. In cystic fibrosis, cAMP fails to
activate the chloride channels.
The gene product is the transmembrane regulator of the passage of ions through the chloride
channel, and expression of the good gene (but not the bad alleles) cures cystic fibrosis at the cellular
level (Nature 347: 358, 1990).
In fact, expression of the gene opens chloride channels, even in recombinant, non-epithelial cells
(Nature 352: 628, 1991).
Ironically, the healthy gene is named "CFTR" (cystic fibrosis transmembrane regulator). Its
expression in tissues: Nature 353: 434, 1991. Exactly where it sits in relation to the rest of the
chloride pumping apparatus is still unclear (Proc. Nat. Acad. Sci. 88: 5277, 1991).
* Rare CF-phenotype patients have normal CFTR: NEJM 347: 405, 2002.
Cyclic-AMP-dependent protein kinase and protein kinase C activate airway chloride channels in
healthy people, but not in cystic fibrosis. Calcium/calmodulin dependent protein kinase activates the
channels of cystic fibrosis patients (Nature 349: 793, 1991), and this may lead to therapeutic
applications eventually.
Studying the gene has confirmed clinicians' impression that mild forms of cystic fibrosis caused by
one or two "mild" alleles are common (NEJM 323: 1685, 1990; "why" Nature 362: 160, 1993).
Interestingly, some male heterozygotes and some men with only mild mutations are healthy except
for absent vas deferens (JAMA 267: 1794, 1992). * The CF recombinant mouse: Nature 359: 211, 1992; Lancet 340: 702, 1992.
The clinical syndrome is complex and reflects the underlying pathophysiology.
The sweat glands perform normally, but chloride is not reabsorbed through the sweat ducts. Hence,
these children's sweat is excessively salty. This forms the basis for the old midwives observation that
"a baby that tastes salty when you kiss it will die in the first year", and the modern-day "sweat test".
*Allele with lung disease but a normal sweat test: NEJM 331: 974, 1994.
In the bronchial epithelium, the defective chloride pump fails to excrete water into the bronchial
lumens. The lumens become plugged by super-thick mucus, and lung infections (Staph. aureus,
Pseudomonas cepacia (now Burkholderia cepacia), a special "mucoid" strain of Pseudomonas aeruginosa) occur again and
again, with pneumonias, lung abscesses, bronchiectasis (i.e., chronic, never-healing ulcers of the
airways that increase dead space), etc.
{11075} cystic fibrosis, lung (see the pus / mucus)
In the pancreatic ductal epithelium, chloride secretion also fails (* ignore "Big Robbins" on
bicarbonate), pancreatic ducts become plugged, and the pancreas undergoes atrophy. Malabsorption
and vitamin deficiencies (notably vitamin A and K deficiencies) result.
Some alleles are harder on the pancreas than on the lung; why this should be is not clear (NEJM
323: 1685, 1990; Lancet 336: 1081, 1990). Others seem to spare the pancreas and intestine: Am. J.
Hum. Genet. 51: 245, 1992.
Secondary diabetes occurs in a few percent of these patients (update J. Ped. 142: 97, 2003).
{08854} cystic fibrosis, pancreas
Those salivary glands that produce mucus (i.e., all but the parotid) may show some degree of
plugging and atrophy, and the saliva of cystic fibrosis patients is more salty than healthy people.
The intestinal crypts also secrete a certain amount of chloride (Gastroenterology 101: 1012, 1991).
Babies may have bowel obstruction due to thick mucus ("meconium ileus", etc.; affects around 5-10% of these babies); the lack of
pancreatic enzymes in the gut doesn't help either.
{20078} meconium ileus, gross
Despite references in pathology books to cystic fibrosis as an important cause of cirrhosis, only
around 5% of patients suffer this complication (Arch. Dis. Child. 66: 698, 1991;
update Arch. Dis. Child. 81: 129, 1999) and rarely die of it.
The cause, of course, is plugging of the bile ducts.
Cystic fibrosis is a particularly cruel disease, causing the lingering deaths of teenagers and young
adults.
In the old days, these children all died in infancy. Today, the life expectancy of a cystic fibrosis
patient is around 25 years, but there are many variables. Pancreatic enzymes can be replaced, lung
infections treated, and meconium ileus treated.
Almost all cystic fibrosis patients eventually suffer from recurrent lung infections with cumulative
scarring. The typical patients spends two weeks in the hospital several times per year. Teens with
cystic fibrosis become familiar friends, hold "prom" on the wards, etc., etc.
Males with the disease are usually infertile ("plugged vas" is the old story; while the vas is typically
absent in a man with CF, it's now clear that CFTR plays a role in spermatogenesis; see Nature 353:
434, 1991). Females have diminished fertility; CFTR is expressed in the uterine epithelium.
Today, various screening protocols are worked out, involving immunoreactive trypsinogen in a
blood spot taken on day 4-5 of life, coupled with gene analysis (Br. Med. J. 302: 1237, 1991).
* We can finally say it: "Cultures matter in cystic fibrosis
outcome" (J. Ped. 132: 202, 1998.
A number of novel treatments for cystic fibrosis are in use or on the horizon.
Recombinant human DNAse I unclogs secretions nicely (JAMA 267: 1947, 1992; NEJM
326: 812, 1992; marketed in 1993 as "Pulmozyme").
Lung transplantation is now fairly common (Thorax 46: 213, 1991; J. Thoracic Cardiovasc. Surg.
101: 633, 1991); 5-year survival seems to be around 50%.
In March 1993, a mouse was reported cured of cystic fibrosis by gene therapy (Nature 362: 25,
1993; unborn mouse Lancet 349: 619, 1997). A trial of gene therapy of cystic fibrosis is underway, using retroviruses to
place the
functional gene into the respiratory epithelium. Keep your fingers crossed.
*Simpler: Ibuprofen, which suppresses neutrophil free-radical production, to keep down the havoc in
the lungs (NEJM 332: 848, 1995).
The common-sense remedy of inhaling hypertonic saline seems to be another
big help (NEJM 354: 229, 2006).
* Trying to get the good CFTR gene into the lungs without using a retroviral
vector: Lancet 353: 947, 1999.
Antenatal diagnosis of cystic fibrosis is now available.
In people of northern European ancestry, the allele delta-F508 (which lacks three base pairs) is the
most common variant (and more severe than others; see Lancet 337: 631, 1991). CFTR made by
this gene is not taken to the plasma membrane (Nature 358: 709 & 761, 1992). It can be detected
using the polymerase chain reaction or other techniques. Prenatal detection of delta-508 was
announced in 1990 (NEJM 322: 291, 1990). Since then, more alleles have been identified
and become available.
We can now detect most heterozygotes. Despite lots of early nay-sayers,
mass-screening is now a reality among the Ashkenazi in the US (long-accustomed
to screening for Tay-Sachs and Gaucher's): Arch. Int. Med. 158: 77,
1998. Finding one case costs $11,000 dollars (Lancet 356: 789, 2000).
The lifetime cost "to society" is $800,000
(JAMA 279: 1068, 1998), and
the
respiratory care alone costs around $40,000 per year, with
deoxyribonuclease actually bringing costs down (Ann. Pharm. 34:
304, 2000).
* The case against screening: JAMA 263: 2777, 1990.
This is still a good read.
The author of this
fascinating article points out the massive ignorance of grammar-school math and science among
parents and clinicians. Remember this, whether or not you agree with the author's rejection of
screening for CF.
Only around 20% of parents of young children with cystic fibrosis say they would abort a second
child with the disease (Am. J. Pub. Health. 81: 992, 1991; of course, they haven't seen what it will
do to their kid yet). Pre-implantation testing of test-tube babies for CF: NEJM 327: 905, 1992. The
awful human impact of cystic fibrosis: "Shattered Dreams", Discover, July 1988.
* Although most people with chronic nasal sinus trouble have normal CFTR genes,
mutated CFTR is much over-represented among them, making
their sinus disease a forme fruste of cystic fibrosis (JAMA 284: 1814, 2000). Watch for more on this.
Basic cancer biology successfully predicts that cancers
would be much less common early in life, when there's been
less time to accumulate mutations.
However, it's hard to explain why any cancers would
be more common in children than in adults.
The explanation must be that these cancers arise from cell types
which adults have lost. And again, this fits with what you
can see for yourself. Wilms' tumor arises
from blastema, and neuroblastoma from neuroblasts, both of which you can
easily find and see to be
dividing in a healthy baby. Both cell types
lose their mitotic potential and vanish
soon after birth.
We know this is true of neuroblastomas, which often "mature" into benign
masses of nerve-like tissue. Probably the high curability of Wilms' tumor
and acute leukemia in the young also results from the last few cells
losing their mitotic potential (and/or undergoing apoptosis)
just as if they'd never turned malignant. Remember we now cure around 77%
of cancers in children under age 15 (NEJM 351: 145, 2004).
However, we haven't yet identified the genes to explain this. Stay tuned.
Here are the tumors worth remembering at different ages:
Age 5-9
Age 10-14 {08455} sacrococcygeal teratoma
Pediatric Pathology
Cornell
Class notes with clickable photos
 Prenatal Diagnosis
Prenatal Diagnosis
WebPath Tutorial
* Note the misuse of the term "embryonic stem cells" in the current
culture-war business. The cells in question are from eight-celled fertilized eggs.
* "Partial birth abortion" goes to the Supreme Court: NEJM 344:
152, 2001. The court reaffirms 5-4 the principle of Roe v. Wade
that this isn't the government's business.
Congress bans the loathsome practice: Lancet 362: 1464, 2003.
The procedure itself seems to
be based on the curious fact that the law protects the life of a child
when, and only when, it is fully delivered. The real purpose is to
prevent the birth of profoundly defective children.
The obvious alternative is
humane, inexpensive
care for these children while nature takes its course ("perinatal
hospice"; Issues in Law
and Medicine 13: 125, 1997).
It is only now coming into use in the United States
(J. Repro. Med. 7: 269, 2004).
* Despite pressure to "do something",
it is not at all clear that
intensive "interventions to improve cognitive and
academic abilities" for these kids do any good at all.
See JAMA 277: 126, 1997.
 Renal tubular dysgenesis
Renal tubular dysgenesis
Potter baby
Pittsburgh Pathology Cases
 Anencephaly
Anencephaly
WebPath Photo
Any cause of neonatal congestive heart failure (i.e., congenital heart
disease, other birth defects compromising blood flow) or severe anemia
(i.e., high-output CHF -- famous causes include both hemolytic disease of the
unborn, the worst thalassemias, and parvovirus B19) can produce severe edema.
 Hydrops fetalis
Hydrops fetalis
Intrauterine death from Rh disease
KU Collection
Subgaleal hematoma
WebPath Photo
* Future pathologists: Here's the progression
of "maceration" after intrauterine death.
Up to eight hours: Red skin only
 Contemporary wars are fought largely by child-soldiers, who in many cases
are kidnapped, brutalized, and given guns.
The children are already bitter over their lives of hunger and menial labor,
and are more willing than adults
to adopt some stupid ideology or blame
their neighbors who look and talk a little different.
They are also more willing to take orders
than adults, and more willing to throw
their lives away.
Contemporary wars are fought largely by child-soldiers, who in many cases
are kidnapped, brutalized, and given guns.
The children are already bitter over their lives of hunger and menial labor,
and are more willing than adults
to adopt some stupid ideology or blame
their neighbors who look and talk a little different.
They are also more willing to take orders
than adults, and more willing to throw
their lives away.
As noted above, the causes of premature labor remain elusive, as is the mystery of
why it's so much more common in the underclass (NEJM 399: 130, 1998).
{09883} sirena
{09888} amnionic band syndrome
{09889} amnionic band syndrome
{18245} omphalocele, failure of abdominal wall to form around umbilical cord
 Prune Belly Syndrome
Prune Belly Syndrome
From a Saddam-era Iraqi
propaganda website (!)
 Prune Belly Syndrome
Prune Belly Syndrome
From a Saddam-era Iraqi
propaganda website (!)
 Ichthyosis "Collodion baby"
Ichthyosis "Collodion baby"
From a Saddam-era Iraqi
propaganda website (!)
 Hydrocephalus, untreated
Hydrocephalus, untreated
From a Saddam-era Iraqi
propaganda website (!)
 Severe midline facial defect
Severe midline facial defect
From a Saddam-era Iraqi
propaganda website (!)
 Sporadic phocomelia (?)
Sporadic phocomelia (?)
From a Saddam-era Iraqi
propaganda website (!)
Newborn's pneumonia
Premature rupture of membranes
WebPath Photo
* Other
functions are being discovered (i.e., it plays a role in exocytosis: Science 256: 444 & 530, 1992).
* Could Chopin's illness have been a milder allele of cystic fibrosis (Med. J. Aust. 147: 586, 1987)? In his era,
those with the full-blown illness did not reach adulthood.
The mouse did not get lung disease, but a newer mouse does: Nat. Med. 10: 453 & 487, 2004.
* Pseudomonas is handled by normal people's lungs using
CFTR, which apparently causes it to enter the epithelial cells
and get destroyed, something of a surprise, and unusual for a
bacterium (Proc. Nat. Acad. Sci. 94: 12088, 1997).
{10139} cystic fibrosis
{20076} cystic fibrosis, lung
{20077} cystic fibrosis, lung (see the mucus plugs)
{26249} cystic fibrosis, lung
{41466} cystic fibrosis, x-ray
{08855} cystic fibrosis, pancreas
 Cystic fibrosis
Cystic fibrosis
Photo and mini-review
Brown U.
{20079} meconium ileus, cross-section
{20080} meconium ileus, microscopic
Meconium ileus
Virtual Hospital
CHILDHOOD TUMORS
Children get different cancers from adults.
Age 0-4
When young lips have drunk deep of the bitter waters of hate, suspicion and despair, all the love in the world will not wholly take away that knowledge.
-- Rudyard Kipling, "Baa Baa Black Sheep" 1888
Joany Phony [Joan Baez]: Oh, look at all those poor orphans! I'm going to stop right here and donate ten thousand dollars!
Li'l Abner: In money?
Joany Phony: No, in protest songs!
-- Al Capp, "Li'l Abner", 1967
 * Politicians will interfere with your ability to be a good doctor for children.
* Politicians will interfere with your ability to be a good doctor for children.
Children do not vote.
When politicians and ideology get involved, children are almost always big-time losers. I would
like to cite five examples. You can add others.
1. "The War on Poverty!" In the early 1960's and the decades before, only 10% of children in the
U.S. were born out of wedlock. These children were typically put up for adoption, and since 10% of
couples are infertile, this worked out nicely. Thanks largely to "compassionate social policies" that
make it far more lucrative and immediately-gratifying for girls to have babies than to go to school,
get jobs, or get married, one third of U.S. children were born out of wedlock from the mid-60's
through the early 90's.
Dad had a strong disincentive to stay around, since Mom got
more money if he disappeared. At the crack houses, "mothers' day" meant
the day the welfare checks
came. By the mid-1990's, even the Far Left
had to agree that the status quo wasn't the best we could be doing for our
children, and the rest is now history.
I note with pleasure (mid-1999) that with the loss of government incentives to have
children out of wedlock, the illegitimacy rate has
dropped spectacularly, and the US teen pregnancy rate is suddenly
lower than it's been in a century.
It's hard not to see this as cause-and-effect. The numbers (though not the "why"'s):
National Vital Statistics Reports 48: 1, 2000.
2. Pious-rightwing "get tough on crime" politics: As a volunteer in criminal justice
in Tennessee in the mid-1980's, I learned that there was (of course) no money for child protective
services, but that there was plenty of money to protect society from "dangerous kids". The system
would take a kid in an abusive or neglectful home situation, find him guilty of something, and put
him in reform school. This also seems to be the rule nationwide, particularly for black youngsters
(Am. J. Orthopsych. 61: 578, 1991). I cannot think that the long-term results of this policy are
salutary.
3. Intellectual-leftwing "multiculturalism and diversity" politics: In 1972, the social workers framed a
major policy document stating that allowing white families to adopt a black child was "a form of
genocide". The result was many white families eager but unable to adopt a black child, and around
50,000 black children at a time chronically institutionalized, almost all of whom could easily have
been placed if legal barriers to timely transracial adoption had not existed. When the debate was re-opened in the early
1990's, the black community was divided. Rev. Jesse Jackson and others argued
that it was more important for every child to have a stable, loving home. Other leaders and
organizations (including, regrettably, Ben Chevis's N.A.A.C.P) argued that it was more important
that every child grow up sharing not only minority group identity, but especially minority group
resentments and hostilities. I am not making this up. See, for starters, K.C. star op-ed 1/2/94. For a
scathing critique of the "mental health" pseudo-expertise at the heart of this fiasco, see Bull. Am.
Acad. Psych. Law. 19: 339, 1991.
See also Child Welfare 70: 477, 1991,
Am. J. Orthopsychiatry 67: 568, 1997 (the kids do great),
and the references in Am.
J. O., above. The Multi-Ethnic Placement Act (1996 thanks Bill)
prevent federally-funded organizations from interfering with transracial
adoptions and foster-care, but it is still widely ignored, with social
workers writing no-data articles about how bad it is.
4. In modern warfare, it is commonplace for governments to deliberately
put their own children where they are most likely to be killed.
This is of course done to obtain media coverage and sympathy, in the hopes
that "compassionate peace-loving peoples around the world" will let the
tyrants get their own way. Every informed person is aware of this,
and I have always been surprised that neither
"liberals" nor "conservatives" raise much fuss over it.
The Viet Cong practice of placing anti-aircraft guns atop schools and hospitals
was succeeded by Saddam Hussein's use of "human shields"
during the first bombing of Baghdad. More recent examples come
from the Middle East and Sri Lanka.
5. Here's a tale from Brown, your lecturer's alma mater, where the students were and are overdosed
on "cultural relativism":
In the past year, [child abuse survivor and ethics professor Richard Cheit] has often wondered
whether he can go on teaching ethics. "They're such moral relativists", he says of his students. "In
the midst of this whole thing, one of my seniors asked, 'Aren't these moral taboos just cultural
constructions? Isn't incest bad just because we think it is?'" (U.S. News Nov 29, 1993, p. 63).
* Being a sick kid in the U.S. is always difficult. The worst part, for many of them, is the isolation
from peers.
Being a healthy school kid in the U.S. isn't always easy, either. Before you decide that a kid with
school phobia is "a victim of secret sexual abuse" or has "attention deficit disorder" or whatever's the
current fad in psychiatry, remember that today's schools are full of gangs, guns
(in some communities, kids reportedly
have to carry them just to travel safely to and
from school; guns in the schools Arch. Ped. Adol. Med.
151: 360 & 555, 1997, Arch. Ped. Adol. Med. 153:
21, 1999, just before Columbine),
bullies (suddenly
discovered as a problem: Br. Med. J. 310: 274, 1995;
Child Abuse & Negl. 22: 705, 1998; J. Child Psych.
39: 533, 1998; JAMA 285: 2094, 2001; Br. Med. J. 323:
480, 2001; kids who are crippled
or otherwise different
are singled out for torment), and
a percentage of moronic-cruel teachers.
Violent deaths at school: JAMA 275: 1729, 1996.
The recent celebrated school shootings were by boys who had been bullied
(Sci. Am. Sept. 1998; weakling Michael Carneal, who opened fire on a
"prayer fellowship" in Kentucky, had been ridiculed,
bullied and threatened by members of the group; one "Christian" responded
to the boy's cry for help a few days earlier by threatening
to beat him up: US News Dec. 15, 1997.)
If you have ever gone hungry because your lunch
money was stolen, or had your homework or art project maliciously
destroyed, or been unable to use the bathroom because you would get
roughed up, you can perhaps understand.
The Left ("Let's spend a lot of somebody
else's money for a course in conflict resolution!" "Differences
must be tolerated and encouraged!" "Schools should be a place
where values are clarified!"), despite their
general interest in finding "victims",
have always
ignored the bullies. (There is zero evidence that "teaching
conflict resolution", the current fad, does any good: Sci. Am. Sept. 1998).
The Right ("D.A.R.E."; "I don't think they should teach ANY
science until college"; "Schools should be a place where
family
values are taught") have always ignored the bullies.
Doc: Pre-teen won't tell why he's afraid? Ask about shyness in the group shower. Public
schools have long been dominated by politics and ideology, so that today,
especially in poor communities, teachers have no incentive to teach well, and students have no (or
negative) incentive to learn well. In the inner cities especially, longstanding attitudes about
education have reduced the schools to mere day-care centers. Of course, this feeds into the cycle of
non-achievement and hopelessness that shouldn't be part of any kid's life, but is. Sooner or later,
somebody needs to claim "victim" status on a talk show or a sentencing hearing "because I was
never forced to do homework as a kid, and now I'm stupid." In the area of science education alone,
the impacts of both far-Right and far-Left
have made the United States the laughing-stock
of the world scientific and educational community. Today, there's even a bureaucratic procedure
whenever a student bored into fidgeting because of hours of passive and rote learning gets
"recommended for Ritalin therapy" by a teacher. (Ritalin, i.e., methylphenidate, is now known to work in the same way
on anybody, whether or not they "have A.D.D."; it enables anybody to stay focused on a boring task,
and present estimates are than 10% of U.S. grade-school boys are on the stuff: Br. Med. J. 312: 657,
1996.) I was in grammar school in the 1950s, and I remember left-handed kids being punished for
writing with their left hands. That's how stupid and cruel it gets.
Since then, I've watched most-if-not-all of our young people's problems
blamed (more or less successively) on the international communist conspiracy, teaching evolution,
non-conformity, food additives, "elitism", dyslexia and "minimal brain dysfunction", refined sugar,
"secular humanism", attention-deficit disorder, all-pervasive-yet-imperceptible vicious racism, cow's
milk, multicultural insensitivity, grading students instead of "focusing on building their self-esteem",
not teaching radical Afrocentrism, multiple chemical sensitivities,
and secret-forgotten sexual abuse.
Simplistic (when not totally wrong),
and proposed/attempted solutions (which are always part of somebody's political-economic agenda)
are just as dumb.
The 1990's mandate to remove asbestos from school buildings
is now universally recognized as having been a colossal waste of money.
And I think most educators
today will tell you that today's entitlements for children
with special needs have grown far in excess of what is reasonable,
and interfere seriously with teaching reading, writing, and arithmetic
to the healthy children.
From
the mid-1980's to just-recently, there was a
monumentally stupid fad to ban (not just de-emphasize) the study of phonics and teach reading by
word-recognition only (i.e., kids aren't allowed to sound-out words, but must guess what they are
from context; this is an dumbing-down
abuse of the "Whole Language" model, it clearly explains the sharp rise in
U.S. illiteracy in the past ten years, and it finally was banned in California
in early 1997;
California was the center of the no-phonics fad, and the good
citizens of the state were dismayed when it resulted in their
children's reading scores plummeting to second-to-the-bottom in
the US. I predicted the disaster in 1985.
In 1998, even the National Research Council (Feds) came out with
a statement that kids learn best if they learn phonics too.
During the stupid fad, savvy parents bought phonics packages for
home-teaching.) The fiasco in retrospect: Sci. Am. 286(3): 84, 2002.
"Bilingual education", long a cornerstone of education
in communities with many Hispanic members, is recognized today
as having been another disaster.
After "Saving Private Ryan", two different teens
on two different occasions
asked me, "Why were we never taught in school about D-day or
what the second world war was fought about?" If it got covered
at all, it's not sticking. The
perennial desire is for "the schools to teach values",
which, if they're not taught in the home and
backed up by tough-love discipline, get nothing but lip service (and after-hours ridicule) from savvy
children. As a country in which only 17% of us grown-ups say grace with our families at meals,
only 33% show up at weekly services, but 80% of us want our children to be taught to pray the
classroom, I'd say that we grown-ups are getting what we deserve when 12-year-old kids rob us at
gunpoint. You may disagree. As a physician, you are educated to recognize bad science and
emotionally-based foolishness. You may wish to take an interest in your local public schools.
Too many textbooks and discussions leave students free to make up their minds about things.
-- Mel Gabler, Texas "conservative" textbook critic
* "Family values!" is a positive-inferential term
that means many things to many people.
As politicians (liberal, conservative)
make political capital by decrying Joe Camel and
dirty pictures on the internet ("Protect our children! Protect our children!"), around two million kids
silently leave home for the streets, or otherwise become homeless, each year (see, for example, Pub.
Health. Rep. 108: 150, 1993). On any night, there are at least 100,000 kids living on the streets,
separated from their families. Some are "runaways". Many are "throwaways". Most are
something-in-between. Almost all are escaping intolerable family living situations (Hosp. Comm.
Psych. 43: 155, 1992). Most support themselves on the "street economy" (MMWR 42: 873, Nov.
19, 1993) by panhandling, petty crime, the drug trade, and/or prostitution. (I use the "politically-incorrect" term
without apology to the Left. The term "commercial sex work" implies a certain
dignity and work-satisfaction that child prostitution doesn't possess.
Child prostitution around the world: Lancet 359: 1417, 2002.
A large minority of
runaways, male and female, turn to prostitution; of course the "academic" literature refers to these
kids as "sexually delinquent".) The Right talks about "protecting the family and the authority of
parents" and offer no humane solutions whatsoever. (I note with hope the new emphasis of the
conservative "Promise Keepers" on not being physically or verbally abusive with your family, while
at the same time demanding decent behavior. Newt's orphanages sounded like the best idea so far to
me -- ask me why, if you want.) The Left
will usually suggest trendy-lucrative "drug, alcohol, and AIDS
counseling" and some also offer their brand of political indoctrination. Actual effective help for
these kids (who are mostly mistrustful, recalcitrant, and lacking in useful skills) comes from
apolitical private individuals and agencies and mainstream religious organizations. There's plenty
written about these kids; if you're going to do primary care and/or care about children, spend a few
hours at a big medical school library and read up on the problem like I did. Runaways-throwaways
tend to come from violent, abusive families in which kids are offered little opportunity for autonomy
or individuation (gee whiz, Adolescence 28: 867, 1993). Adolescents are every bit as likely to be beaten
by their parents as are younger kids; not surprisingly, these kids are mostly not paragons of virtue
and social responsibility, and interestingly, people at protective services are likely to say that getting
beaten is the teen's own fault (JAMA 270: 1850, 1993). Abusers typically say, "We / my partner /
you spoiled the child." Examined in the cold light of reason, the decision by many girls to run away
seems to be itself the result of clear thought and reflection: Adolescence 27: 387, 1992 (i.e., neither
the far-Left nor the far-Right, despite all their talking, are willing to actually do anything to
protect her from incest or whatever). Suspect incest when a parent (usually the father)
is "overprotective" of a child, severely restricting outside activities;
often these abusers are big on "family values" and right-wing anti-everything
"spirituality".
Not surprisingly, street teens are typically unable to read
("thank you, Today's Educational Establishment"), and those who can aren't much inclined to
read things, in particular pamphlets on AIDS prevention (Pub. Health Rep., above, gee whiz
Uncle Sam.) Government AIDS education projects for street kids seem like a total flop to
this reviewer: MMWR 42: 873, 1993 for the statistics; Pub. Heath Rep. above agrees (gee whiz).
An elaborate program based on "educational theory" intended to prevent
kids from taking sexual risk was a total flop: Br. Med. J. 324: 1430, 2002;
so was a massive intervention to educate girls not to get pregnant: Br. Med. J. 324: 1426, 2002
The
current ideology in the child-protection business is "Don't break up the biological family; give
everybody lots of counseling instead". ("Elisa Izquierdo syndrome"). That means more money for
trendoid-counselors and of course less money spent overall; does it work well? Of course not.
Adults who beat up children are
not reasonable people
interested in benefiting from psychotherapy.
Children know it's a sham and become bitter.
Some workers in the trenches, where it really matters, testify that the current system simply isn't
reaching kids in need or doing what it's supposed to do: J. Adol. Health 12: 555 & 576, 1991.
There is, of course, no real access to health care for runaway kids, for example, if they're HIV-positive (J. Adol. Health.
12: 504, 1991). One statistic I could not find is how many "sexually
delinquent" street boys were thrown out of their homes for "being gay" in the first place
(pseudo-conservatism strikes again! -- this is NOT what "family
values" means to most of us), but this fiasco is extremely common (J. Adol. Health
12: 515, 1991; homosexual orientation is almost never a deliberate choice,
a fact which is ignored by right-wing adults trying to make political
capital at these kids' expense.
A teenaged boy who believes he is gay often has a
choice, particularly in a "conservative moral home", of being ridiculed
and beaten regularly
by his parents (J. Consult. Clin. Psych. 62: 261, 1994) and suiciding or running away: JAMA 275:
1354, 1996.) It is extremely difficult to provide effective social services for these kids, since they
are pawns in the culture war (left vs. right: Child Welfare 73: 291, 1994). Fewer than
half of adolescent male prostitutes have had normal sex with a woman (J. Adol. 14: 229, 1991).
The pop wisdom that being molested sexually typically has major
long-term pervasive adverse consequences is now being challenged
(Psych. Bull. 124: 22, 1998) -- when the impact of a crazy
home is controlled for, the effect of sexual abuse largely
disappears. (This is the famous article that the US Congress unanimously
"condemned"; common-sense told me the authors went too far in their rhetoric,
even if their data is okay.)
This is not to say that sexual contact between adults and children
isn't wrong or that it should be treated lightly.
It is also part of our world. According to the British,
three-and-a-half million "sex tourists" go to the poor nations
each year with the specific intent of having sex with children
(Lancet 363: 542, 2004 -- Spain cracks down....)
We'll briefly review childhood sexual abuse under "CNS", when we talk about the "repressed
memories" fiasco of 1988-1995. Reading on victims and perpetrators
of the real thing: Br. J. Psych. 169: 408, 1996.
Sexual behavior in children includes a
considerable amount of exploring, and not everybody agrees about how much
of this is wholesome (Child Abuse & Neglect 22: 289, 1998).
The current definition of "sexual abuse" seems to include simply
getting flashed once, or shown dirty pictures once, or even showing it to an older kid who asked (Br.
Med. J. 312: 1326, 1996); under these definitions, 10% of boys are sexually abused and 33% of
girls are sexually abused, and these numbers seem to hold up internationally. (The horrendous adult
misbehavior that most of us think of when we hear the words "sexual abuse" is far, far less
common, thankfully.) Kids running away from insufferable homes are, of course, nothing new. If
you haven't read "Huckleberry Finn" or the novels of Charles Dickens, do so sometime.
In the poor nations, children are simply left even in the most
atrocious situations (J. Urol. 160: 1116, 1999, young boys are
returned to families that just cut their penises off); otherwise they
would starve. In 2003 (Lancet 361: 1196, 2003)
Brazil suddenly discovered that its huge number of homeless kids include
child prostitutes and promised they will all stop being prostitutes by 2004.
* Loathsome teenage ideas (racism of all varieties, silly-disgusting occultism, right-wing and left-wing demagoguery, proud
do-nothing bitterness and bad-mouthed entitlement, live-fast-die-young,
amoral pseudo-mysticism, and glorification of weird sex, death, and violence; have you visited your
local music store lately?) are supposed to provide a focus for peer groups that are "a substitute for
caring parents and other figures that these youngsters can look up to..." and so forth. They also deal
directly and explicitly (though I'd say badly and foolishly) with issues that parents have learned
not to speak about. I believe this is substantially correct [abstract 92376240; from Germany, where
they talk more bluntly, I guess]. Kentucky teen vampire cult:
Child Psych. Hum. Dev. 29: 209, 1999. Kids who commit
genuine hate crimes don't belong to grown-up hate groups (Am. J. Psych. 160: 979, 2003).
* The neuropathology of attention deficit disorder, in which the kid can't concentrate or focus, is
being worked out; the current work focuses on the caudate and its frontal lobe connections, which
have to do with the ability to pay attention (Am. J. Psych. 151: 1791, 1994). It appears to be
autosomal dominant with variable penetrance. One locus might be the dopamine transport gene
DAT1 (Am. J. Hum. Genet. 56: 993, 1995); dopamine transport is inhibited by methylphenidate
and amphetamine, which help attention deficit disorder. This writer believes this is a real entity (you
can tell, because the kid can't focus on play: Br. Med. J. 311: 72, 1995), amenable to therapy with
sympathomimetics (or try the few-foods approach: Arch. Dis. Child. 69: 564, 1993; JAMA 293:
1871, 1995). The writer also wonders what ever happened to kids who are disruptive simply
because they are undisciplined, or unproductive because they lack guidance (no $ in diagnosing this,
I guess, and somebody might get offended and boohoo to the judge). Tartrazine yellow, long
considered an exacerbating factor by mothers and the tabloid press, might really make these kids
worse: J. Ped. 125: 691, 1995. Before you diagnose "attention deficit disorder",
I trust you'll rule out hearing problems, vision problems, lead poisoning,
a chaotic home, and lack of discipline. Good luck.
Likewise, by the mid-1990's, learning disability were diagnosed in 3 million
U.S. kids, typically on the basis of academic performance staying below measured IQ. The kids
then get special treatment. This writer believes learning disabilities are real, but wonders what
happened to kids who are lazy, unmotivated, or unsupervised by their parents. Such kids, if they
exist (ha ha) would meet the above criteria for "learning disabled", but there is no $ in diagnosing
this, I guess, and somebody might get offended and boohoo to the judge. Even Science 267: 1896,
1995 is with your writer on this; in the years that followed, the literature started
getting more sensible, and limiting the term "learning disability" to what we
used to call "mental retardation" (Lancet 362: 811, 2003), affecting 1.5-2%
of the population. We'll cover pervasive developmental defect ("autism", "Rain
Man") under "CNS"; it's entirely a wiring problem and anyone who tells you otherwise is ignorant.
* As a family physician, you should see a teen who wishes to be seen without the parents'
knowledge. Don't expect to get paid, Doc. Further, you're damned-if-you-do, damned-if-you-don't
because of confidentiality issues (Curr. Op. Ped. 5: 395, 1993). Of course, if there's an anti-abortion
tell-the-parents snitch-law in your state, and this applies to the teen's problem, you need to let the
teen know. Your lecturer, who objects to abortion under most circumstances (and who recognizes
and respects the fact that many people disagree with him), would take the anti-abortion militants
more seriously if they also wanted to make contraception more available to teens -- some girls,
especially in very bad neighborhoods, truly have no choice. Approach to the
kid who is supposedly sexually abused: South. Med. J. 87: 1242, 1994.
* Final note, citing what is (after "I have a right to...") probably our era's most popular slogan: I am
glad that many people champion what they perceive to be good causes, though none of us agree with
all of these. However... When someone championing a cause or philosophy tells you that "A society
is to be judged by how it cares for its most helpless members" (meaning, depending on the speaker,
irreversible coma patients, people who caught the very bad sexually transmitted disease, unwanted
fetuses, fetuses with Duchenne's muscular dystrophy, people with end-stage multiple sclerosis
seeking Dr. Kevorkian's services, babies born without a forebrain, the non-compliant mentally ill on
the streets, alcoholic bullies, heroin addicts, spotted owls, albino lab rats, beef cattle, unwanted
puppies, frozen blastulas,
cold-blooded lying murderers on death row, etc., etc., etc.), find out whether the speaker has ever
done anything for the healthy, neglected and mistreated kids in his or her own town.
 * Regrettably, concern with child abuse (sexual and otherwise) has become the preoccupation of the
lunatic fringes (right, left), tending to discredit others who want to do something about this very
serious problem. When we come to CNS, we'll discuss the "hypnotically-enhanced memories"
fiasco of the 1988-1995 era, in which amateur and pseudo-professional psychotherapists convinced
troubled people that their fathers or some other man had molested them bizarrely over many years,
and hundreds of families were broken up, lives were ruined, men were sent to prison, and so forth.
However, if an activist wants to "find" horrid, weird, secret abuse in a day care center,
hypnosis isn't even required. Kids are extremely suggestible, and even "experts" are notoriously
unable to agree as to whether a child's story of common-style sexual mistreatment is credible, and
what's the future risk (i.e., it ain't a science, folks; Bull. Am. Acad. Psych. Law. 218: 281, 1993). In
the contemporary witch-hunt, once one student makes one accusation, some community nut (on the
lunatic fringe of the "Christian right", "New Age", "child protective advocacy", "feminist", and/or
"recovery" movements) takes up the cause, the rest of the kids are told they are "in denial", and they
get grilled repeatedly for months by "therapists" and prosecutors until they "remember". As any
doctor knows, the best way to get the truth during an interview is to ask open-ended questions;
activist "therapists" typically do just the opposite. Eventually, preposterous, constantly-changing
stories emerge ("He slaughtered a giraffe in the kindergarten room" is typical), innocent people are
put on trial, lives are ruined, and so forth (New Yorker 10/3/94). There have been over one hundred
such trials, almost all of them extremely long and expensive. The prosecutors (who aren't always
stupid) may realize it's all rubbish, but must continue the prosecutions for political reasons. The
"therapists" always say "Believe the children! Believe the children! You are victimizing them again
if you don't believe them!", never explaining why they don't believe the children originally when
they say nothing happened. At least one acquitted defendant was murdered afterwards by a
vigilante. The same kind of thing happened at the Salem Witch trials of 1692, where 20 people
were put to death (19 hanged, one tortured to death) on the testimony of a group of children, ages 5-12. Case law, which is
very sane, deals only with procedural stuff, and leaves the decision about the
child's testamentary capacity to the judge (Supreme Court White vs. Illinois 1992, Coy vs. Iowa
1988). Children have enough problems with gangs, drugs, crime, and honest-to-goodness abuse
(i.e., almost always in the home). We ought to stop coercing them into making up stories of abuse.
* Regrettably, concern with child abuse (sexual and otherwise) has become the preoccupation of the
lunatic fringes (right, left), tending to discredit others who want to do something about this very
serious problem. When we come to CNS, we'll discuss the "hypnotically-enhanced memories"
fiasco of the 1988-1995 era, in which amateur and pseudo-professional psychotherapists convinced
troubled people that their fathers or some other man had molested them bizarrely over many years,
and hundreds of families were broken up, lives were ruined, men were sent to prison, and so forth.
However, if an activist wants to "find" horrid, weird, secret abuse in a day care center,
hypnosis isn't even required. Kids are extremely suggestible, and even "experts" are notoriously
unable to agree as to whether a child's story of common-style sexual mistreatment is credible, and
what's the future risk (i.e., it ain't a science, folks; Bull. Am. Acad. Psych. Law. 218: 281, 1993). In
the contemporary witch-hunt, once one student makes one accusation, some community nut (on the
lunatic fringe of the "Christian right", "New Age", "child protective advocacy", "feminist", and/or
"recovery" movements) takes up the cause, the rest of the kids are told they are "in denial", and they
get grilled repeatedly for months by "therapists" and prosecutors until they "remember". As any
doctor knows, the best way to get the truth during an interview is to ask open-ended questions;
activist "therapists" typically do just the opposite. Eventually, preposterous, constantly-changing
stories emerge ("He slaughtered a giraffe in the kindergarten room" is typical), innocent people are
put on trial, lives are ruined, and so forth (New Yorker 10/3/94). There have been over one hundred
such trials, almost all of them extremely long and expensive. The prosecutors (who aren't always
stupid) may realize it's all rubbish, but must continue the prosecutions for political reasons. The
"therapists" always say "Believe the children! Believe the children! You are victimizing them again
if you don't believe them!", never explaining why they don't believe the children originally when
they say nothing happened. At least one acquitted defendant was murdered afterwards by a
vigilante. The same kind of thing happened at the Salem Witch trials of 1692, where 20 people
were put to death (19 hanged, one tortured to death) on the testimony of a group of children, ages 5-12. Case law, which is
very sane, deals only with procedural stuff, and leaves the decision about the
child's testamentary capacity to the judge (Supreme Court White vs. Illinois 1992, Coy vs. Iowa
1988). Children have enough problems with gangs, drugs, crime, and honest-to-goodness abuse
(i.e., almost always in the home). We ought to stop coercing them into making up stories of abuse.
* Nowadays,
"Huckleberry Finn syndrome" refers to a person of substantial natural abilities but little direction or
ambition, supposedly as a result of neglectful or abusive parents.
The theme of the novel is that a child from a trash background
is nevertheless wiser and morally superior to the "sivilized"
folks who even he feels are his betters.
* Shakespeare's "Romeo and Juliet" may have been spoiled for you as required reading in high
school, and/or by parodies of the balcony scene and/or a bad (left-wing, right-wing) college
"Western Civ" course. Think: The play's about godawful teenaged murder-suicide. (Juliet is 14,
Romeo 16.) Shakespeare's plot-source was a warning to teenagers to obey their parents. The
themes of the play, which were pretty-much new with Shakespeare and very radical in his time, are
(1) young people ought to be allowed to marry for love, not just whoever their parents choose for
them; (2) young people's tragedies likely result from their parents' stupidity and meanness; (3) love
matures people, and gives dignity, meaning, and beauty even in the worst of circumstances. By
the way, did you notice that Papa Capulet is an old guy ("past [his] dancing days",
thirty years since he was "in a mask"), but Mama Capulet
is was pregnant with Juliet at age 13 . In other words, she was the old
lecher's forced child-bride and she is setting up the same thing for Juliet.


|
You can lead a kid to knowledge but you can't make him think.
|
 |

 Syndactyly
Syndactyly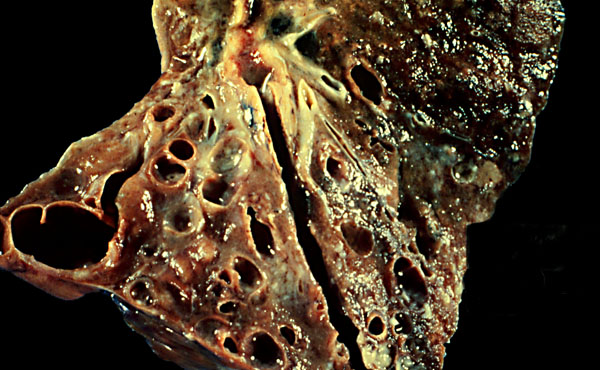 Cystic fibrosis
Cystic fibrosis