Ed Friedlander, M.D., Pathologist
scalpel_blade@yahoo.com



Cyberfriends: The help you're looking for is probably here.
Welcome to Ed's Pathology Notes, placed here originally for the convenience of medical students at my school. You need to check the accuracy of any information, from any source, against other credible sources. I cannot diagnose or treat over the web, I cannot comment on the health care you have already received, and these notes cannot substitute for your own doctor's care. I am good at helping people find resources and answers. If you need me, send me an E-mail at scalpel_blade@yahoo.com Your confidentiality is completely respected.
 DoctorGeorge.com is a larger, full-time service.
There is also a fee site at myphysicians.com,
and another at www.afraidtoask.com.
DoctorGeorge.com is a larger, full-time service.
There is also a fee site at myphysicians.com,
and another at www.afraidtoask.com.
Translate this page automatically
 |
With one of four large boxes of "Pathguy" replies. |
 I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
Numbers in {curly braces} are from the magnificent Slice of Life videodisk. No medical student should be without access to this wonderful resource. Someday you may be able to access these pictures directly from this page.
Also:
Medmark Pathology -- massive listing of pathology sites
Freely have you received, freely give. -- Matthew 10:8. My
site receives an enormous amount of traffic, and I'm
handling about 200 requests for information weekly, all
as a public service.
Pathology's modern founder,
Rudolf
Virchow M.D., left a legacy
of realism and social conscience for the discipline. I am
a mainstream Christian, a man of science, and a proponent of
common sense and common kindness. I am an outspoken enemy
of all the make-believe and bunk that interfere with
peoples' health, reasonable freedom, and happiness. I
talk and write straight, and without apology.
Throughout these notes, I am speaking only
for myself, and not for any employer, organization,
or associate.
Special thanks to my friend and colleague,
Charles Wheeler M.D.,
pathologist and former Kansas City mayor. Thanks also
to the real Patch
Adams M.D., who wrote me encouragement when we were both
beginning our unusual medical careers.
If you're a private individual who's
enjoyed this site, and want to say, "Thank you, Ed!", then
what I'd like best is a contribution to the Episcopalian home for
abandoned, neglected, and abused kids in Nevada:
My home page
Especially if you're looking for
information on a disease with a name
that you know, here are a couple of
great places for you to go right now
and use Medline, which will
allow you to find every relevant
current scientific publication.
You owe it to yourself to learn to
use this invaluable internet resource.
Not only will you find some information
immediately, but you'll have references
to journal articles that you can obtain
by interlibrary loan, plus the names of
the world's foremost experts and their
institutions.
Alternative (complementary) medicine has made real progress since my
generally-unfavorable 1983 review linked below. If you are
interested in complementary medicine, then I would urge you
to visit my new
Alternative Medicine page.
If you are looking for something on complementary
medicine, please go first to
the American
Association of Naturopathic Physicians.
And for your enjoyment... here are some of my old pathology
exams
for medical school undergraduates.
I cannot examine every claim that my correspondents
share with me. Sometimes the independent thinkers
prove to be correct, and paradigms shift as a result.
You also know that extraordinary claims require
extraordinary evidence. When a discovery proves to
square with the observable world, scientists make
reputations by confirming it, and corporations
are soon making profits from it. When a
decades-old claim by a "persecuted genius"
finds no acceptance from mainstream science,
it probably failed some basic experimental tests designed
to eliminate self-deception. If you ask me about
something like this, I will simply invite you to
do some tests yourself, perhaps as a high-school
science project. Who knows? Perhaps
it'll be you who makes the next great discovery!
Our world is full of people who have found peace, fulfillment, and friendship
by suspending their own reasoning and
simply accepting a single authority that seems wise and good.
I've learned that they leave the movements when, and only when, they
discover they have been maliciously deceived.
In the meantime, nothing that I can say or do will
convince such people that I am a decent human being. I no longer
answer my crank mail.
This site is my hobby, and I presently have no sponsor.
This page was last updated February 6, 2006.
During the ten years my site has been online, it's proved to be
one of the most popular of all internet sites for undergraduate
physician and allied-health education. It is so well-known
that I'm not worried about borrowers.
I never refuse requests from colleagues for permission to
adapt or duplicate it for their own courses... and many do.
So, fellow-teachers,
help yourselves. Don't sell it for a profit, don't use it for a bad purpose,
and at some time in your course, mention me as author and KCUMB as my institution. Drop me a note about
your successes. And special
thanks to everyone who's helped and encouraged me, and especially the
people at KCUMB
for making it possible, and my teaching assistants over the years.
Whatever you're looking for on the web, I hope you find it,
here or elsewhere. Health and friendship!
If nature had wanted you to be a specialist, she'd have had you born with one eye with a microscope
fastened to it.
-- Buckminster Fuller
"An eye for an eye" makes the world blind.
-- Mohandas Gandhi
τυφλάς ΄εν αύτοίς ΄ελπίδας καταώικισα -- Aeschylus's Prometheus
Heaven wheels above you displaying to you her eternal glories
and still your eyes are on the ground. -- Dante
{21860} normal fundus
QUIZBANK Eye & Ear #'s 1-42
On general anatomic pathology services, pathologists seldom see material from the eye. We've
already mentioned eye disease when we talked about trachoma, diabetes, vitamin A deficiency,
onchocerciasis, and loa loa. "Big Robbins" contains a chapter on "Eye" that you will probably
want to read. Learning objectives for this unit...
Give a reasonable differential diagnosis for conjunctivitis, uveitis, and
cataracts
Describe the abnormal anatomy and physiology of each of these,
and recognize it anatomically:
Great pictures of retinal diseases: NEJM 331: 95, 1994.
The pathologists at Duke decided to examine eyes routinely at autopsies,
and claim that there was something important in 32%, and at least one diagnosis in 86%.
I am not sure that everyone will agree with their conclusion that eyes should
always be taken, and I doubt families will always want this. But you decide.
See Arch. Path. Lab. Med. 125: 1193, 2001.
There are about 45 million blind people in the world, including 6 million children.
It is far more common in the poor nations than in the industrial nations,
and the most common causes are lack of health care, vitamin A deficiency,
poor sanitation, "traditional health practices", and
uncorrected refractive error. No, I am not making this up. Review
Br. Med. J. 327: 760, 2003.
Eye enucleations are not rare. About half are done for tumors, and a majority
of the rest are taken because of trauma (Am. J. Clin. Path. 119: 594, 2003.)
The following terms are the ones I wish I'd learned in my basic sciences years. Additional terms
appear underlined in the remainder of the handout.
Amaurosis: An eye that appears normal, but is blind. Perhaps the lesion is in the optic nerve or
brain. Amaurosis fugax: An episode of blindness lasting less than ten minutes (mini-thrombi or
vasospastic, treat the latter, as with other types of vasospasm, with calcium channel blockers NEJM
329: 396, 1993).
Amblyopia: An eye that appears normal, yet cannot see normally. One important cause is the "lazy
eye", i.e., the one ignored by strabismus patients.
Angle: The angle in the anterior chamber where the uveal tract joins the cornea-sclera. This is
where the aqueous humor drains from the eye.
Arcus: Fatty deposit around the limbus of the cornea.
"Arcus lipoides". Don't give it much attention; these people's atherogenic
lipids are a bit more likely to be disturbed (Neth. J. Med. 55:
184, 1999). A young person with arcus
can have high LDL's, a corneal dystrophy, or be normal. We prefer not to say
"arcus senilis".
Buphthalmos: Swollen globe, as in childhood glaucoma.
Cataract: Any opacification of the crystalline lens
Coloboma: Malformed iris and ciliary body.
{22238} coloboma
Color blindness: Inherited defects in one or more of the cones. Most are X-linked recessives.
Common red-green blindness is well-known; deuterans have trouble seeing blue and green, protans
have trouble seeing red, etc.
Cotton-wool patch: An ischemic area of the nerve-fiber layer of the retina
Cyclitis: Inflammation of the ciliary body
Dacryocystitis: Inflammation of the lacrimal apparatus
{13179} dacryocystitis
Dot-and-blot hemorrhages: Bleeding into the inner nuclear layer of the retina
Drusen: Accumulation of inert material (described as a mix of protein and lipofuscin) at the
basement membrane of the choroid.
{22830} drusen
Ectropion: Eversion of an eyelid
Endophthalmitis: Inflammation of the interior of the eye
Entropion: In-turning of an eyelid, often as a result of scar contraction on its conjunctival surface.
This sounds bad and is; for one thing, the eyelashes scratch the cornea.
Epicanthus / epicanthic fold: An extra fold of skin next to the nose, imparting a distinctive contour to
the periorbital tissue
Esotropia: Crossed eyes; convergent strabismus
Exophthalmos: When the eyeball is pushed too far forward
Exotropia: Wall-eyes; divergent strabismus
Flame hemorrhages: Bleeding into the nerve-fiber layer of the retina
Fluorescein: Dye used in ophthalmology to better visualize breaks in the surface of the cornea.
Hyperopia / hypermetropia: Farsightedness, convergence of focus posterior to the retina. Often, but
not always, due to a foreshortened eyeball.
Hypertelorism: Eyes set very wide apart.
Hyphemia: Blood in the anterior chamber
Hypopyon: Pus in the anterior chamber
Hypotelorism: Eyes set very close together
Iritis: Inflammation of the iris
Keratic precipitate: Clusters of chronic inflammatory cells on the inner surface of the cornea.
"Mutton-fat"; seen in uveitis.
Keratitis: Inflammation of the cornea
Keratoconus: Cone-shaped cornea
{22180} keratoconus
Leukocoria: White instead of the normal red pupillary light reflection. Think of retinoblastoma!
Limbus: The junction between the cornea and the sclera
Marcus Gunn pupil: Descriptions vary, but this is an indicator
for optic nerve damage in the involved eye. The pupil is larger than
the other one ("to let in more light"), and constricts more slugglishly
than the other on both direct and consensual testing.
Myopia: Nearsightedness, convergence of focus anterior to the retina. Often, but not always, due to
an elongated eyeball.
Panophthalmitis: Inflammation of the whole eye. Usually bacterial, after trauma.
Papilledema: Changes in the optic disk seen in increased intracranial pressure. Mechanisms are
complex and reviewed in "Big Robbins"; longstanding papilledema damages the optic nerve.
{22092} papilledema
Phaco-, phako-: Pertaining to the lens of the eye
Photophobia: Pain on exposure to light
Phthisis bulbi: End-stage, shrunken, often painful eye
Presbyopia: Loss of the ability of the lens to alter its shape; one result of advancing age.
The usual
reason people get bifocal eyeglasses.
Proptosis: Forward protrusion of the eye
Retinal dysplasia: Persistence of many little tubules and/or "rosettes", like in embryonic eye or
classic retinoblastomas. Seen, usually with other abnormalities, in certain birth defects.
Scotoma: A blind spot
Strabismus: Eyes pointed in different directions, the result of eye muscle balance problems. Several
interesting synonyms exist, including (for some reason) "squint".
Synechiae: As elsewhere, fibrous adhesions resulting from healing
Uvea / Uveal tract: Term for the vascular coat of the eye, i.e., the choroid, ciliary body, and iris.
Xerophthalmia: Dry eyes
BIRTH DEFECTS: A selection
Trisomy 13 ("Trisomy D", "Patau's")
You're already familiar with the other stigmata of this illness. The eyes are almost never normal.
They may be single ("cyclops") or fused (cyclops variant); even if there are the correct number, they
present an array of abnormalities described in "Big Robbins".
Future eye pathologists: A coloboma with cartilage suggests Patau's.
Trisomy 21 ("Down's", etc.)
Brushfield's spots are areas where the iris is hypoplastic.
{15608} Brushfield's spots
A variety of other abnormalities are common. Remember esotropia and epicanthic folds.
Congenital rubella syndrome
Again, you are familiar with the other features of this syndrome.
Rubella cataract results from retention of nuclei in the center of the lens. This is pretty distinctive.
*The iris epithelium is largely necrotic, there may be granulomas, and so forth. The result is leather
iris.
*The pigment layer of the retina alternates between hypertrophic ("pepper") and atrophic ("salt")
areas.
* Congenital rubella syndrome with blindness is still rampant
where immunization is not practiced, or where people refuse (Arch. Ophth. 122: 541, 2004;
J. Inf. Dis. 187(S1): S-146 & S-191 & S-223 & S-235, 2003; Am. J. Pub. Health 90: 1555, 2000).
Congenital syphilis
Again, you are familiar with the extra-ocular features.
The characteristic eye finding is inflammation of corneal stroma (interstitial keratitis). This appears
in youth, but is not present at birth.
There are likely to be other abnormalities in the eyes.
Tay-Sach's
In this and a few other inborn errors of metabolism, the normal red of the macula forms the "cherry"
in the pale, lipid-laden retina.
{20115} cherry red spot
LID PROBLEMS
Sty (hordeolum) is suppuration (usually staphylococcal) of the hair follicle, sebaceous glands
(* "Zeis's glands"), and/or apocrine glands (* "Moll's glands").
{13143} chalazion
Of course, infections that involve the bulbar conjunctiva often involve the conjunctiva of the lid, too.
See below.
VITAMIN A DEFICIENCY (still around: Br. Med. J. 310: 1051, 1995)
The basic problem (at the front of the eye) is excessive squamous differentiation of the corneal
epithelium ("xerophthalmia"). Bitot's spots are actually just the
thickened, hyperkeratotic epithelium, typically at the limbus.
As you'd also expect, the cornea mucus cells are lost.
When keratomalacia is said to be present, it means the hyperkeratotic epithelium has become soft. It
may become secondarily infected (* Corynebacterium xerosis, others) and even perforate.
Remember that in the absence of vitamin A, you can't make the pigment for rods. Night blindness
results.
Many governments, for their own dark reasons,
fail to implement or even allow public health measures that
would do a lot of good for very little money spent. Over half of the boys
in rural Ethiopia have Bitot's spots (East African Medical Journal 76: 590, 1999);
of course their growth is stunted and their vitamin A levels very low.
Cambodia: Arch. Ophth. 122: 517, 2004.
An amateur vegan family blinds its six-year-old son: Arch. Ophth. 122: 1228, 2004. More about
vegans: Clin. Ped. 43: 107, 2004.
* After years of delay because of anti-biotech activism, vitamin-A enriched rice
is now widely used and being welcomed by the world's poor: Nature Biotech. 21: 971, 2003.
TRACHOMA (Br. Med. J. 362: 223, 2001; Lancet 362: 223, 2003)
We've already discussed Chlamydia trachomatis, an important cause of blindness worldwide.
The pathology mostly involves lymphoid follicles on the conjunctival membrane. Later there is scarring.
If there is coexistent vitamin A deficiency, the infection is likely to be worse
(Lancet 357: 1676, 2001).
McCallan's stages of trachoma:
I: Follicles (i.e., lymphoid infiltrates) on the cornea, with early fibrosis
II: Debris-laden macrophages ("Leber cells") appear
III: Severe scarring; contraction produces an entropion
IV: The actual infection self-cures, since the damaged, opacified eye surface is no longer vulnerable to
infection.
CONJUNCTIVITIS
Trachoma's lesser chlamydial counterpart in the U.S. is swimming pool conjunctivitis (inclusion
conjunctivitis). Look for the characteristic inclusions on smears (* we suggest a Giemsa stain).
Bacterial conjunctivitis generally produces a red eye with purulent discharge. Think of gonorrhea,
pneumococci, staph (* I once endured this), and Hemophilus.
Classic ophthalmia neonatorum was gonococcal infection acquired in the birth canal. Silver nitrate,
erythromycin, and (now) povidone iodine (great for the poor nations) are prophylaxis (NEJM 332:
562 & 600, 1995).
Conjunctivitis can also be viral (remember adenovirus and measles), IgE-mediated (vernal
conjunctivitis, i.e., in the springtime allergy season; look for eosinophils), due to delayed
hypersensitivity (often cosmetics), due to injury or a foreign body, or due to ultraviolet light
(remember "snow blindness").
Remember that conjunctivitis from most causes can involve the cornea (keratoconjunctivitis). See
below. Unless you know the cause of the conjunctivitis, don't share towels....
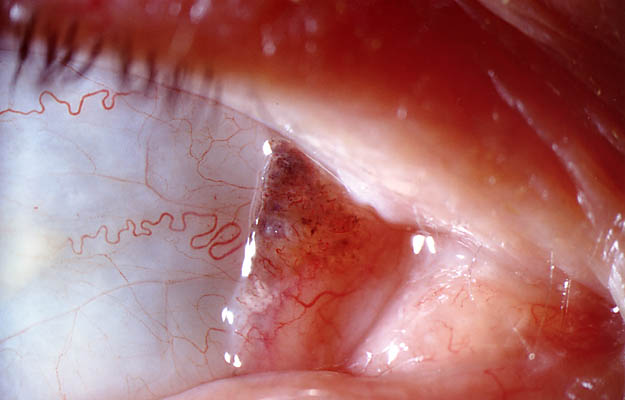
PINGUECULA AND PTERYGIUM
Pinguecula is fatty deposits in the conjunctiva, especially in people who've had lots of sun exposure.
Look near the nasal aspect of the limbus on both sides.
{5932} pinguecula
Pterygium ("wing") is more of the same, but extending over the cornea, obliterating Bowman's
membrane.
{21874} pterygium, gross
CORNEAL DISEASE
Remember the layers (from out to in): Epithelium, Bowman's membrane, stroma, Descemet's
membrane, endothelium.
Because there are no vessels here, once the cornea gets infected, it's serious. Especially in parts of
the world where treatment is not available, blindness often results.
Herpes simplex produces the familiar dendritic ulcers.
{14127} herpes keratitis
Acanthamoeba recently produced an epidemic among users of certain contact-lens solutions.
{22192} red eye from acanthamoeba
Kayser-Fleischer ring: copper deposit in Wilson's disease. Band
keratopathy: Hypercalcemia.
{21992} Kayser-Fleischer ring
*The corneal dystrophies, which render
the cornea opalescent due to faulty chemistry, include several hereditary problems.
Granular dystrophy -- autosomal dominant -- opacities
Lattice dystrophy -- autosomal dominant -- amyloid
Macular dystrophy -- autosomal recessive -- mucopolysaccharide
Also worth knowing: Fuch's -- leaky backside epithelium, with water bubbles
on the inner surface
Here's an example of one locus for several illnesses: BIGH3 can cause
lattice, granular, or other corneal dystrophies depending on
the mutation (Am. J. Hum. Genet. 62: 320, 1998). Why is this not
surprising, especially in the cornea?
{21935} granular dystrophy
If for some reason you wish to know more about amyloid on the cornea and elsewhere in the eye,
refer to Am. J. Ophth. 117: 529, 1994.
UVEAL DISEASE
Aniridia: No iris. Lots of problems with the eyes; many of these patients have a gene deletion that
extends to the nearby Wilms tumor locus (chromosome 11).
Albinism: The major problem these people face is excessive sensitivity of the eye to light.
Non-granulomatous uveitis is usually idiopathic, chronic inflammation.
Granulomatous uveitis (by contrast) has a long differential...
Infection
Bacteria: tularemia, syphilis, gonorrhea
Viruses: CMV, zoster
Fungi: various
Other: toxoplasmosis. (NOTE: Toxoplasmosis is an important disease of the eye. In the worst
cases, pathologists find patches of coagulation necrosis in retina and choroid.)
Odd immune diseases
Sarcoidosis
Ulcerative colitis and Crohn's disease
Reiter's and Behçet's syndromes
Sympathetic ophthalmia is probably an autoimmune reaction against one's own pigment epithelium
and retinal neurons following penetrating injury of one eye. Unfortunately, it involves both eyes,
and does great harm. Thankfully it is rare, but
the only sure prevention is to enucleate the injured eye within a week or two.
A white-knuckle management problem for ophthalmologists. The anatomic pathology:
Am. J. Ophth. 138: 475, 2004.
All about uveitis: Lancet 338: 1498 & 1501, 1991. Since material is seldom obtainable for study,
the antigens involved in the (surely immune-mediated) havoc remain largely unknown.
CATARACTS
A variety of opacities in the lens; nuclear sclerosis is the most common type seen in the aging lens.
{12428} cataract
Remember as causes of cataract:
radiation
long-term glucocorticoid therapy
hypoparathyroidism
congenital rubella
trauma
diabetes ("sorbitol snowflake cataract", others)
galactosemia
genes (* two loci, the crystallins, are known)
heavy sunlight exposure (Ophth. 108: 1400, 2001, minor risk)
While we're on the subject of lens disease, a displaced lens ("ectopia lentis") is one problem faced by
Marfan types.
{21999} ectopia lentis
RETROLENTAL FIBROPLASIA ("retinopathy of prematurity"; Ped. Clin. N.A. 50: 77, 2003)
The developing fetal retinal circulation, especially at its temporal margin, is selectively damaged by
high concentrations of oxygen. The vessels, which are sprouting from the optic disk, at first
constrict, then obliterate, so that the peripheral retina fails to vascularize. Several weeks after
cessation of oxygen therapy, vessels begin sprouting willy-nilly from the edge, and grow into the
vitreous; scar may contract and detach the retina, and there may be other problems.
This is a classic cause of blindness in premature infants treated with high concentrations of oxygen.
It became a major public health problem in the 1940's and early 1950's (my grammar school had a
girl a few years older than myself who had a full-time amanuensis). It became less troublesome
when oxygen concentrations were reduced, but has recurred now that very small babies are
surviving (a 600 gm baby tolerates even 90 mmHg of oxygen poorly).
HYPERTENSIVE AND ARTERIOSCLEROTIC (better, "arteriolosclerotic") RETINOPATHY
A common subject for discussion on rounds. Here's the system:
Hypertensive retinopathy: High blood pressure is bad for the vessels.
Grade I: The arterioles are a bit narrowed
Grade II: The arterioles are going into spasm somewhere
Grade III: There are bleeds
Grade IV: There is also edema of the optic disk, i.e., the hypertension has resulted in increased
intracranial pressure
{22018} hypertensive retinopathy with hemorrhages
Arteriosclerotic retinopathy: Due to progressive opacification of the arteries
Grade I: Widened light reflex due to "hyaline arteriolosclerosis", which renders the vessels
opalescent
Grade II: AV crossing defects; the hyaline wall of the artery makes it hard to see the vein underneath
Grade III: Copper wires; the blood doesn't show clearly through the arterial wall
Grade IV: Silver wires. The blood fails to show at all.
{22034} don't forget diabetic retinopathy, too
RETINITIS PIGMENTOSA
A heterogeneous group of diseases, mostly hereditary, in which the photoreceptor cells gradually die
off. Patients are first troubled by loss of peripheral vision, and later lose all sight. The rods are
typically lost before the cones ("night blindness", again).
There is proliferation of the pigment cells of the retina, typically along the vessels.
The molecular biology for the major autosomal dominant forms were worked out in the early
1990's. Around 1/3 of cases have a defective rhodopsin gene; some people with simple autosomal-dominant
night-blindness have
the same thing (Nature 367: 639, 1994), and vitamin A in fairly big
doses can help these folks.
*Other autosomal dominant syndromes are known (RP1, peripherin,
NRL: Br. J. Ophth. 86: 328, 2002).
In common (rhodopsin) retinitis pigmentosa, the defective rhodopsin accumulates
and kills the cells. Gene therapy now works in mice, and involves administering
a ribozyme (via a virus) that cleaves the defective gene's mRNA (Nat.
Med. 4: 967, 1998.)
Usher syndrome (retinitis pigmentosa and congenital nerve deafness) is often the myosin VII-A
locus.
Consider night blindness in children with unexplained fear of the dark.
{22074} retinitis pigmentosa
Stationary night blindness, i.e., the rods don't work but the cones work fine, has a variety of genetic
causes (Nat. Genet. 13: 358, 1996; update Am. J. Ophth. 135: 733, 2003).
Vitamin A deficiency is of course a better-known cause of night blindness,
but thankfully it is no longer common in the
U.S.
Night-vision goggles are now coming into use for people with night-blidness
(Inv. Op. 45: 1725, 2004).
RETINAL DETACHMENT
When the nerve-cell layers separate from the pigmentary epithelium, they lose their effective blood
supply, and degenerate over days or weeks.
Underlying causes are (1) contraction of scar within the vitreous (as after trauma, hemorrhage);
(2) exudation from inflamed or neoplastic tissue; (3) a hole in the retina, through which the vitreous
penetrates.
Important causes of retinal detachment include trauma, diabetes (from neovascularization of
vitreous), and marked nearsightedness (in which the eyeball is elongated and the retina stretched).
{22080} retinal detachment
MACULAR DEGENERATION
A family of diseases in which the nervous tissue of the macula degenerates, causing lost of central
vision.
The most troublesome is the common age-related macular degeneration (again, it's better not to call
it "senile"....) Look for drusen around the macula, and maybe some new vessels
in the choroid. Smoking clearly
brings it on faster. Whether sunlight exposure is really a risk factor
is far from clear ("maybe yes": Arch. Ophth. 119: 246, 2001;
"no": Arch. Ophth. 119: 1463, 2001; "actually less if there's
been heavy sun exposure" Ophth. 104: 770, 1997). Having blue eyes is at best
a minor risk (Ophth. 105: 1359, 1998).
Possibly zinc and anti-oxidants slows it down, vitamins C
and E and carotene flopped
("Age-Related Eye Disease Study", Arch. Ophth. 119: 1417 & 1439, 2001).
The most common gene for macular degeneration has been cloned, and it is a
forme fruste of a young-onset disease (* Stargardt's; gene
is ABCA4; Science 277: 1765, 1997). Several others are known:
NEJM 351: 346, 2004.
{22059} macular degeneration
{22062} macular degeneration
OPTIC NERVE
Optic neuritis has come to include any non-neoplastic cause of optic nerve dysfunction, from
methanol poisoning to ischemia to demyelination.
Devic's disease is full-thickness demyelination of an optic nerve.
GLAUCOMA
A family of diseases, their common feature being damage to the eye due to increased intraocular
pressure.
Open-angle glaucoma: Some problem, more or less mysterious, exists with drainage of aqueous
humor via the canal of Schlemm, despite apparently normal anatomy.
* The most important gene is
TIGR/MYOC/GLC1A, myocilin), a
trabecular
meshwork protein that in its mutated form gums up
the slits: Science 275: 668, 1997; NEJM 338;
1022, 1998; another gene optineurin Science 295: 1077, 2002).
Closed-angle glaucoma: Some people's anterior chamber is too shallow. As a result, the angle is too
acute, and the drainage of aqueous humor is compromised. This is exacerbated as the lens thickens
during later life.
Congenital glaucoma: Autosomal recessive (* a cytochrome C gene
component: Am. J. Ophth. 131: 345, 2001), or rubella.
Secondary glaucoma, the result of some other disease or injury to the eye, may be open-angle or
closed-angle.
The optic cup becomes wider and deeper, and the optic nerve and retina bear the brunt of the
troubles. "Big Robbins" suggests that the increased pressure causes disruption of the axoplasmic
flow where the axons lie over the edge of the deepened optic cup.
The major glaucoma gene, with many alleles of varying severity,
is GLC1a, on chromosome *1: NEJM 338: 1022, 1998.
{21990} optic nerve, glaucoma
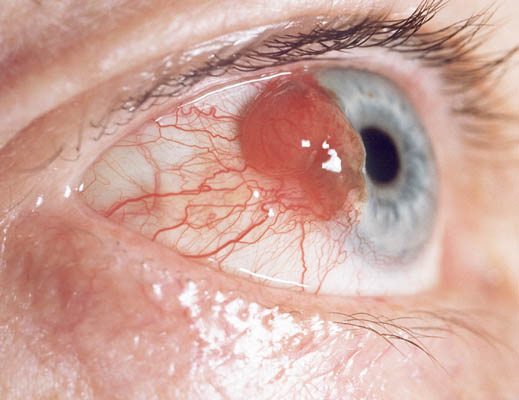
EYE TUMORS
Cancer of the conjunctiva and lids is usually squamous cell carcinoma. As with squamous cell
carcinoma of the skin, sunlight is a risk factor. The in situ phase is likely to appear as leukoplakia.
Remember melanomas can occur on the outer surface of the eye; they may be preceded by
"melanosis".
{21900} squamous cell carcinoma
Uveal melanoma, from the uveal melanocytes (not the pigment epithelium) is the most important
adult eye cancer. As with skin melanoma, this is most a problem for light-hued, sun-exposed people.
They range from masses on the iris to lesions hidden deep within the eyeball. These metastasize to
the liver, accounting for the old adage "Beware the patient with the glass eye and the large liver".
Don't worry about the arcane histopathology (which does affect survival).
{22162} melanoma
Retinoblastoma accounts for 1% of pediatric cancer deaths. This is another "tumor of small blue
cells"; like neuroblastomas, they often feature various "rosettes" (* even "real" ones without vessels
or fuzz in the center), often respond well to treatment, and a small percent undergo spontaneous
involution or maturation.
Remember the Rb anti-oncogene? Familial cases are typically multifocal (why?), and other tumors
(notably osteosarcomas) are also common in survivors.
{22149} retinoblastoma, gross
Basal cell carcinoma of the eyelids is classic. Optic nerve meningioma, and glioma (astrocytoma)
within the optic nerve, are additional eye tumors. Sebaceous carcinoma of the Meibomian glands is
a rarity. Other important orbital tumors include lymphomas in adults and embryonal
rhabdomyosarcoma in children.
{21862} sebaceous carcinoma
{22101} optic nerve glioma (astrocytoma)
* Future major ground wars will probably make heavy use of
weapons that blind the enemy soldiers. The weapons are already
in existence and work well. Blinded soldiers require more care
than dead people, and
blinding is demoralizing to military and civilians alike
(Br. Med. J. 315: 1392, 1997). In lawless eras,
blinding one's political enemies and prisoners of war
(sometimes en masse)
was fairly common, and was considered a humane alternative to
simply killing them. Of course, sending thousands of blinded
soldiers back to their homes is worse for the enemy's economy, too.
* In the African kleptocracies, many children are confined to
"charitable institutions for the blind" simply because they are
myopic and do not have glasses (Med. J. Aust. 167: 351, 1997).
I leave you to figure out the dark and corrupt politics responsible for
this travesty.
* Future pathologists:
When the heart stops, intraocular pressure (which largely
results from arterial pressure) drops by about half, and pressure
continues to drop over the following hours, imparting the
softness and deformability to the eyes of the dead.
1021-1040, 1042-1044 retina
 I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
Pathology Education Instructional Resource -- U. of Alabama; includes a digital library
Houston Pathology -- loads of great pictures for student doctors
Pathopic -- Swiss site; great resource for the truly hard-core
Syracuse -- pathology cases
Walter Reed -- surgical cases
Alabama's Interactive Pathology Lab
"Companion to Big Robbins" -- very little here yet
Alberta
Pathology Images --hard-core!
Cornell
Image Collection -- great site
Bristol Biomedical
Image Archive
EMBBS Clinical
Photo Library
Chilean Image Bank -- General Pathology -- en Español
Chilean Image Bank -- Systemic Pathology -- en Español
Connecticut
Virtual Pathology Museum
Australian
Interactive Pathology Museum
Semmelweis U.,
Budapest -- enormous pathology photo collection
Iowa Skin
Pathology
Loyola
Dermatology
History of Medicine -- National Library of Medicine
KU
Pathology Home
Page -- friends of mine
The Medical Algorithms Project -- not so much pathology, but worth a visit
National Museum of Health & Medicine -- Armed Forces Institute of Pathology
Telmeds -- brilliant site by the medical students of Panama (Spanish language)
U of
Iowa Dermatology Images
U Wash
Cytogenetics Image Gallery
Urbana
Atlas of Pathology -- great site
Visible
Human Project at NLM
WebPath:
Internet Pathology
Laboratory -- great site My team:
My team:Ed Lulo's Pathology Gallery
Bryan Lee's Pathology Museum
Dino Laporte: Pathology Museum
Tom Demark: Pathology Museum
Dan Hammoudi's Site
Claude Roofian's Site
Pathology Handout -- Korean student-generated site; I am pleased to permit their use of my cartoons
Estimating the Time of Death -- computer program right on a webpage
Pathology Field Guide -- recognizing anatomic lesions, no pictures

St.
Jude's Ranch for Children
I've spent time there and they are good. Write "Thanks
Ed" on your check.
PO Box 60100
Boulder City, NV 89006--0100
More of my notes
My medical students
Clinical
Queries -- PubMed from the National Institutes of Health.
Take your questions here first.
HealthWorld
Yahoo! Medline lists other sites that may work well for you

We comply with the
HONcode standard for health trust worthy
information:
verify
here. 

![]()
 Young men's love lies not in their hearts but in their eyes.
Young men's love lies not in their hearts but in their eyes.
-- Shakespeare, Romeo & Juliet
I caused to dwell within human beings hopes for things that they could not see.
{21863} normal fundus
 Eye Pathology
Eye Pathology
For allied health professionals
Many clinical photos on this site
Eye pathology site
Supply the definition for the "eye words" on the handout
Aniridia
Albinism
Bacterial and viral conjunctivitis
Basal cell carcinoma
Chalazion
Diabetic retinopathy
Glaucoma
Ectropion
Entropion
Keratitis (herpes, acanthamoeba)
Macular degeneration
Melanoma
Optic neuritis
Pinguecula / Pterygium
Retinal changes of vascular disease
Retinal detachment
Retinitis pigmentosa
Retinoblastoma
Retrolental fibroplasia
Sty
Sympathetic ophthalmia
Trachoma
Tay-Sachs
Vitamin A deficiency
 Eye pathology links
Eye pathology links
From a cyberfriend who
produces contact lenses
 SELECTED EYE WORDS
SELECTED EYE WORDS
* Do you remember the biochemistry? The X-linked
forms involved R-opsin (most protans have a mutation here)
and G-opsin (most deuterans have a mutation here).
{22832} drusen
)window.location='http://www.mdchoice.com/photo/img/img0078.jpg') Corneal abrasion
Corneal abrasion
Visualized by fluorescein
EMBBS
* Lisch nodules, little hamartomas, are usual in the iris of neurofibromatosis I patients.
 Chalazion (* Greek for hailstone) is chronic, usually granulomatous, inflammation of the sebaceous
(* "Meibomian") glands.
Chalazion (* Greek for hailstone) is chronic, usually granulomatous, inflammation of the sebaceous
(* "Meibomian") glands.
The World Health Organization "plans to eliminate trachoma by the year 2020"
by mass antibiotic use, twice a year in areas where the disease is prevalent
(Nat. Med. 5: 572, 1999).
{21876} pterygium, gross
{21879} pterygium, micro, oil red O stain for lipid
{21931} herpes keratitis
{22055} herpes, inclusion bodies
{21927} band keratopathy, gross
{21928} band keratopathy, micro, calcium dark blue
{21938} granular dystrophy
{21920} lattice dystrophy
{21957} lattice dystrophy, congo red
{21929} macular dystrophy, histology
{21932} macular dystrophy, histology
{22117} corneal transplant
{22121} corneal transplant
{22009} cataract
{22209} cataract
{22212} cataract
{22251} cataract
{22254} cataract; nuclear sclerosis
* Not surprisingly, the mechanism turns out to be suppression of VEGF-A production
in the retina. The details are being worked out (J. Clin. Invest. 112: 50, 2003).
 Retinitis pigmentosa
Retinitis pigmentosa
Prize photograph
Institute of Medical Illustrators
{22802} retinal detachment
{21993} optic nerve, glaucoma, micro
{21901} squamous cell carcinoma
{21894} carcinoma in situ, gross
{21898} carcinoma in situ, gross
{21895} carcinoma in situ, micro
{21899} squamous cell carcinoma, microscopic (good pearls)
{19377} amelanotic melanoma of the conjunctiva
 Squamous cell carcinoma
Squamous cell carcinoma
Eye pathology site
 Conjunctival melanosis
Conjunctival melanosis
Prize photograph
Institute of Medical Illustrators
 Conjunctival melanoma
Conjunctival melanoma
Prize photograph
Institute of Medical Illustrators
{22157} melanoma
{22636} melanoma
{22644} melanoma
{21873} melanoma
{21917} melanoma
{21918} melanoma
{22141} retinoblastoma, gross
{22146} retinoblastoma, micro
Basal cell carcinoma
Eye pathology site
B-cell lymphoma
In the eyelid
Loyola Med
{21864} sebaceous carcinoma
{21865} sebaceous carcinoma, oil-red O stain (sebum)
{22113} rhabdomyosarcoma
{22114} rhabdomyosarcoma
{22115} rhabdomyosarcoma
* For
your reading enjoyment: Blindness is a perennial symbol for spiritual darkness. See
Oedipus the King,
and the New
Testament ("Light of the body", "Blind leading the blind"), Shakespeare's
King Lear,
Goethe's Faust
(at the end), Robert Lewis Stevenson's Treasure Island
(Blind Pew), Yeats's "On Baile's Strand" & "The Cat and
the Moon", hymn "Amazing Grace", "The Blind Men and the Elephant" (re-read that last verse),
cartoon "Mr. Magoo's Christmas Carol" (Scrooge isn't a bad man, he's a blind man), others. For the
opposite view, see John Milton's sonnet "On His Blindness", and Paradise Lost Book III vv. 1 ff.;
Ibsen's Solveig ("Peer Gynt") is blind to Peer's faults, which is how Peer eventually discovers his
"real self"; the Mountain King ("In the Hall of the") offers Peer eye surgery so that he will see ugly
("Be selfish") as beautiful ("Be yourself").

)window.location='http://www.mdchoice.com/photo/img/img0085.jpg') Subconjunctival hemorrhage
Subconjunctival hemorrhage
EMBBS
)window.location='http://www.mdchoice.com/photo/img/img0083.jpg') Ruptured eyeball
Ruptured eyeball
Car wreck
EMBBS
)window.location='http://artchive.com/artchive/G/goya/goya_blind_guitarist.jpg.html') *SLICE OF LIFE REVIEW
*SLICE OF LIFE REVIEW
{15065} eye, human
{15066} eye, human
{15067} iris and lens, normal
{15067} iris and lens, normal
{15068} iris and lens, normal
{15068} iris and lens, normal
{15069} ciliary body, normal
{15069} ciliary body, normal
{15070} ciliary body, normal
{15070} ciliary body, normal
{15071} retina (cross section), normal
{15071} retina (cross section), normal
{15072} retina (cross section), normal
{15072} retina (cross section), normal
{15073} photoreceptor cells, normal
{15073} photoreceptor cells, normal
{15074} photoreceptor cells, normal
{15074} photoreceptor cells, normal
{15075} fovea, normal
{15075} fovea, normal
{15076} fovea, normal
{15076} fovea, normal
{15083} lens and iris, normal
{15083} lens and iris, normal
{15084} lens and iris, normal
{15084} lens and iris, normal
{15312} meibomian gland, normal
{15312} meibomian gland, normal
{20715} ciliary process, normal eye
{20716} optic nerve head and retina, normal
{21802} eye, normal anatomy
{21804} eye, normal anatomy
{21805} eye, normal anatomy
{21806} eyelid, normal anatomy
{21808} eyelid, normal anatomy
{21812} eye, normal eye
{21821} anterior chamber angle, normal ant. chamber angle
{21828} canal of schlemm, normal
{21830} canal of schlemm, normal
{21836} cornea, normal cornea
{21839} cornea, normal cornea
{21842} cornea, normal
{21845} limbus, normal limbus
{21860} fundus, normal optic disk and macula
{21863} fundus, normal optic disk and macula
{21869} optic disc, normal
{21872} optic disc, normal
{21881} retina, normal retina
{21884} retina, normal retina
{21905} lens, normal human lens
{21908} zonular fibers of lens, normal zonules attaching to lens
{21909} melanosis, primary acquired
{21914} cornea, normal cornea
{21916} cornea, normal cornea
{21922} cornea, normal anatomy
{21924} cornea, normal anatomy
{21925} cornea, normal anatomy
{21974} glaucoma, normal anterior chamber ingle
{21976} glaucoma, normal anterior chamber angle
{21977} glaucoma, normal anterior chamber angle
{21996} lens, normal anatomy
{21997} lens, normal anatomy
{22014} retina, normal
{22015} retina, normal
{22017} retina, normal
{22083} optic nerve, normal anatomy
{22391} retina, normal
{22403} fundus, normal eye
{22418} optic disc, normal
{22535} choroid of eye, normal
{23144} fundus, normal
{46438} ciliary body, normal
{46515} diabetic retinopathy, norma


| Visitors to www.pathguy.com reset Jan. 30, 2005: |
Ed says, "This world would be a sorry place if
people like me who call ourselves Christians
didn't try to act as good as
other
good people
."
Prayer Request
 Teaching Pathology
Teaching Pathology
PathMax -- Shawn E. Cowper MD's
pathology education links
Ed's Autopsy Page
Notes for Good Lecturers
Small Group Teaching
Socratic
Teaching
Preventing "F"'s
Classroom Control
"I Hate Histology!"
Ed's Physiology Challenge
Pathology Identification
Keys ("Kansas City Field Guide to Pathology")
Ed's Basic Science
Trivia Quiz -- have a chuckle!
Rudolf
Virchow on Pathology Education -- humor
Curriculum Position Paper -- humor
The Pathology Blues
 Ed's Pathology Review for USMLE I
Ed's Pathology Review for USMLE I
![]()
![]()
 | Pathological Chess |
 |
Taser Video 83.4 MB 7:26 min |

 Eye photos
Eye photos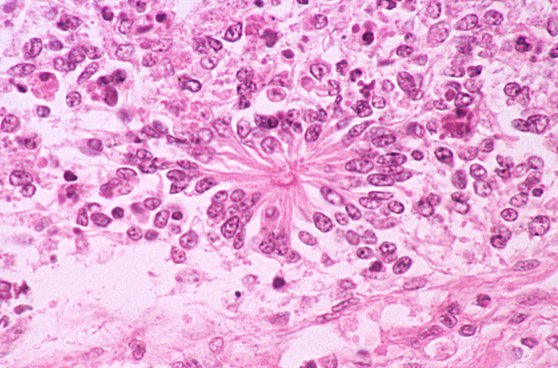 Flexner "True" Rosette
Flexner "True" Rosette