Ed Friedlander, M.D., Pathologist
scalpel_blade@yahoo.com



Cyberfriends: The help you're looking for is probably here.
Welcome to Ed's Pathology Notes, placed here originally for the convenience of medical students at my school. You need to check the accuracy of any information, from any source, against other credible sources. I cannot diagnose or treat over the web, I cannot comment on the health care you have already received, and these notes cannot substitute for your own doctor's care. I am good at helping people find resources and answers. If you need me, send me an E-mail at scalpel_blade@yahoo.com Your confidentiality is completely respected.
 DoctorGeorge.com is a larger, full-time service.
There is also a fee site at myphysicians.com,
and another at www.afraidtoask.com.
DoctorGeorge.com is a larger, full-time service.
There is also a fee site at myphysicians.com,
and another at www.afraidtoask.com.
Translate this page automatically
 |
With one of four large boxes of "Pathguy" replies. |
 I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
Numbers in {curly braces} are from the magnificent Slice of Life videodisk. No medical student should be without access to this wonderful resource. Someday you may be able to access these pictures directly from this page.
Also:
Medmark Pathology -- massive listing of pathology sites
Freely have you received, freely give. -- Matthew 10:8. My
site receives an enormous amount of traffic, and I'm
handling about 200 requests for information weekly, all
as a public service.
Pathology's modern founder,
Rudolf
Virchow M.D., left a legacy
of realism and social conscience for the discipline. I am
a mainstream Christian, a man of science, and a proponent of
common sense and common kindness. I am an outspoken enemy
of all the make-believe and bunk which interfere with
peoples' health, reasonable freedom, and happiness. I
talk and write straight, and without apology.
Throughout these notes, I am speaking only
for myself, and not for any employer, organization,
or associate.
Special thanks to my friend and colleague,
Charles Wheeler M.D.,
pathologist and former Kansas City mayor. Thanks also
to the real Patch
Adams M.D., who wrote me encouragement when we were both
beginning our unusual medical careers.
If you're a private individual who's
enjoyed this site, and want to say, "Thank you, Ed!", then
what I'd like best is a contribution to the Episcopalian home for
abandoned, neglected, and abused kids in Nevada:
My home page
Especially if you're looking for
information on a disease with a name
that you know, here are a couple of
great places for you to go right now
and use Medline, which will
allow you to find every relevant
current scientific publication.
You owe it to yourself to learn to
use this invaluable internet resource.
Not only will you find some information
immediately, but you'll have references
to journal articles which you can obtain
by interlibrary loan, plus the names of
the world's foremost experts and their
institutions.
Alternative (complementary) medicine has made real progress since my
generally-unfavorable 1983 review linked below. If you are
interested in complementary medicine, then I would urge you
to visit my new
Alternative Medicine page.
If you are looking for something on complementary
medicine, please go first to
the American
Association of Naturopathic Physicians.
And for your enjoyment... here are some of my old pathology
exams
for medical school undergraduates.
I cannot examine every claim which my correspondents
share with me. Sometimes the independent thinkers
prove to be correct, and paradigms shift as a result.
You also know that extraordinary claims require
extraordinary evidence. When a discovery proves to
square with the observable world, scientists make
reputations by confirming it, and corporations
are soon making profits from it. When a
decades-old claim by a "persecuted genius"
finds no acceptance from mainstream science,
it probably failed some basic experimental tests designed
to eliminate self-deception. If you ask me about
something like this, I will simply invite you to
do some tests yourself, perhaps as a high-school
science project. Who knows? Perhaps
it'll be you who makes the next great discovery!
Our world is full of people who have found peace, fulfillment, and friendship
by suspending their own reasoning and
simply accepting a single authority which seems wise and good.
I've learned that they leave the movements when, and only when, they
discover they have been maliciously deceived.
In the meantime, nothing that I can say or do will
convince such people that I am a decent human being. I no longer
answer my crank mail.
This site is my hobby, and I presently have no sponsor.
This page was last updated February 6, 2006.
During the ten years my site has been online, it's proved to be
one of the most popular of all internet sites for undergraduate
physician and allied-health education. It is so well-known
that I'm not worried about borrowers.
I never refuse requests from colleagues for permission to
adapt or duplicate it for their own courses... and many do.
So, fellow-teachers,
help yourselves. Don't sell it for a profit, don't use it for a bad purpose,
and at some time in your course, mention me as author and KCUMB as my institution. Drop me a note about
your successes. And special
thanks to everyone who's helped and encouraged me, and especially the
people at KCUMB
for making it possible, and my teaching assistants over the years.
Whatever you're looking for on the web, I hope you find it,
here or elsewhere. Health and friendship!
QUIZBANK: Respiratory #'s 43-65, 150-169
Describe the origin, importance, and harmful effects of tobacco addiction. Describe factors that
perpetuate it, and proposed remedies.
Describe what happens to particles of various shapes and sizes when they are inhaled.
Distinguish the inorganic and organic pneumoconioses. Distinguish harmful and innocuous
inorganic dusts, and list some of each kind.
Describe groups at risk, gross and microscopic pathology, pathophysiology, clinical picture, and
important complications of each of the following inorganic pneumoconioses:
coal worker's pneumoconiosis
Describe medicolegal aspects of coal worker's pneumoconiosis and asbestosis. Explain why this
subject is so complex.
Describe the typical clinical settings, pathophysiology, and means of diagnosis for the important
organic pneumoconioses.
 I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
Pathology Education Instructional Resource -- U. of Alabama; includes a digital library
Houston Pathology -- loads of great pictures for student doctors
Pathopic -- Swiss site; great resource for the truly hard-core
Syracuse -- pathology cases
Walter Reed -- surgical cases
Alabama's Interactive Pathology Lab
"Companion to Big Robbins" -- very little here yet
Alberta
Pathology Images --hard-core!
Cornell
Image Collection -- great site
Bristol Biomedical
Image Archive
EMBBS Clinical
Photo Library
Chilean Image Bank -- General Pathology -- en Español
Chilean Image Bank -- Systemic Pathology -- en Español
Connecticut
Virtual Pathology Museum
Australian
Interactive Pathology Museum
Semmelweis U.,
Budapest -- enormous pathology photo collection
Iowa Skin
Pathology
Loyola
Dermatology
History of Medicine -- National Library of Medicine
KU
Pathology Home
Page -- friends of mine
The Medical Algorithms Project -- not so much pathology, but worth a visit
National Museum of Health & Medicine -- Armed Forces Institute of Pathology
Telmeds -- brilliant site by the medical students of Panama (Spanish language)
U of
Iowa Dermatology Images
U Wash
Cytogenetics Image Gallery
Urbana
Atlas of Pathology -- great site
Visible
Human Project at NLM
WebPath:
Internet Pathology
Laboratory -- great site My team:
My team:Ed Lulo's Pathology Gallery
Bryan Lee's Pathology Museum
Dino Laporte: Pathology Museum
Tom Demark: Pathology Museum
Dan Hammoudi's Site
Claude Roofian's Site
Pathology Handout -- Korean student-generated site; I am pleased to permit their use of my cartoons
Estimating the Time of Death -- computer program right on a webpage
Pathology Field Guide -- recognizing anatomic lesions, no pictures

St.
Jude's Ranch for Children
I've spent time there and they are good. Write "Thanks
Ed" on your check.
PO Box 60100
Boulder City, NV 89006--0100
More of my notes
My medical students
Clinical
Queries -- PubMed from the National Institutes of Health.
Take your questions here first.
HealthWorld
Yahoo! Medline lists other sites which may work well for you

We comply with the
HONcode standard for health trust worthy
information:
verify
here. 

![]()
 LEARNING OBJECTIVES
LEARNING OBJECTIVES
silicosis
asbestosis
berylliosis
Sublime tobacco! which from east to west
Cheers the tar's labor or the Turkman's rest;...
Divine in hookas, glorious in a pipe,...
Yet thy true lovers more admire by far
Thy naked beauties -- Give me a cigar!
--Lord Byron (1788-1824) The Island II.19
... And for the vanities committed in this filthy custom, is it not both great vanity and uncleanness, that at the table, a place of respect, of cleanliness, of modesty, men should not be ashamed, to sit tossing of tobacco pipes, and puffing of the smoke of tobacco one to another, making the filthy smoke and stink thereof, to exhale across the dishes, and infect the air, when very often men that abhor it are at their repast?... It makes a kitchen also often-times in the inward parts of men, soiling and infecting them, with an ... oily kind of soot, as has been found in some great tobacco takers, that after their death were opened.... Have you not reason then to be ashamed and to forbear this filthy novelty ... a custom loathsome to the eye, hateful to the nose, harmful to the brain, dangerous to the lungs, and in the black stinking fume thereof, nearest resembling the horrible Stygian smoke of the Pit that is bottomless....?
-- King James I of England (1566-1625)
The incessant, witless repetition of advertisers' moron-fodder has become so much a part of life that if we are not careful, we forget to be insulted by it.
-- The Times of London
|
Some years ago a model named David Goerlitz told me that while posing for a Winston ad he had asked a group of R.J. Reynolds executives if any of them smoked. He said one of them replied: "Are you kidding? We reserve that right for the poor, the young, the black, and the stupid." -- Bob Herbert, New York Times columnist, 1998 |

|
TOBACCO SMOKING: Med. Clin. N.A. 76: 355, 1992. Here are some facts you may find handy in talking with patients.
Tobacco was discovered by the American Indians, and has been described as their revenge. The addictive leaves were smoked in pipes, called tobaccos, which gave the plant its European name. Early explorers introduced tobacco to the rest of the world. No country has ever been able to rid itself of tobacco -- even when tobacco use has been a capital crime. With widespread smoking of cigarets (today's preferred spelling of "cigarettes"), previously-rare diseases such as lung cancer and emphysema became common. Even Hitler and his people recognized that smoking was highly addictive and explained the new epidemic of lung cancer, and as part of their "purity" campaign undertook a strong anti-tobacco campaign (Br. Med. J. 313: 1450, 1996); the German tobacco industry called this "unscientific". Cigaret smoking is now a major problem throughout the world. Mainland China has the world's highest cigaret consumption per capita. The role of the U.S. in all this is troubling: Thorax 46: 153, 1991. In Singapore, they're now caning anybody under 18 caught doing tobacco ("Good" says Ed; Br. Med. J. 313: 636, 1996).
 Today,
tobacco smoke is the most widespread of the known pollutants. In developed countries,
ethanol and tobacco are the two principal causes of avoidable death. Surgeon General Koop called
cigaret smoking "the chief, single, avoidable cause of death in our society and the most important
public health problem of our time." (I'd have voted for alcoholism on the second point, but it's
close....) Tobacco smoking kills 1000 people in the US each day. Mortality rates for young and
middle-aged cigaret smokers is 1.7 x that of nonsmokers. By taking up smoking, a person cuts his
or her life expectancy by 15 years (JAMA 258: 2080, 1987); the estimate of "5 minutes of life lost
for every cigaret" is probably low.
Today,
tobacco smoke is the most widespread of the known pollutants. In developed countries,
ethanol and tobacco are the two principal causes of avoidable death. Surgeon General Koop called
cigaret smoking "the chief, single, avoidable cause of death in our society and the most important
public health problem of our time." (I'd have voted for alcoholism on the second point, but it's
close....) Tobacco smoking kills 1000 people in the US each day. Mortality rates for young and
middle-aged cigaret smokers is 1.7 x that of nonsmokers. By taking up smoking, a person cuts his
or her life expectancy by 15 years (JAMA 258: 2080, 1987); the estimate of "5 minutes of life lost
for every cigaret" is probably low.
Tobacco smoke is a complex mixture that contains nicotine (the addictive component) and many other harmful substances, including carbon monoxide, benzopyrene (* mutates ras codon 12 G-->T; Cancer 72: 432, 1993), nickel, polonium, and radon. "Low-tar" and "low nicotine" cigarets are not measurably less dangerous than the regular kind (Am. J. Pub. Health 77: 546 & 685, 1987). Smoking without inhaling (pipes, cigars) is less addictive and easier on the lungs, but the risk of mouth and throat cancer is high.
"Smokeless tobacco" ("spit tobacco") is as addictive as cigarets. The average age at which an American begins "chewing tobacco" is now ten (JAMA 266: 3143, 1991). Tobacco companies make "starter" (low-nicotine, nice flavors) chewing tobacco products targeted at kids, who then graduate to the more familiar products. And every school kid knows that chewing tobacco and snuff are much safer in the long-term than smoking. (If anti-tobacco education really was concerned with telling the whole truth and saving lives, rather than "teaching values", we'd encourage teens who cannot quit using tobacco to switch to smokeless tobacco. But this is politics.) Snuff produces a trademark mutation in p53 (Int. J. Cancer 81: 527, 1999), and a variety of curious benign mucosal lesions (which often appear within a few days after beginning smokeless tobacco use), and occasionally causes a mouth cancer (same genes mutated as in smokers' mouth cancer: Cancer 83: 204, 1998... one has to wonder whether this really demonstrates cause and effect). The risk of getting cancer from chewing is much less than is generally supposed (Oral Surg Oral Path 86: 697, 1998). No surprise. Apart from some nitrosamines, the noted carcinogens in tobacco smoke are products of combustion. Cardiovascular effects of snuff, at least in Sweden (Reg. Tox. Pharm. 28: 1, 1998; J. Am. Coll. Card. 34: 1784, 1999), are conspicuous by their absence: nor does Swedish snuff produce any measurable increased risk of cancer (Cancer 82: 1367, 1998). A study of baseball players, about half of whom use smokeless tobacco, showed that it was bad for their gums and teeth (gee whiz) but produced no difference in athletic performance (ooh, Abstract 98185116; no cancers either). Smokeless tobacco does not impair middle-aged men's exercise abilities (Eur. J. Clin. Inv. 27: 427, 1997). But if you are not already physically addicted to nicotine, using smokeless tobacco has nothing to recommend it.
What happens to tobacco smokers? You will learn about the anatomic lung pathology of uncomplicated cigaret smoking later in the course. After high serum cholesterol, cigaret smoking is the most important risk factor for coronary heart disease (heart attacks, sudden death, angina pectoris -- see Chest 94: 449, 1988) and other complications of atherosclerosis (including ruptured aortic aneurysms and strokes -- for the latter, see Lancet 2: 643, 1989). Smoking lowers HDL ("good") cholesterol; nobody knows how. Chronic bronchitis and emphysema (together, "chronic obstructive pulmonary disease") kill 150,000 people in the US each year. Lung cancer kills around 170,000 people in the US each year. Most patients who get the disease die of it. The vast majority of these cancers are caused by cigaret smoking. Mouth cancer, throat cancer, larynx cancer, and esophageal cancer are all much more common in tobacco smokers. Bladder cancer rates are roughly tripled for cigaret smokers. Pancreatic cancer and kidney cancer rates are at least doubled for cigaret smokers. Leukemia and plasma cell myeloma are also probably increased in smokers. We are now zeroing in on the molecular biology on oncogenesis on these cancers, which seem to result, at least in part, from mutations which carcinogens in tobacco cause. Smoking and cancer: Am. J. Med. 93(1A): 13S-17S, 1992. Tobacco mutates p53 (gee whiz NEJM 332: 712, 1995).
Peptic ulcer disease is especially common in cigaret smokers. Cigaret smoking accounts for an extra 15,700 cases of stroke among U.S. men each year (accelerated atherosclerosis and hypercoagulable blood: NEJM 316: 628, 1987; also Am. J. Med. 149: 2053, 1989). Buerger's disease is a (fortunately rare) disease of young male smokers, who develop gangrene of their hands and feet. Osteoporosis in women is also exacerbated by smoking, and tobacco will rob a woman of 5-10% of her total bone mass over a lifetime (NEJM 330: 387, 1994). It increases your risk for rheumatoid arthritis, probably (Arth. Rheum. 39: 732, 1996). The majority of household fires are caused by cigaret smoking. In Cuban epidemic neuropathy (1991-1993), tobacco combined with malnutrition (no thanks Fidel) to cause a grisly disease, and tobacco amblyopia (i.e., going blind from it) is probably a sporadic variant. Rear-end collisions often result from "acts of smoking" (i.e., fumbling for your tobacco, lighting, flicking, etc.: JAMA 273: 1334, 1995). And smoking causes gum disease, bad breath, and stained teeth. (An unusually candid RJR dealer once acknowledged on TV that tobacco smoking "may" cause stained teeth "in predisposed individuals".) In a study with an obvious flaw ("it's dumb to smoke, and being dumb could be hereditary"), mothers who smoked during pregnancy gave birth to kids with persistently far-lower IQ's (Pediatrics 93:221, 1994), but the "definite maybe" that this causes brain damage in the unborn child is still alarming. And we now know it greatly accelerates wrinkling of the skin (Ann. Int. Med. 114: 840 & 900, 1991). A strong statistical relationship between parents' smoking and kids' tooth decay (JAMA 289: 1258, 2003) seems harder to believe; even though this is after controlling for frequency of dental visits and all the usual socioeconomic stuff, maybe parents who blow smoke on their kids also care less about their teeth-brushing and candy consumption.
 During the 1950's (people still idealize the
"family values" era),
popular ads showed
physicians endorsing particular brands of cigarets,
and it was considered
very rude to complain if somebody blew smoke in your face in public.
Today, there is no longer any reasonable doubt that passive smoking (inhaling someone else's cigaret
smoke) is dangerous.
It is hard to know how many people die as a result of second-hand smoke,
but
histopathologists may examine JAMA 268: 1697. 1992). Parents' smoking and children's health: Am. Rev.
Resp. Dis. 133: 959, 1986; spouses' health: Am. J. Pub. Health 77: 548, 1987;
smoking and children's asthma Chest 122: 409, 2002; one problem with this kind of
work is controlling for the fact that any adult who'd smoke around his/her asthmatic kid
probably doesn't take good care of the kid in general. More: Arch. Ped. Adol. Med. 151:
135, 1997. In New Zealand, they're monitoring
nicotine levels in kids' hair to see whether the parents smoke around them (Arch. Env. Health 56: 117, 2001).
The impact of passing smoking
on coronary disease (if real) is probably small: NEJM 340:
920, 1999 (the literature is full of people still trying to show an effect.)
The EPA (Am. J.
Med. 93(1A): 38-S, 1992) decided that second-hand smoke
kills 53,000 Americans yearly (which is
plain silly, as EPA pronouncements so often are).
Philip Morris fought back with a campaign calling this "junk science",
but ended up quietly admitting that environmental smoke could indeed cause
lung cancer (Am. J. Pub. Health. 91: 1742, 2001).
But the push to a smoke-free
workplace is laudable. In the mid-1990's, the ethics
circus included a proposed ban
on smokers adopting babies.
During the 1950's (people still idealize the
"family values" era),
popular ads showed
physicians endorsing particular brands of cigarets,
and it was considered
very rude to complain if somebody blew smoke in your face in public.
Today, there is no longer any reasonable doubt that passive smoking (inhaling someone else's cigaret
smoke) is dangerous.
It is hard to know how many people die as a result of second-hand smoke,
but
histopathologists may examine JAMA 268: 1697. 1992). Parents' smoking and children's health: Am. Rev.
Resp. Dis. 133: 959, 1986; spouses' health: Am. J. Pub. Health 77: 548, 1987;
smoking and children's asthma Chest 122: 409, 2002; one problem with this kind of
work is controlling for the fact that any adult who'd smoke around his/her asthmatic kid
probably doesn't take good care of the kid in general. More: Arch. Ped. Adol. Med. 151:
135, 1997. In New Zealand, they're monitoring
nicotine levels in kids' hair to see whether the parents smoke around them (Arch. Env. Health 56: 117, 2001).
The impact of passing smoking
on coronary disease (if real) is probably small: NEJM 340:
920, 1999 (the literature is full of people still trying to show an effect.)
The EPA (Am. J.
Med. 93(1A): 38-S, 1992) decided that second-hand smoke
kills 53,000 Americans yearly (which is
plain silly, as EPA pronouncements so often are).
Philip Morris fought back with a campaign calling this "junk science",
but ended up quietly admitting that environmental smoke could indeed cause
lung cancer (Am. J. Pub. Health. 91: 1742, 2001).
But the push to a smoke-free
workplace is laudable. In the mid-1990's, the ethics
circus included a proposed ban
on smokers adopting babies.
It is very difficult to quit, and people have done so deserve our congratulations. Quitting smoking greatly and quickly improves one's chance of a long and healthy life. The risk of sudden cardiac death drops almost to baseline immediately, while the risk of heart attack and lung cancer return to baseline over the next several years (NEJM 322: 213, 1990). Only the changes of emphysema are known to be irreversible.
 Defenses of tobacco smoking are ingenious but flawed, and closely resemble other forms of
junk science / pseudoscience. (See, for example, "Dr. Oat Cell"'s letter, JAMA 255: 1016, 1986.) Even the
scientists who get their grant money from the tobacco companies ("The Council on Tobacco
Research") are pretty much unanimous in agreeing that smoking obviously causes disease (Am. J.
Pub. Health. 81: 894, 1991). People don't smoke "because they like the taste" -- if they did, you
could buy tobacco-flavored ice cream at "31 Flavors". People smoke because they are physically
addicted to nicotine (see Chest 93(2S), 1988; the withdrawal syndrome is as severe as drugs that
actually give pleasure, see JAMA 261: 898, 1989). Most addicts started smoking as teenagers, in
order to assert their "independence" and as a sign of "maturity". The majority are never able to
quit. Addicts cannot really exercise "freedom of choice". There is not a shred of evidence for "a
gene to like cigarets" that also causes all cigaret-related diseases. There is no evidence, either, that
smokers are self-medicating for a primary deficiency in certain neurotransmitters.
Defenses of tobacco smoking are ingenious but flawed, and closely resemble other forms of
junk science / pseudoscience. (See, for example, "Dr. Oat Cell"'s letter, JAMA 255: 1016, 1986.) Even the
scientists who get their grant money from the tobacco companies ("The Council on Tobacco
Research") are pretty much unanimous in agreeing that smoking obviously causes disease (Am. J.
Pub. Health. 81: 894, 1991). People don't smoke "because they like the taste" -- if they did, you
could buy tobacco-flavored ice cream at "31 Flavors". People smoke because they are physically
addicted to nicotine (see Chest 93(2S), 1988; the withdrawal syndrome is as severe as drugs that
actually give pleasure, see JAMA 261: 898, 1989). Most addicts started smoking as teenagers, in
order to assert their "independence" and as a sign of "maturity". The majority are never able to
quit. Addicts cannot really exercise "freedom of choice". There is not a shred of evidence for "a
gene to like cigarets" that also causes all cigaret-related diseases. There is no evidence, either, that
smokers are self-medicating for a primary deficiency in certain neurotransmitters.
Our laws governing tobacco are "peculiar". The laws protecting US citizens from dangerous products all contain specific exemptions for tobacco. Before the 1997 compromise, the words addictive and death were kept off tobacco warning labels, as a compromise with dealers. We have banned heroin, cocaine, cyclamates, many useful drugs, lawn darts, and pet turtles, but we subsidize and advertise tobacco and allow smoking in public. Some (not all) conservatives shout for more and tougher penalties for the recreational drugs, while sporting "Smokers' Rights" bumper stickers. Advertising by tobacco dealers is a multi-billion dollar industry (NEJM 311: 725, 1987). The Camel mnanufacturers actually sued the physician who did a study intended to show that Joe Camel appealed primarily to children (JAMA 266: 3143, 1991); of course in 1999, the Marlboro Man rode Joe into the sunset. The Minnesota Tobacco Trial documents are a good read: JAMA 280: 1173, 1998. Today, tobacco advertisers are making a special effort to target minority youth, especially Hispanics, blacks, and gays (Am. J. Pub. Health 92: 1086, 2002), and to young people going to bars, where they are going to take up drinking and are most susceptible to taking up other "adult" habits as well (Am. J. Pub. Health 92: 75, 2002). U.S. tobacco companies presently give cigarets to minority youths in the US at sponsored "youth events" and to children in the poor nations as "gifts", i.e., to get them addicted. Perhaps there's some good news ... Mainland China was the heaviest-smoking country in the late 20th century, but if we're to believe the Red Chinese (uh, sure), only 1 in 300 of their high school students are presently smokers Am. J. Pub. Health 91: 1653, 2001. The cost to the U.S. of cigarets in terms of lost productivity is estimated at $53.7 billion per year (Onc. Times 9(9): 5, 1987). Of course, this ignores savings generated by cigarets -- specifically, in old-age care and pensions that smokers never use! (I suspect this is why tobacco is not more closely regulated!) Perhaps most disturbing of all, U.S. "fair trade" treaties with third world nations restrict their attempts to prevent their citizens from smoking (Am. J. Pub. Health 80: 659, 1990). Despite the grandstanding of the 1997-8 settlement ("Protect children!"), don't expect this to change. Follow-up on the "settlement": Am. J. Pub. Health. 94: 218, 2004.
In spite of all this, however, most adults today know that tobacco is highly addictive and lethal. U.S. men are smoking less, and the incidence of lung cancer in men is finally starting to go down. Cigaret smoking, once macho, is now a teenaged girl's vice. The most successful stop-smoking campaigns are run by industry. Each smoking worker costs industry several hundred dollars extra per year.
 The most effective anti-smoking ads directed for young people
are the ones which remind them "The tobacco companies are playing
you for a fool" (JAMA 279: 772, 1998).
The most effective anti-smoking ads directed for young people
are the ones which remind them "The tobacco companies are playing
you for a fool" (JAMA 279: 772, 1998).
Health care professionals are natural leaders in the fight against tobacco. Today only around 20% of physicians and 20% of nurses are tobacco smokers -- way down from previous decades. There are many packages to help your patients quit. The skin patch is now over-the-counter, and nicotine (though of course "evil") itself does not seem to be a problem for heart patients, who can use the patch safely (NEJM 337: 1230, 1997). Doxepin and clonidine both ease withdrawal, and "Zyban" became a sensation in 1998. There's also "Nicotrol" nicotine nasal spray (Mayo Clin. Proc. 73: 118, 1998; "the patch for 5 months and the spray for a year" BMJ 318: 285, 1999). Bupropion and/or patch: NEJM 340: 685, 1999.
If you believe that a physician's job is to improve the health of his or her patients, you will want to talk to them about smoking. If you take two minutes to urge a patient to stop smoking, he or she is around 50% likely to eventually quit. (See also Am. J. Pub. Health 77: 313 & 782, 1987; JAMA 259: 2882 & 2883, 1988). Comparisons of three stop-smoking clinics: Am. J. Pub. Health. 80: 554, 1990. To quantitate tobacco smoke exposure in your research, measure urinary cotinine (Thorax 45: 356, 1990). To measure oxidative damage to a person, measure serum F2-isoprostane: yes, cigarets greatly increase it (NEJM 332, 1995).
|
|
THE PNEUMOCONIOSES: A group of diseases, ancient and modern, resulting from dust inhalation. (* Conios means "dust" in Greek.) Occupational lung disease: Disease-A-Month 44: 41, 1998.
Dust elimination by the respiratory tree:
Particles over 5 microns are caught in the upper airways and eliminated on the mucociliary elevator
Particles under 1 micron either are not deposited or are deposited diffusely on the alveolar surfaces
Particles 1-3 microns in size tend to be deposited at the level of the respiratory bronchioles because of the sudden decrease in air velocity at this level. (These particles are the most dangerous.)
The pneumoconioses tend to involve the upper lobes more than the lower lobes, because more air goes to the upper lobes (why?)
Exception: long, thin fibers (i.e., asbestos) end up carried by the wind to alveolar duct bifurcations, where they penetrate the tissue and work their way through the lung parenchyma.
Mechanisms of dust removal from the respiratory bronchioles and alveoli include transport on surfactant and in lymphatics and/or phagocytosis by wandering macrophages.
Inorganic pneumoconioses:
Chronic diseases, typically with pulmonary fibrosis.
Silicosis, asbestosis, berylliosis, and complicated forms of coal workers' pneumoconiosis have caused widespread morbidity and mortality. They often appear and progress long after exposure to the dusts.
Except for trouble breathing, patients with the inorganic pneumoconioses usually have few or no physical signs.
Respiratory failure and/or cor pulmonale (right-sided heart failure from pulmonary hypertension) eventually kill the patients.
Most inorganic dust exposures are much less dangerous.
Traditionally included among the inorganic pneumoconioses are harmless accumulations of inert dusts -- iron oxide, barium, tin, welding fumes (NEJM 316: 631, 1987), etc.
*Exotic dusts (such as produced in grinding of "hard metal" -- a tungsten alloy used in the tool and die industry) can occasionally cause disease (Eur. J. Resp. Dis. 69: 83, 1986). The chief culprit is probably cobalt (Chest 95: 2 & 29, 1989) with a contribution from nickel (Thorax 45: 267, 1990). αTNF is implicated as culprit in the pathophysiology: Am. Rev. Resp. Dis. 146: 1600, 1992.
A variety of "dust diseases" -- including simple coal-worker's pneumoconiosis -- are caused by dust accumulation plus small amounts of fibrosis around the terminal (* "membranous") and respiratory bronchioles. These compromise respiration far less than do the fibrogenic dusts.
The inorganic pneumoconioses are often "mixed", depending on type of exposure and complications.
*For example, "dental technician's pneumoconiosis" is due to inhalation of a mixture of silica, asbestos, vitallium, and other curious substances.
"Black lung" changes its meaning as the laws change.
Like most diseases, the inorganic pneumoconioses are incurable.
Some of the coal dust may be lavaged from the lungs.
Organic pneumoconioses:
Allergic diseases caused by spores, fibers, etc. They are more important than their omission from Baby Robbins would indicate.
Type I (IgE-mediated, asthma) and/or Type III (immune complexes, vasculitis) & IV (cell-mediated, granulomatous) reactions are the mechanisms of tissue injury. This is bad.
Usually patients recover, usually with little or no fibrosis, but repeated exposure causes the disease to recur. Treatment is directed against the hypersensitivity reaction.
|
{27639} bowling ball manufacture; rumors of dust disease
|

|
COAL WORKER'S PNEUMOCONIOSIS (CSP, "black lung"): Path standards: Arch. Path. Lab. Med. 103(8), 375-432, 1979 (still the best)
{27458} coal miner
{27514} coal workers
A complex pneumoconiosis:
Lesions attributed to coal dust itself ("simple CWP", i.e., the coal macule)
Lesions of silicosis (anthracite coal contains more silica, but bituminous coal workers get silicosis too)
Lesions possibly due to air pollution (miner's wives also suffer severe respiratory symptoms)
Lesions of cigaret smoking (Most disabling "black lung" really results from cigaret smoking!)
Lesions of co-existing tuberculosis
Lesions typical of autoimmune lung disease ("Caplan's syndrome" when the patient has an inorganic pneumoconiosis)
Lesions not easily accounted for by any of the above -- notably progressive massive fibrosis ("genuine black lung").
Simple CWP: the coal macule (macule means "spot")
Focal accumulations of coal dust in the lung. Coal macules are considered practically harmless.
Patients with simple CWP rarely have serious respiratory problems unless there is additional pathology (silicosis, TB, Caplan's, progressive massive fibrosis, cigaret damage).
Coal macules do not grow after coal dust exposure ceases, though patients will cough up black dust for years afterwards. This will impress the miner (and the politicians), who may believe this indicates serious disease.
*Symptomatic graphite pneumoconiosis is now believed to be due to silica in graphite.
Gross pathology:
You can feel the coal macules as 1 mm, hard black bumps. These are located at the centers of pulmonary lobules (i.e., around respiratory bronchioles).
Microscopic pathology:
Aggregates of carbon-laden macrophages within a reticulin network. There is no dense fibrosis. There is mild focal stretching of air-spaces ("emphysema") around the bronchiole, but (in non-smokers!) this is not believed to impair respiratory function.
{08762} anthracosilicosis
In our polluted times, carbon pigment is present in the lungs of every adult. This is ordinarily called
anthracosis.
Progressive massive fibrosis
PMF is variously defined to be many large nodules and/or one or more circumscribed areas of dense
black scar-like tissue, usually in an upper lobe.
It is uncommon, affecting less than 1% of those exposed to coal dust
"Fibrosis" is a misnomer, as there is not nearly so much
collagen in these lesions as you'd find in a scar or a silicotic nodule
Collagen: 20-30%
*Calcium phosphate: 1-30%
*Glycosaminoglycans: 10-20%
*IgA and IgG: several % (but no IgM)
Coal: up to 20%
*All the rest is "amorphous protein" including fibronectin
The etiology of PMF is still obscure, but is probably immune-mediated and
caused by the carbon
itself.
*Thinking about etiology
focuses on rupture of carbon-filled hilar lymph nodes, with discharge of their
contents into the air spaces. This makes the most sense.
*A PMF-like lesion can be induced in immunologically altered animals by giving coal dust, and
PMF occurs in graphite and carbon electrode workers.
PMF is progressive and lethal. Death usually occurs within a few years. There is no treatment.
{49094} progressive massive fibrosis
Caplan's syndrome: rheumatoid arthritis or systemic lupus
or scleroderma or polymyositis-dermatomyositis with an inorganic pneumoconiosis.
(* The eponym has no precise meaning and seems to be passing out of use.)
Sometimes big rheumatoid nodules fill the lungs in these workers. In CWP with Caplan's, they are
inky black, and they may be part of a continuum with PMF.
Coal dust and cancer: coal dust exposure places a worker at increased risk for stomach cancer, but
not for any other common cancer.
Future pathologists: Crack cocaine smoking can impart considerable black
pigment to the lungs.
SILICOSIS: Common and deadly; until recently the most serious occupational disease. All about
silicosis: Arch. Path. Lab. Med. 112: 673, 1988 (great pictures); historians see Science 256: 116,
1992.
The silicosis industries:
Sandblasting
{27461} sandblaster
{27462} sand mold lining
Mt. St. Helen's volcano survivors are not developing chronic silicosis (Am. Rev. Resp. Dis. 133:
526, 1986), but silicosis is common in areas of the world where sand-storms occur (Thorax 46: 334
& 341, 1991).
Tetrahedral crystals of silicon dioxide make up much of the earth's crust.
The tetrahedral configuration is essential to fibrogenicity; octahedral and other forms of silica, as
well as other non-silica crystals with sharp edges (powdered diamonds, etc.) do not cause
collagenization.
*Mixed rock dust disease ("silicatosis"; the term didn't catch on) is essentially silicosis.
Ideas about how silica causes fibrosis no longer emphasize death of macrophages. However they do
their damage, tetrahedral silica crystals have potent effects in biologic membranes.
The hydroxyl groups on the surfaces of the crystals are arranged to interact efficiently with the -NH3
and -PO4 groups in lipids. (This is called "contact catalysis".)
Free radical formation with peroxidation of membrane lipids is probably also involved.
Interestingly, fresh-cut silica powder bears free radicals on its surface for several hours, and it is
much more fibrogenic in the short-term than old-cut silica powder.
*Further, silica crystals directly activate C5a which attracts phagocytes.
The silica crystals seem mostly to affect macrophages. The steps leading to fibrosis are being
worked out.
In the classic model of silica fibrogenesis, a macrophage (sometimes a neutrophil) ingests an inhaled
silica particle, which is taken into phagolysosomes. The crystal disrupts the phagolysosome
membrane, releasing the hydrolytic enzymes and killing the phagocyte. (The silica particle is then
ready for phagocytosis by another phagocyte....) The breakdown products of macrophages are
chemotactic for other phagocytes and finally promote collagen formation. This works in vitro, but is
probably only a minor mechanism in vivo -- silica-laden macrophages washed from the lungs of
workers usually seem quite healthy.
Current thinking focuses instead on inappropriate production of interleukin 1 and other factors by
macrophages following contact with silica.
* A new twist is the discovery that a particular allele for α-TNF
predisposes to much more severe silicosis (Am. J. Resp. Crit. Care Med. 165:
690, 2002).
Gross pathology of silicosis:
Pleural adhesions, silicotic nodules, eggshell calcifications (why?)
in lung and lymph nodes, and silicotic
nodules around the respiratory bronchioles ranging in diameter from 0.1 to 5 mm. (Several nodules
may become confluent, and nodules may occur outside the lungs as crystals travel via lymphatics.
See Hum. Path. 16: 393, 1985. Massively packed, expanding lymph nodes in the
mediastinum can occlude the pulmonary artery (Br. J. Rad. 74: 859, 2001).
The silicotic nodule consists of:
{12437} silicotic nodules
Variations:
Silicotuberculosis: Silicosis with TB, a very common combination (because of poor macrophage
function? poverty? probably both....)
Caplan's syndrome: silicosis with autoimmune disease. (As in CWP, usually the autoimmune
disease is rheumatoid arthritis or systemic lupus.
The active surface of the silica crystals possibly alter the patient's proteins to make them antigenic.
Interleukins could be another problem.
Anthracosilicosis: silicosis with coal worker's pneumoconiosis
Siderosilicosis: silicosis with iron oxide dust
Acute silicosis ("alveolar silicoproteinosis"):
After a massive dose of silica particles, all the alveoli fill with proteinaceous fluid, surfactant, and
necrotic mononuclear phagocytes. The patient dies in a few days to a few months.
The dose of silica overloads the periarteriolar lymphatics that go directly to the hilum. The silica is
transported instead to the alveoli, where it is phagocytized by, and destroys, the Type II
pneumocytes.
Patients are usually sandblasters and rock drillers who fail to wear protective masks. Acute silicosis
led to the World War II graffiti: "Join the Navy and see the world, become a sandblaster and see the
next."
No joke; acute silicosis still exists. See Lancet 337: 344, 1991; Am. Rev. Resp. Dis. 143: 880,
1991 ("Ajax cleanser snorter").
Glucocorticoids for silicosis sufferers: Am. Rev. Resp. Dis. 143: 814, 1991.
* Tetrandrine, a Chinese herb which kills alveolar macrophages, is
a possible help
against silicosis (Biochem. Pharm. 53: 773, 1997). Watch this one.
ASBESTOSIS:
Am. Rev. Resp. Dis.
143: 408, 1991; Rad. Clin. N.A. 30: 1245, 1992; South. Med. J. 85: 616, 1992.
The mineral Sci. Am. 272(1): July 1997.
Asbestos is a family of fibrous minerals, hydrated silicates of sodium, iron, calcium, magnesium. It
is very dangerous stuff, and asbestos-related disease has been under-diagnosed. All types of asbestos
are dangerous, * though chrysotile (serpentine, curved fibers) seldom reach the pleura.
Asbestosis follows heavy or prolonged exposure to airborne asbestos fibers, and progresses even if
dust exposure ceases.
One million people in the US have industrial exposure (workers, neighbors). There are probably
70,000 cases of asbestosis here today. Spray-on asbestos was the worst. (See Postgrad. Med. 74:
93, Oct. 1983.)
Some of the heaviest exposure of the most people was in shipyards before 1970.
(* Great historical article in CA 28: 87, 1978.)
*Asbestos is also used in insulation, fire-proofing, cement, water mains, brake linings, oven cloths,
linoleum, ironing boards, gloves, fireman's suits, linings for chemical pans, theater curtains,
acid-resistant filtering cloths, etc. etc.
In Greece and nearby, asbestos is used for whitewash ("Metsovo Lung", Chest 99: 1158, 1991).
"Practical guide to asbestos abatement": Occup. Health. Saf. 55: 45, Jan., 1986. Selective
indignation and asbestos policy: Science 247: 294, 1990.
A review of the asbstos "cancer epidemic", which we may reasonably think
will cost 10 million lives worldwide: Env. Health Perspect. 112: 285, 2004.
The Environmental Protection Agency (August 1990) reversed itself on the business of
asbestos removal from schools and other public buildings, and now recommends removal only when
buildings are to be demolished. This sensible action recognizes that undisturbed asbestos is no
health threat, and that asbestos removal, (which re-introduces the material into the air) is dangerous.
Perhaps the politicians also realized that asbestos removal would have cost the nation around
$150,000,000,000; the whole episode is now discussed as a classic example of education finally
overcoming hype and hysteria (JAMA 266: 696, 1991). In 2001, the EPA
told everybody not to worry about the tons of asbestos that went swirling
through Manhattan from the World Trade Center collapse. Sensible -- but what
a reversal from the old "one fiber is too many" ideology.
Asbestos fibers that remain in the lung are long (several microns) and slender (around 0.5 microns).
The size and shape of the straight asbestos fiber appear to cause it to be carried preferentially to the
pleural surfaces. Think about a needle, sharper at one end, moving through lung.
Gross pathology:
Marked pulmonary interstitial fibrosis (i.e., actual fibrosis of alveoli and collagenous thickening of
the alveolar-capillary membrane.
Unlike silicosis, the fibrosis is diffuse rather than nodular, involving
mostly the alveolar
septa.
Pleural and subpleural fibrosis develop before there is much pulmonary fibrosis. Large, dense
fibrous plaques form on both parietal and visceral pleura. They may calcify and are occasionally
visible on chest x-ray.
These may be
accompanied by chronic bleeding into the pleural spaces. Asbestos pleural disease: Chest 99: 191,
1991).
Microscopic pathology:
Marked peribronchiolar and (later) alveolar interstitial fibrosis and many asbestos bodies. Often
whole alveoli are obliterated. * We now know granulomas form early in involved areas, but have
undergone fibrosis by the time the patient comes to autopsy (Exp. Mol. Path. 44: 207, 1986).
Asbestos bodies ("ferruginous bodies") are characteristic. They are 10-200 microns long, 1-6
microns wide; golden-yellow beaded rods formed when asbestos (or talc, or other) fibers are coated
by protein in the body. They are most plentiful beneath the pleural surfaces.
{27472} asbestos on the pipes
Only a few of the fibers get coated, and in symptomatic asbestosis, a gram of dry lung tissue may
contain more than a million asbestos fibers. Today's standard seems to be 1000 perticles per gram of dry lung
as an indicator ofoccupational disease (Am. J. Clin. Path. 117: 90, 2002).
Chrysotile -- white asbestos, the commonest form -- is seldom coated, is less likely to reach the
pleura, and dissolves more readily than the other forms. Nevertheless, it's dangerous and is clearly
linked to mesothelioma (Cancer 67: 1912, 1991).
The finding of an asbestos body in sputum or pulmonary lavage fluid is not diagnostic of clinical
asbestosis. Most city-dwellers have a few in their lungs and solid particles of all sorts tend to be
released during episodes of pulmonary edema. However, the more you have in your lavage fluid,
the more likely you are to have serious asbestosis (big study Chest 126: 966, 2004).
*Standards for pulmonary pathology of asbestosis: Arch. Path. Lab. Med. 106: 544, 1982
(still good).
The mechanism of fibrogenesis in asbestosis is probably similar to that in silicosis.
Magnesium atoms spaced along the surface of a fiber react electrostatically with sialic acid residues
on surface glycoproteins of cells, immobilizing them. (See Lab Invest. 49: 468, 1984; Chest
89(S3): 156 S.) Asbestos fibers also activate complement, attracting phagocytes.
As in silicosis and PMF, there is much discussion of altered immunity, but little is known (Chest 91:
110, 1987). * Like silica, asbestos is a potent activator of C5a.
Even in the absence of pulmonary fibrosis, asbestos-exposed people are at special risk for several
forms of cancer.
*Asbestos fibers tangle chromosomes -- Am. J. Path. 126: 343, 1987.
Asbestos is the principal risk factor for mesothelioma
("Steve McQueen's cancer" -- he worked on his own motorcycle, including
the asbestos-lined brakes, and inhaled huge quantities of asbestos while
working in a military brig).
The mechanism is unknown (but see Am. J. Path. 128: 410, 1987). Concurrent cigaret smoking
does not increase the risk.
Most mesotheliomas involve the pleura or, less often, the peritoneum.
One of the most infamous trick questions in medical-school pathology is, "Asbestosis most
often causes which cancer?" The answer is "common bronchogenic carcinoma"
rather than "mesothelioma".
A high mortality rate (20%, up to 50% for smokers) due to the common types of lung cancer has
been reported in U.S. asbestos workers, even those with fairly low exposure and without clinical
asbestosis. For common lung cancers ("bronchogenic carcinoma"), cigaret smoke and asbestos are
obviously synergistic,
perhaps because tobacco carcinogens adsorb onto
the asbestos fibers.
Asbestos exposure also clearly increases the risks of laryngeal and GI cancer, and perhaps malignant
lymphomas.
Other carcinogenic dusts:
Chromium: cancer of the nasopharynx and/or lung
Nickel: cancer of the lung
* Your lecturer does not believe that silica is a carcinogen,
but it is currently classified as such by some government agencies. Stay tuned.
{27494} asbestos and lung cancer
However, the majority of asbestos workers seeking compensation have breathing problems still due
primarily to heart disease or cigaret smoking (Am. Rev. Resp. Dis. 135: 812, 1987).
*Tobacco smoking greatly increases the amount of peribronchiolar fibrosis -- which is surprising.
See JAMA 259: 370, 1988.
The asbestos companies knew the dangers long, long ago: JAMA 265:
898, 1991.
You may enjoy visiting the informational site of mesothelioma lawyers mesothelioma
here or here
or here
or here
or here
or here
(not endorsements, but an instructive read for young doctors -- Ed).
* It takes almost no time or effort to make up and publish a shameless
lie. If the lie is ugly or stupid enough, some people will choose to believe
and act on it, simply to feel "moral" / "spiritual".
And refuting the lies of others is a hard, thankless task.
In 1999, an e-mail campaign
warned about big commercial tampon
manufacturers putting asbestos in cotton tampons to make women
bleed heavier and longer. Of course this was simply made up.
I traced it as
far as I could, and found a culture warrior (left-wing)
who linked her endorsement
and promotion of the
claim with her mail-order "natural" tampon company. She also
mentioned that she founded this company
"to get herself off welfare". I am not making this up. Although
I do not understand why tampon cotton needs to be bleached, the
business about the bleaching process generating agent orange
and causing toxic shock syndrome wasn't true, either. And the persons
cited as the authors of the e-mail vociferously denied having written
it.
BERYLLIOSIS (Chest 109(3S): 40-S, 1996)
Due to inhaled beryllium, which activates macrophages and T-helper cells (NEJM 320: 1103,
1989). Thanks to public health measures, there are fewer opportunities to get berylliosis today --
but the Rocky Flats epidemic of the 1980's
and the Toledo epidemic of the 1990's
should reminded us that powdered beryllium is still
dangerous.
In the past, the greatest peril was in the rocket and fluorescent bulb industries.
The typical lesion of chronic berylliosis is granulomas and interstitial fibrosis of the
lung. You may or may not see necrosis. Sensitization takes a while
but tends to progress (Am. J. Resp. CCM. 171: 54, 2005); thankfully
the vast majority of those exposed never get sick (J. Clin. Inv. 110:
1473, 2002; the key is the immunology).
Cutaneous berylliosis also showed the non-necrotizing granulomas. These patients had scratched
themselves on old fluorescent light bulbs.
The lesions are practically identical to those of sarcoidosis. If you need to distinguish the two
diseases using the lab, we can check for berylliosis.
*Only a minority of exposed people are vulnerable to this disease (i.e., most people are
non-reactive to beryllium). Those who can get it had glutamate in position 69 of the HLA-DPβ1
chain (Science 262: 197, 1993; now a robust finding though somewhat modified J. Imm. 163: 1647, 1999).
* The Rocky Flats fiasco: Allied Occup. Env. Hy. 16: 405, 2001;
Env. Health Perspect. 104 (S5): 981, 1996.
Some folks got sick, notably about 10% of the beryllium machinists,
but it was not a massive disaster as it has been portrayed.
Probably the neighbors were not endangered
(Env. Health Perspect. 107: 731, 1999).
{27503} berylliosis
*There was also an acute, "irritant" pneumoconiosis.
*Zirconium dust produces the same picture; "deodorant granulomas" were from zirconium.
FARMER'S LUNG (and variants)
Victims are sensitive to spores from moldy hay, etc. (Micropolysporum, Thermoactinomyces -- these
"molds" include allergenic bacteria). Both farmers and their animals are susceptible.
{27489} farmers in moldy hay
Non-farmers can get a similar disease from mold in air-conditioners ("humidifier fever", etc.),
cardboard, etc. (See JAMA 258: 1210, 1987).
Clinical course: Either or both of two phases
First phase: transient IgE-mediated syndrome with bronchoconstriction (wheezing, etc.)
Second phase: IgG-mediated type III-injury vasculitis ("extrinsic allergic alveolitis";
"hypersensitivity alveolitis") which may be serious. It can be acute, subacute, or chronic. In really
bad cases, there may be granuloma formation, tissue necrosis, fibrosis (Am. Rev. Resp. Dis. 133:
88, 1986), etc.
Precipitating IgG antibodies against the offending mold can be demonstrated in the patient's serum
(and in the serum of many asymptomatic farmers, too; Thorax 44: 469, 1989). For a review of the
diagnostic immunology of the organic pneumoconioses, see Clin. Lab. Med. 4: 523, 1984.
Bagassosis: farmer's lung caused by molds in dry sugar cane.
*Other forms of "extrinsic allergic alveolitis":
"Animal house lung": fraternity party with straw (JAMA 258: 1219, 1987)
*Interestingly, these patients are reported to have semi-anergy: Thorax 44: 132, 1989.
You can benefit many of these people by installing electrostatic dust filters (Ann. Int. Med. 110:
115, 1989). A face mask for hay-time: Chest 95: 100, 1989.
BYSSINOSIS (cotton, flax, hemp processing)
Nobody questions that fibers from vegetable textiles are noxious and irritating.
Traditional pathology texts describe "monday morning asthma".
This is the only organic pneumoconiosis in which there is prolonged
wheezing.
Here's the familiar story. On Monday morning, lots of guys at the cotton mill report not feeling well.
By Monday afternoon, and for the rest of the week all the mediators are depleted and the symptoms
disappear. Over the weekend the mediators are replenished in time for next Monday's attack.
If you believe this "disease mechanism", you'll believe anything. For starters, most allergic
wheezing is due to leukotrienes, which aren't even stored. Decide for yourself what's really
happening. Reports of a substance in cotton that releases histamine
from mast cells remain unconfirmed.
"Brown lung" is claimed by some textile workers to be a major cause of chronic respiratory
disability.
Much of the problem, of course, is due to cigaret smoking.
Only recently has chronic obstructive lung disease in non-smoking cotton workers been clearly
caused by cotton dust exposure. As usual, there are "confounding variables."
 Hut lung
Hut lung
From indoor air pollution
Dr. Warnock's Collection
 Silicosis
Silicosis
Lung pathology series
Dr. Warnock's Collection
{35063} progressive massive fibrosis
The OSHA "acceptable" levels might still be a bit high, since even today,
the more exposure a worker has
has, the more obstruction shows on spirometry. However, it's far worse
to be a smoker.
See Chest 122: 721, 2002.
Mining and tunneling (silicosis is still a major problem in third-world mines: Chest 113: 340, 1998;
Am. J. Resp. Crit. Care Med. 153: 706, 1996)
Foundries
Gun-flint industry
Sandstone industry
Granite industry
Pottery industry
Metal grinding
Manufacture of abrasive soaps
*Kaolin (china clay, mild because kaolin is really feldspar -- Thorax 41: 190, 1986; Am. Rev. Resp.
Dis. 138: 813, 1988; silicosis in a U.S. toilet factory: MMWR 41: 405, 1992)
{34985} sandblaster
{28760} silicosis
{28763} silicosis
{28766} silicosis
{28769} silicosis
{35000} silicosis
{49096} silicosis
{35057} anthracosilicosis
 Silicosis and silicatosis
Silicosis and silicatosis
Lung pathology series; follow the arrows
Dr. Warnock's Collection
Silicotic nodule
WebPath Photo
Silicotic nodule
WebPath Photo
As a clinician, you may decide to treat everybody who has
a history of silica exposure and a positive PPD as if he/she was
actually sick with TB. Ask your infectious disease consultant.
Alveolar proteinosis from silicosis
Lung pathology series
Dr. Warnock's Collection
(* By the way, have you ever heard a
politician getting all excited about lead-based paint chips in old houses inhabited mostly by
poor people who don't care about "environmentalism"? This is a real health menace,
but one with no activism.
{36190} ferruginous body
{39685} ferruginous body
{09834} ferruginous body, special preparation (darkfield?)
Ferruginous body
Inside an epithelioid giant cell
Urbana Atlas of Pathology
Asbestosis
Photo and mini-review
Brown U.
Asbestosis
Lung pathology series
Dr. Warnock's Collection
 Mesothelioma Information Group
Mesothelioma Information Group
Resources and advocacy
Also asbestosis and bronchogenic CA
Beryllium lung and sarcoid
Lung pathology series
Dr. Warnock's Collection
Hypersensitivity pneumonitis
Lung pathology series
Dr. Warnock's Collection
Woodworker's pneumoconiosis (including "sequoiosis" from redwood mold)
Mushroom worker's lung (Chest 122: 1080, 2002)
Cheese worker's disease
Grain handler's pneumoconiosis (Can. Med. Assoc. J. 133: 969, 1985)
Malt worker's pneumoconiosis
Pigeon keeper's lung ("bird-fancier's lung")
Pituitary snuff taker's lung (diabetes insipidus victims)
Portuguese cork-worker's lung (suberosis)
Sisal-worker's disease
 Hungarian paprika-splitter's disease
Hungarian paprika-splitter's disease
Tea-maker's asthma
Coffee bean dust disease
Furrier's lung
Sudanese bat-guano asthma (Lancet 1: 316, 1987)
Leather waterproofer's lung (Br. Med. J. 292: 727, 1986)
Zimbabwe ivory-carver's lung (Thorax 43: 342, 1988); save the elephants
Silkworm dropping lung (Thorax 45: 233, 1990)


| Visitors to www.pathguy.com reset Jan. 30, 2005: |
Ed says, "This world would be a sorry place if
people like me who call ourselves Christians
didn't try to act as good as
other
good people
."
Prayer Request
 Teaching Pathology
Teaching Pathology
PathMax -- Shawn E. Cowper MD's
pathology education links
Ed's Autopsy Page
Notes for Good Lecturers
Small Group Teaching
Socratic
Teaching
Preventing "F"'s
Classroom Control
"I Hate Histology!"
Ed's Physiology Challenge
Pathology Identification
Keys ("Kansas City Field Guide to Pathology")
Ed's Basic Science
Trivia Quiz -- have a chuckle!
Rudolf
Virchow on Pathology Education -- humor
Curriculum Position Paper -- humor
The Pathology Blues
 Ed's Pathology Review for USMLE I
Ed's Pathology Review for USMLE I
![]()
![]()
 | Pathological Chess |
 |
Taser Video 83.4 MB 7:26 min |

 Environmental Pathology
Environmental Pathology
 Occupational Lung Disease
Occupational Lung Disease Asbestos
Asbestos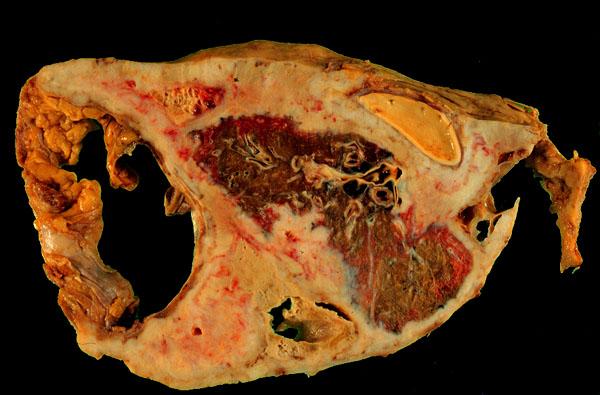 Mesothelioma
Mesothelioma