Ed Friedlander, M.D., Pathologist
scalpel_blade@yahoo.com



Cyberfriends: The help you're looking for is probably here.
Welcome to Ed's Pathology Notes, placed here originally for the convenience of medical students at my school. You need to check the accuracy of any information, from any source, against other credible sources. I cannot diagnose or treat over the web, I cannot comment on the health care you have already received, and these notes cannot substitute for your own doctor's care. I am good at helping people find resources and answers. If you need me, send me an E-mail at scalpel_blade@yahoo.com Your confidentiality is completely respected.
 DoctorGeorge.com is a larger, full-time service.
There is also a fee site at myphysicians.com,
and another at www.afraidtoask.com.
DoctorGeorge.com is a larger, full-time service.
There is also a fee site at myphysicians.com,
and another at www.afraidtoask.com.
Translate this page automatically
 |
With one of four large boxes of "Pathguy" replies. |
 I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
Numbers in {curly braces} are from the magnificent Slice of Life videodisk. No medical student should be without access to this wonderful resource. Someday you may be able to access these pictures directly from this page.
Also:
Medmark Pathology -- massive listing of pathology sites
Freely have you received, freely give. -- Matthew 10:8. My
site receives an enormous amount of traffic, and I'm
handling about 200 requests for information weekly, all
as a public service.
Pathology's modern founder,
Rudolf
Virchow M.D., left a legacy
of realism and social conscience for the discipline. I am
a mainstream Christian, a man of science, and a proponent of
common sense and common kindness. I am an outspoken enemy
of all the make-believe and bunk that interfere with
peoples' health, reasonable freedom, and happiness. I
talk and write straight, and without apology.
Throughout these notes, I am speaking only
for myself, and not for any employer, organization,
or associate.
Special thanks to my friend and colleague,
Charles Wheeler M.D.,
pathologist and former Kansas City mayor. Thanks also
to the real Patch
Adams M.D., who wrote me encouragement when we were both
beginning our unusual medical careers.
If you're a private individual who's
enjoyed this site, and want to say, "Thank you, Ed!", then
what I'd like best is a contribution to the Episcopalian home for
abandoned, neglected, and abused kids in Nevada:
My home page
Especially if you're looking for
information on a disease with a name
that you know, here are a couple of
great places for you to go right now
and use Medline, which will
allow you to find every relevant
current scientific publication.
You owe it to yourself to learn to
use this invaluable internet resource.
Not only will you find some information
immediately, but you'll have references
to journal articles that you can obtain
by interlibrary loan, plus the names of
the world's foremost experts and their
institutions.
Alternative (complementary) medicine has made real progress since my
generally-unfavorable 1983 review linked below. If you are
interested in complementary medicine, then I would urge you
to visit my new
Alternative Medicine page.
If you are looking for something on complementary
medicine, please go first to
the American
Association of Naturopathic Physicians.
And for your enjoyment... here are some of my old pathology
exams
for medical school undergraduates.
I cannot examine every claim that my correspondents
share with me. Sometimes the independent thinkers
prove to be correct, and paradigms shift as a result.
You also know that extraordinary claims require
extraordinary evidence. When a discovery proves to
square with the observable world, scientists make
reputations by confirming it, and corporations
are soon making profits from it. When a
decades-old claim by a "persecuted genius"
finds no acceptance from mainstream science,
it probably failed some basic experimental tests designed
to eliminate self-deception. If you ask me about
something like this, I will simply invite you to
do some tests yourself, perhaps as a high-school
science project. Who knows? Perhaps
it'll be you who makes the next great discovery!
Our world is full of people who have found peace, fulfillment, and friendship
by suspending their own reasoning and
simply accepting a single authority that seems wise and good.
I've learned that they leave the movements when, and only when, they
discover they have been maliciously deceived.
In the meantime, nothing that I can say or do will
convince such people that I am a decent human being. I no longer
answer my crank mail.
This site is my hobby, and I presently have no sponsor.
This page was last updated February 6, 2006.
During the ten years my site has been online, it's proved to be
one of the most popular of all internet sites for undergraduate
physician and allied-health education. It is so well-known
that I'm not worried about borrowers.
I never refuse requests from colleagues for permission to
adapt or duplicate it for their own courses... and many do.
So, fellow-teachers,
help yourselves. Don't sell it for a profit, don't use it for a bad purpose,
and at some time in your course, mention me as author and KCUMB as my institution. Drop me a note about
your successes. And special
thanks to everyone who's helped and encouraged me, and especially the
people at KCUMB
for making it possible, and my teaching assistants over the years.
Whatever you're looking for on the web, I hope you find it,
here or elsewhere. Health and friendship!
 I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
Pathology Education Instructional Resource -- U. of Alabama; includes a digital library
Houston Pathology -- loads of great pictures for student doctors
Pathopic -- Swiss site; great resource for the truly hard-core
Syracuse -- pathology cases
Walter Reed -- surgical cases
Alabama's Interactive Pathology Lab
"Companion to Big Robbins" -- very little here yet
Alberta
Pathology Images --hard-core!
Cornell
Image Collection -- great site
Bristol Biomedical
Image Archive
EMBBS Clinical
Photo Library
Chilean Image Bank -- General Pathology -- en Español
Chilean Image Bank -- Systemic Pathology -- en Español
Connecticut
Virtual Pathology Museum
Australian
Interactive Pathology Museum
Semmelweis U.,
Budapest -- enormous pathology photo collection
Iowa Skin
Pathology
Loyola
Dermatology
History of Medicine -- National Library of Medicine
KU
Pathology Home
Page -- friends of mine
The Medical Algorithms Project -- not so much pathology, but worth a visit
National Museum of Health & Medicine -- Armed Forces Institute of Pathology
Telmeds -- brilliant site by the medical students of Panama (Spanish language)
U of
Iowa Dermatology Images
U Wash
Cytogenetics Image Gallery
Urbana
Atlas of Pathology -- great site
Visible
Human Project at NLM
WebPath:
Internet Pathology
Laboratory -- great site My team:
My team:Ed Lulo's Pathology Gallery
Bryan Lee's Pathology Museum
Dino Laporte: Pathology Museum
Tom Demark: Pathology Museum
Dan Hammoudi's Site
Claude Roofian's Site
Pathology Handout -- Korean student-generated site; I am pleased to permit their use of my cartoons
Estimating the Time of Death -- computer program right on a webpage
Pathology Field Guide -- recognizing anatomic lesions, no pictures

St.
Jude's Ranch for Children
I've spent time there and they are good. Write "Thanks
Ed" on your check.
PO Box 60100
Boulder City, NV 89006--0100
More of my notes
My medical students
Clinical
Queries -- PubMed from the National Institutes of Health.
Take your questions here first.
HealthWorld
Yahoo! Medline lists other sites that may work well for you

We comply with the
HONcode standard for health trust worthy
information:
verify
here. 

![]()
Describe the principal cells of the immune system, where they are found, and what we think they do. Identify CD4, CD8, CD6. Explain the CD4+/CD8+ ratio, especially as it applies to the historic test for AIDS. Identify interleukin 1, interleukin 2, tumor necrosis factor, lymphotoxin, and interferons.
Identify the five classes of antibodies, and tell what we know they do. List some helpful, some useless, and some harmful antibodies that our immune systems can make. Tell what complement is and what we know it does. Tell what a hapten is.
For each of the following, describe the essential mechanism and mention some real-life illustrations: Type I, Type II, Type III, and Type IV hypersensitivity injury.
Briefly describe each of the following:
urticaria
systemic anaphylaxis
food allergy
Type II (fixed antigens)
Complement-mediated
ABO-mismatched transfusion reaction
Rh-mismatched delayed transfusion reaction
Autoimmune hemolytic anemia
Autoimmune thrombocytopenia
Goodpasture's disease of the lung and kidney
Pemphigus family of skin diseases
Cell-mediated ("antibody-dependent cell-mediated cytotoxicity")
Antibody-mediated dysfunction ("Type V immune injury")
circulating anticoagulants
classic pernicious anemia
excitatory and inhibitory antibodies (Graves', many others)
Type III (immune complex disease; soluble antigens)
Arthus reaction -- serum sickness
aches and pains of the "'flu"
Immune-complex induced thrombocytopenia (AIDS, idiopathic)
polyarteritis nodosa secondary to hepatitis B infection
Type IV (delayed hypersensitivity, + non-antibody-mediated)
tuberculin skin test
nickel skin allergy
multiple sclerosis
juvenile-onset diabetes mellitus
"anergy"
Recognize each of the following using the microscope:
eosinophils, plasma cells, basophils, lymphocytes
vasculitis (with and without fibrinoid)
granulomas and their epithelioid cells
Critique the following statement, overheard at a party: "By strengthening our immune system, we prevent or cure most diseases. We strengthen our immune system by nutritional supplements and mental imagery to reduce stress."
QUIZBANK
Immunopathology (all; this covers these 4 lectures)
Metabolic (amyloid) #'s 93-111
Clinical immunology lab (all)
LEARN FIRST: TYPES OF IMMUNE INJURY ("HYPERSENSITIVITY")
Okay. These divisions are artificial.
Type I... Havoc resulting from IgE and mast-cell degranulation
Type II... Antibodies bind to cells. This can cause
Type III... Antigen-antibody complexes ("immune complexes") precipitate and cause the damage
Type IV... Havoc wrought by specifically-sensitized T-cells without involvement of antibodies. This includes...
"Classic delayed hypersensitivity", in which the harm is done primarily by recruited macrophages and innocent bystander cells are also massacred. No antibody is involved.
"Antibody-independent cell-mediated cytotoxicity", in which individual cells are assassinated ("apoptosis") by T-CTL lymphocytes, without harm to innocent bystanders.
CELLS OF THE IMMUNE SYSTEM
|
{14252} lymphocytes
| 
|
Overview of the immune system: Origins, molecular biology, basic components, with nice pictures and articles Sci. Am. Sept. 1993. Evolution of the vertebrate system: Proc. Nat. Acad. Sci. 91: 10769, 1994. Immunity in drosophila is quite different, and is just now being unravelled.
T-lymphocytes (T-cells):
A versatile family of cells that have passed through the thymus (and been acted on by the hormone thymosin) during early biological life.
T-cells are the center-piece of the immune system. T-cells of various sorts are predominant throughout the lymph nodes except in and around germinal centers. They also make up most of the white pulp of the spleen, and occupy the thymus gland. Around 80% of circulating lymphocytes are T-cells.
Young T-cells differentiate into many subtypes, which act as regulators and effectors.
Each T-cell acquires its specificity, which it transmits to its descendants, by recombination of its TCR gene before birth.
CD3 -- joins with the TCR surface molecule, but is not rearranged
CD4 -- marker for cells such as helpers, which recognize class II MHC antigens
CD8 -- marker for cells such as killers, which recognize class I MHC antigens.
CD28 -- co-receptor that must be stimulated when the TCR is stimulated,
or else the T-cell becomes anergic or apoptotic
T-helper cells (TH-cells) activate B- and other T-cells
Many subclasses exist to do different things. You'll learn about them in "Immunology".
Worth remembering: TH1's produce IL-2 and INF-gamma and act on macrophages; TH2's produce IL-4 and IL-5 and work on the eosinophils.
T-cytolytic (T-CTL-cells, T-killer cells) cells attach to and kill (apoptosis) cells bearing whatever antigen against which they are specifically programmed and sensitized. These cells may be T4+ or T8+.
After a T-cell has responded to a particular antigen and proliferated, some members of the clone survive and thus the response to the antigen is stronger next time it is encountered ("clonal expansion").
B-lymphocytes (B-cells):
Another class of lymphocytes, which when activated produce freely circulating immunoglobulins ("antibodies", "gamma globulins", "humoral immunity").
Antibodies coat harmful foreign particles, and bind to foreign molecules.
Sometimes this helps (pneumococcal pneumonia, measles, hepatitis B).
Sometimes it doesn't seem to help (AIDS, many other infections, cancer).
Sometimes it hurts (ragweed allergy, autoimmune hemolytic anemia, systemic lupus, pernicious anemia, and every other type I, type II, and type III hypersensitivity disease).
B-cells predominate in the follicles (germinal centers) of the lymph nodes and are more common than T-cells in the red pulp of the spleen and in the bone marrow.
In the germinal centers, antigen-antibody complexes are presented to baby B-cells by the dendritic follicular cells (seen 'em?); the ones that match the antigen best are caused to divide and mature (Nature 367: 425, 1994). These will be the ones that make IgG.
* Misleading statement in Big Robbins -- we often do not see germinal centers in the spleen, especially in older folks.
Around 15% of circulating lymphocytes in the peripheral blood are B-cells.
B-cells have surface immunoglobulin, Fc receptors, C3b receptors, and * CD40 (which we'll meet again).
B-cell activation is partially understood.
Before birth, each B-cell gets its immunoglobulin gene rearranged to recognize a particular antigen. The antibody that the B-cell will make is displayed on its surface, with its business end pointing straight outward.
If and when this antigen comes along, it triggers the B-cell, which starts dividing (under the modulation of T-cells, of course).
After assuming a variety of curious shapes (look at the cells within a germinal center), most of the original B-cell's progeny become a "selected clone" of plasma cells pumping out specific antibody.
{46429} plasma cell, electron micrograph
When the immune system wins, the plasma cells mostly die, but plenty of the original B-cell's clones survive and "remember". Next time the antigen comes along, the antibody response will be much greater ("anamnestic response", i.e., "we haven't forgotten").
Remember: you can't tell resting B-cells from resting T-cells by their morphology. (* Special stains are available that use the OKT system of monoclonal antibodies.)
Natural Killer Lymphocytes:
"Natural killer lymphocytes" (NK-cells) are bigger than other lymphocytes, and have cytoplasmic granules (i.e., you can pick them out on a smear; they make up around 10% of the circulating cells).
They attack and cause apoptosis in cells with altered class I MCH antigens, without being "specially sensitized".
The granules, which are injected into the target cell, contain perforin and granzyme, along with other stuff (* TIA-1 etc.).
Mononuclear phagocytes
This is all of the "reticuloendothelial system", found throughout the body. Probably this is the oldest component of the immune system.
The familiar wandering macrophages and microglia are monocytes from the peripheral blood that have entered the tissues. (Same cell, different names.)
Fixed phagocytes (the rest of the "mononuclear phagocytic system") line the vascular channels of the body. They, too, were once circulating monocytes.
A special subclass of mononuclear phagocytes, the "dendritic" and "Langerhans'" cells (* together, "the accessory cells", etc.), seem to be the best antigen processors and the poorest effector phagocytes. They have special surface antigens (* Ia -- Immune activation antigens coded by HLA genes), express CD6 (OKT1), and have other special features.
Mononuclear phagocytes are essential to immune responses.
The "accessory cells" ("dendritic" and "Langerhans'") apparently phagocytize antigens, process them (into "epitopes"), attach them to Ia antigens, and present them to lymphocytes to begin the immune response.
Busy macrophages modulate the activities of other cells by secreting soluble factors such as interleukin 1 and TNF-alpha (see above), as well as some complement components (supplementing the bulk, which come from the liver).
In addition, macrophages are effector cells when summoned by T-cells or activated complement. They devour and sometimes digest harmful things, and can become epithelioid cells of granulomas to wall off other bad things.
They have receptors for the Fc portion of IgG and for various complement components.
{08230} macrophage containing leishmania (Baghdad boil)
Mast cells and basophils
These cells are rich in vasoactive (and other) substances. In addition to the familiar histamine (right away) and leukotrienes (after a while), remember endothelium relaxing factor and neutrophil chemotactic factor.
When mast cells are activated (usually by something reacting with the IgE that covers their surfaces), the substances are released (histamine right away, leukotrienes over a few hours). These have a variety of effects on blood vessels, smooth muscle, gastric parietal cells, etc.
* In 1989, at a scientific meeting, the author got into it with French biochemist Jacques Benveniste, who claimed to have demonstrated an effect of homeopathic-type dilutions on basophil degranulation. Dr. Benveniste showed a phase contrast photo that the author believed was a neutrophil, and called it a degranulated basophil. Dr. Benveniste graciously acknowledged that making the distinction was difficult. I believe he is sincere, if perhaps wrong. For more on Dr. Benveniste, see Skeptical Inquirer 22(1): 19, Jan-Feb 1998.
{09205} mast cell granules (electron micrograph)
{13733} mast cells
{14539} mast cells (purple ones) and fibroblasts
{14542} mast cell degranulating
{15117} mast cell city!
{46472} mast cell, electron micrograph, intact
{46473} mast cell, electron micrograph, degranulating
Neutrophils: You are already familiar with these important commando cells.
Polys elaborate at least 50 distinct destructive substances. Remember that, while they fight infection, neutrophils also do tremendous damage to the body itself.
In the common (1/2000 people) "chronic granulomatous disease", the neutrophils cannot produce peroxide to kill staphylococci, so the epithelioid macrophages must take over (hence the name of the disease).
Eosinophils: Review in J. Allerg. Clin. Immuno. 105: 651, 2000.
{09207} eosinophil granules
{14099} eosinophils
{14708} eosinophil
IMMUNOGLOBULINS AND COMPLEMENT should be familiar to you.
IgM (our most important macroglobulin) molecules are large pentamers, tend to be cold-reactive, appear early during the humoral immune response, and can fix complement when just one molecule binds to something. IgG molecules are usually monomers, tend to be warm-reactive, appear later during humoral response, include some classes that can fix complement when two or more molecules find to something, and comes from B-cells clones with good memories. IgA molecules tend to be found on mucosal surfaces and in mothers' milk. IgD is a receptor on a B-cell, and its significance in the circulating blood remains obscure. IgE sticks by its Fc portion to basophils and mast cells, ready to tell them to degranulate.
Idiotypes are the specific recognition sequences that make a particular antibody unique. Watch for "anti-idiotype" molecules as an up-and-coming way of modulating the immune system (and evidence that it's one way in which we modulate our own system. Note that an anti-idiotype antibody is likely to resemble the antigen, since both bind to the same location.)
The complement cascade, when activated, increases vascular permeability, summons polys and monos, and punches holes in membranes. All chordates have complement.
CYTOKINES
Immune cells send messages by cytokines (formerly called "lymphokines"), and receive similar messages from other cells. Over a dozen of these "biologic response modifiers" are well-characterized, and several are now undergoing clinical trials. (* There are lymphokine reviews by the dozens. How B-cells and T-cells communicate with each other: Nature 367: 425, 1994, still good; lots more.)
Interleukin 1: a "monokine" produced in bulk by macrophages that are phagocytizing or hurting, this substance causes T-cells to multiply. It also causes the acute-phase reaction (* with interleukin 6 and TNF; you will learn about the acute phase reaction later), acts on the brain to cause fever and fatigue (etc., key paper Science 240: 321, 1988), causes catabolism of muscle in acute illness, recruits macrophages for granuloma formation, and is largely responsible for the increase in circulating neutrophils. IL-1 reviews: Blood 87: 2095, 1996; Blood 88: 2465, 1996.
* Interleukin-1 receptor antagonist (IL-1RA) is yet another molecule in your internal milieu. It is still search of a disease for which it's the magic bullet (Postgrad. Med. 106: 82, 1999).
Interleukin 2 (IL-2, "T-cell growth factor"): a lymphokine from activated T4+ cells that promotes the division of other T-cells.
This -- with or without killer cells -- is a perennial experimental cancer therapy. It causes severe fatigue and insanity.... (horror stories Ann. Int. Med. 107: 293, 1987), and old reports that it was extremely elevated in the controversial "chronic fatigue syndrome" ("Yuppie 'flu", Ann. Int. Med. 110: 321, 1989) have failed to find additional support; this claim (and others about cytokines, in chronic fatigue syndrome and in fibromyalgia) have failed by today's tests (J. Clin. Immuno. 19: 414, 1999; Clin. Exp. Imm. 132: 360, 2003). Whether there is some more subtle disturbance remains unknown -- I still suspect there is.
Its use in treating kidney cancer is still controversial: Science 255: 528, 1992. Possibly the archaic bacterially-derived "Coley's toxins" worked against cancer by making the body produce interleukins (Nature 357: 11, 1992).
* IL-2 receptor levels, from breakdown of T cells, lets you know level of activity of immune disease. They are presently used to follow the therapy of various granulomatous diseases (Chest 99: 268, 1991).
Interleukin 5 is the great mobilizer of eosinophils: NEJM 324: 1110, 1991 (still good). Interleukin 8 is chemotactic for neutrophils. We'll meet both of these throughout the "Pathology" lecture sequence.
Interferons: a class of substances, some produced by T-cells, which "interfere with viruses" and have a huge variety of other activities.
Alpha (alfa) interferon (* many subtypes exist) is currently standard therapy for hairy-cell leukemia, chronic hepatitis B and C, essential thrombocythemia, laryngeal warts, chronic granulocytic leukemia (nobody knows how this works), and "chronic granulomatous disease" (i.e., bad polys). Successes against cancer have been less impressive, though it's helped some melanoma patients. Administration causes a 'flu-like syndrome; it also acts on the brain, causing severe fatigue and/or even insanity.
Beta interferon is the old name for B-cell stimulating factor, which turns B-cells into plasma cells. It is now an important part of the treatment of multiple sclerosis.
Gamma interferon seems to be the principal substance that makes macrophages angry and form granulomas, and the substance that causes macrophages to express Ia antigens. Clinical uses now include leprosy, leishmaniasis, atypical mycobacteria, and stubborn venereal warts. It can be administered by vein (the 'flu-like syndrome it produces is mild), or inhaled for lung disease.
Tumor necrosis factors: a "monokine" ("tumor necrosis factor alpha", "cachectin", now usually called simply "tumor necrosis factor" or "TNF") and a closely-related "lymphokine" (tumor necrosis factor beta", now usually called simply "lymphotoxin"), tandem homologous gene products that mediate a wide range of tissue injuries.
This was a hot topic especially in the 1990's. Everything from endotoxic shock -- "the Schwartzman reaction" -- to the Herxheimer response (NEJM 335: 311, 1996) to Waterhouse-Friderichsen syndrome to extreme over-activation of arachidonate metabolite systems to cachexia of cancer and AIDS is attributed to these substances. Key review NEJM 316: 379, 1987; still good.
* It's been known for over a decade that TNF also participates in granuloma formation, probably acting as an autocrine factor (Cell 56: 731, 1989, Clin. Imm. Imm. 51: 419, 1989). TNF is able to generate granulomas in the absence of any lymphocytes (Nature 356: 604, 1992), contradicting classic assumptions ("All granulomas are held together by gamma interferon"), and explaining why AIDS patients can still make reasonable granulomas.
Thalidomide selectively inhibits alpha-TNF production (Proc. Nat. Acad. Sci. 90: 5974, 1993 was key) and is finding uses in clinical medicine (sarcoidosis, inflammatory bowel disease, ankylosing spondylitis, Behcet's, recalcitrant aphthae in AIDS, even congestive heart failure).
* In the mid-1990's, a group of clinicians tried to help septic shock patients by removing tumor necrosis factor using antibodies. This didn't help, and seems to have killed a bunch of people, probably by a type III immune mechanism: NEJM 334: 1697, 1996.
TNF receptors are a story in themselves, and include the apoptosis equipment (no surprise): NEJM 334: 1717, 1996. One of the great success stories of today's medicine is administration of recombinant TNF receptors to soak up TNF itself in various diseases. * "TRAPS" (TNF-receptor-associated periodic syndrome) is an episodic fever syndrome caused by a mutation in the TNF receptor (Medicine 81: 349, 2002).
Transforming growth factor beta is three isoforms that apparently turn down most aspects of chronic inflammation. Mice born without the first isoform die young of widespread chronic inflammation (Proc. Nat. Acad. Sci. 90: 770, 1993).
The chemokines bring in and (sometimes) activate specific subsets of white cells, etc., etc. Lancet 349, 1997.
Lately we've discovered that simply injecting the DNA for a particular protein into muscle or dermis commonly results in B-cell and T-cell immunity to that protein (Proc. Nat. Acad. Sci. 91: 9519, 1994). This is now a BIG deal, especially for vaccines.
TYPE I IMMUNE INJURY IN HUMAN DISEASE (* ahh--CHOO!)
Type I hypersensitivity ("anaphylactic" or "immediate hypersensitivity") is the result of antigen binding to IgE on the surface of mast cells and basophils. These instantly degranulate and release active substances into the surrounding tissue.
The reaction begins within seconds to minutes following antigen exposure, and is over within a few hours.
IgE protects us against worms. (Almost everyone gets allergic to ascaris worm once they have met it.) The idea that type I hypersensitivity was created to help protect us from worms has found good experimental support: Nature 349: 243, 1991.
* IgE production is of course orchestrated by T-helper and T-suppressor cells that specialize in just this.
* A few unusual types of IgG attached to mast cells can do exactly the same thing that IgE does.
Some people make IgE much more readily than others, and these are the people with allergies ("atopic disease").
"Atopy" means "strange". It's strange that some, but not all, people get asthma from something as trivial as cat dander.
"Allergy freaks" (like the author of these notes) express IgE receptor (Fc[epsilon]RI) on the antigen-presenting cells. Despite "Big Robbins", this does seem to be holding up (J. Clin. Inv. 111: 1047, 2003; J. Imm. 171: 6458, 2004).
Once induced (by one or more encounters with the antigen, or "allergen"), IgE binds to the mast cells and basophils. The person is now allergic to the particular "allergen".
It will get worse every time the allergen is encountered, and if the allergen is carefully avoided, the allergy will become less severe.
The mast cell mediators cause a reaction that would help expel a worm (itching, sneezing, coughing, vomiting, diarrhea). Type I allergic responses to harmless allergens range from annoying to fatal.
Histamine from mast cells makes vessels leaky, causes bronchial smooth muscle to constrict, and causes the gastric parietal cells to churn out acid.
Thus, depending on the location of the degranulating mast cells, the patient gets irritation (itching), tissue edema (soft tissue swelling, sniffling, sneezing, maybe diarrhea, even pulmonary edema), starts wheezing, and gets "sick to the stomach" (histamine mediates acid secretion in the stomach).
Mast cells also release "eosinophil chemotactic factor of anaphylaxis" (which summons the eosinophils characteristic of allergy and worm infestation), and neutrophil chemotactic factor (perhaps to eat the suspected worm).
* And plenty of other stuff of dubious significance is found in mast cell granules.
The acute phase is done in an hour, and the late phase may then begin, with infiltration of the tissues by B and T cells and eosinophils.
Leukotrienes (C4, D4, E4) mediate much of this.
They are arachidonic acid metabolites, the old "slow reacting substances of anaphylaxis". They are not released from mast cell granules, but synthesized for the occasion after the cell has degranulated.
Leukotrienes are responsible for some of the allergic wheezing, etc., that does not respond to antihistamines. Today's avant-garde anti-allergy drugs target leukotrienes and their receptors.
* Prostaglandin D2 and "platelet activating factor" are two other made-to-order mediators.
Future pathologists: You can just barely distinguish mast cells in a standard H&E preparation, but you can see them easily if you use a bit of toluidine blue.
Local anaphylaxis: more often a nuisance than a real danger
Urticaria ("hives"): analogous to the wheal-and-flare effect of histamine in acute inflammation. Red, itchy swellings of the skin that blanch easily on pressure.
{09716} urticaria
{09719} urticaria
{09720} urticaria; this is a variant with pressure-sensitive mast cells ("dermographism")
{12238} urticaria
{12240} urticaria
{25474} urticaria
An itchy mosquito bite is an example of localized urticaria.
In cold urticaria, lowering the temperature causes mast cells to degranulate. The mechanism is obscure. (No one knows exactly what the basis is; these people usually have other IgE-mediated allergies. These patients can die instantly when they jump into cold water.)
* There's a familial syndrome in which the cold produces not urticaria, but a maculopapular rash caused by lymphocyte and macrophage infiltration). The locus is the cryopyrin / Muckle-Wells gene CIAS1 (Am. J. Hum. Genet. 71: 198, 2002). Treating the severe form with interluekin-1 receptor antagonist: NEJM 348: 2583, 2003.
Finding the allergen in chronic urticaria may require an elimination diet. Today's thinking is that food is rarely a cause (Pediatrics 111: 1617, 2003 -- remember it's often a problem in atopic dermatitis). Very often, it's an autoimmune disease caused by antibodies against Fc episilon RI and/or IgE (J. Allerg. Clin. Imm. 110: 492, 2002 and below)
Cholinergic urticaria is the little red blotchies that some folks get in a hot shower or on exercising. They start on the chest and spread, and may be accompanied by parasympathetic stuff. Long a minor mystery of medicine, it's now clear that the real cause is obstruction of the outlet of the sweat ducts, especially when sweating occurs infrequently (Dermatology 204: 173, 2002).
Angioedema: similar to urticaria, but a whole organ is involved. (When it's the tongue or larynx, the patient is in serious trouble.) It often results from C1-esterase inhibitor deficiency.
Allergic rhinitis ("hay fever"): sneezing and itchy conjunctiva due to exposure to airborne allergens (pollens, mold spores, house dust, mites, animal dander)
Allergic ("extrinsic") bronchial asthma: bronchoconstriction following inhalation of an allergen.
Generalized ("systemic") anaphylaxis: a life-threatening emergency in which seconds count. Review: Am. Fam. Phys. 68: 1325, 2003.
The commonest clinical setting is penicillin injection, insect stings, and certain "notorious" food allergies.
Three out of every 10,000 patients that get a penicillin injection have anaphylaxis, 10% of these people die from it. You have been warned.
One of the situations in which allergy shots work is
for allergy to insect stings (NEJM 351: 668, 2004).
Some anaphylaxis is "idiopathic" and recurrent. This can kill you.
 Laryngeal edema
Laryngeal edema
Anaphylaxis
WebPath photo
The entire vascular bed opens and leaks, causing blood pressure to drop catastrophically ("anaphylactic shock").
If the patient survives this, all the small airways clamp shut ("bronchospasm", hard to treat effectively).
The mainstay of treatment is epinephrine. Follow-up is a warning bracelet and an anaphylaxis kit!
Food allergies really exist and can cause any form of localized or generalized type I hypersensitivity.
Really severe reactions are known to occur to tiny doses of eggs (my late mother was like that), various nuts (Br. Med. J. 300: 1377 & 1378, 1990; Br. Med. J. 312: 1050, 1996), sesame seeds, shellfish, and fish. Yes, people do die of these (NEJM 327: 374, 380 & 424, 1992).
* A new study finds that having had a peanut-oil-based salve applied to a baby's rash increases risk of subsequent peanut allergy about sevenfold (NEJM 348: 977, 2003). Stay tuned.
Common allergies to wheat and cow's milk are less severe and unlikely to kill.
Food allergy review: JAMA 278: 1888, 1997. The "green" claim that genetically altered foods will be allergenic is an obvious disinformation campaign (common sense, and J. Allerg. Clin. Imm. 107: 765, 2001).
* Do not confuse IgE-mediated hypersensitivity to wheat or milk with gluten enteropathy, galactosemia, or lactose intolerance.
Chocolate, strawberries (* Shakespeare's Richard III), and codeine release histamine non-immunologically in everyone. (Some get it worse than others, and are "allergic").
* In the 1980's, cow's milk was blamed by some people for most diseases and behavior problems of young children. This goofy fad has pretty much died down.
* Conversely, many inexperienced physicians do not believe in food allergy. (Many food allergies are imaginary, and adults usually have enough sense to avoid foods that make them sick.)
A "pop" claim that pertussis immunization in infancy exacerbates allergy later simply isn't true (forced huge, long study: Br. Med. J. 328: 925, 2004).
Hypersensitivity as a cause of "functional" or "idiopathic" illness:
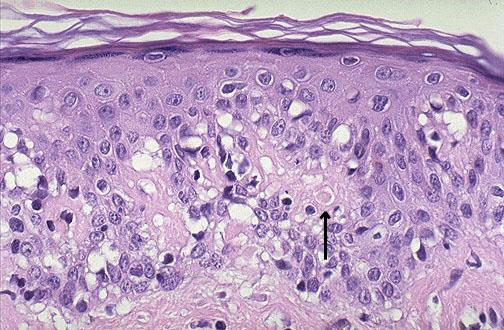
Atopic dermatitis ("eczema"), is a common skin disease that occurs in people who have other allergies. The current literature will leave you wondering whether food allergy is usually the underlying cause, or whether it's essentially a genetic disease, with out-of-synch mediators. And it's hard to decide, since there's no obvious link, and nobody's going to comply with an elimination diet because the disease usually responds nicely to today's topical glucocorticoids.
Thinking about atopic dermatitis has been revolutionized during the past few years by the discovery that in these patients, the dendritic macrophages express IgE receiptor (Fc[epsilon]RI) on their surfaces (J. Allerg. Clin. Imm. 112: 411, 2003).
{08161} atopic dermatitis ("eczema")
{12301} atopic dermatitis ("eczema"); this was probably contact dermatitis
Patch tests are used to confirm the sensitizing agents in type IV immune injury; these tend to be metals or chemicals, and the allergist will look for damage to the epidermis a few days later.
* Future pathologists: Look for tryptase (from degranulated mast cells) in the blood of those dying suddenly. It's a marker for anaphylaxis as long as the post-mortem interval isn't excessive. Serum total IgE and allergen-specific IgE is also coming into use (Am. J. Forens. Med. Path. 25: 37, 2004).
However, skin testing / patch testing are not altogether sensitive or specific. You will hear anecdotes of patients with "unexplained" illnesses that improved spectacularly upon withdrawal of a suspected allergen, and recur on subsequent allergen challenge. (There may or may not be evidence of type I hypersensitivity.)
The problems with this kind of evidence are obvious. * Two that I heard about from respected physicians during my residency involved severe asthma from xerox toner, and rheumatoid arthritis caused by onions in the diet.
For a case of rheumatoid arthritis caused by milk allergy, see Arthr. Rheum. 29: 220, 1986.
An unknown percentage of people suffer fatigue, malaise, behavior problems, "functional" headaches, "functional" bowel syndrome, etc., etc., due to allergy. These patients typically respond well to treatment of the allergy.
"Clinical ecology" is a term used by practitioners who propose to discover these patients. Legitimate allergists prefer the term "environmental medicine".
* "Cytotoxic testing" for food allergy is an old, cynical health fraud: Br. Med. J. 290: 538, 1985. So is "systemic provocation-neutralization testing": NEJM 323: 429, 1990, "electrodermal diagnosis" and "the reaginic pulse test". The funniest is probably "applied kinesiology", in which the "patient" holds some substance with arm outstretched, and the "integrative practitioner" pushes more or less hard on the arm to determine whether the allergen is causing weakness, the "holistic remedy" makes the person stronger, or whatever. I am not making this up.
* As a physician, you will learn very quickly that if you suggest that a person is likely to have/ to get a particular symptom, that person usually will develop it. "Multiple chemical sensitivities" (MCS, "idiopathic environmental intolerance") is a current pop diagnosis. People claim to be chronically ill because of various chemicals in the environment, kids who have to be in special classrooms where nobody uses cosmetics, etc., etc. People believe in this very strongly (Arch. Env. Health 57: 429, 2002), and today there are entire practices devoted to "environmental medicine" (Arch. Env. Health 56: 046, 2001) in which many of these people (adults, kids) are diagnosed. When these people are actually studied, the physiological changes for each chemical seem to take place at the odor threshold (Arch. Env. Health 57: 247, 2002), and beyond this not to vary with dosage -- exactly as you'd expect if the real cause is simply that people believe passionately that smells make them sick. Plus, they get sick off carbon dioxide (J. Allerg. 105: 358, 2000). This makes "multiple chemical sensitivities" and the associated disability one of the great iatrogenic diseases of modern times -- in this case, caused by "independent medical thought." When one group of academic researchers examined these claims and were unable to support them (Ann. Int. Med. 119: 97, 1993), the members were subjected to a horrible campaign of intimidation and legal harassment (NEJM 336: 1176, 1997.) Having dealt with quacks as long as I have, this doesn't surprise me; this can only make studying people who may really have a real disease cause by exposure to some environmental chemical impossible. As usual, the real losers are ordinary, decent people. A catalogue from one group of proponents (who dispute the psychogenic idea based on some uncontrolled independent-thought labs) lists every synthetic and petrochemical but no naturally-occurring scents (Env. Health Perspect. 105 S2: 417, 1997) -- a fact that invites an obvious conclusion. Today, it's obvious that even the "multiple chemical sensitivities" proponents are well-aware that they are on the defensive, and that the best evidence is that the illness is essentially psychogenic (Env. Health Perspect. 109: 161, 2001). A mainstream group discovers that almost everybody diagnosed with "MCS" was an abused kid: Reg. Tox. Pharm. 24: S-96, 1996 -- patients get both secondary gains and a chance to project the cause of their illness onto the chemical industry and an unsympathetic society. The group recommends a durable, caring relationship with a physician in which they can eventually figure out what's really going on, i.e., they they need to learn new living skills.
The BIG news in type I immune injury right now is the development of a monoclonal anti-IgE antibody (omalizumab) that seems useful in the treatment of allergic respiratory disease (asthma, hay fever). It was approved for clinical use in 2003. See Am. J. Resp. Crit. Care. Med. 164: Supplement, Oct. 15, 2001; NEJM 348: 986, 2003. Thanks to omalizumab, there is no longer any reasonable doubt that IgE is central to the entire gamut of allergic inflammation, including the accumulation of lymphocytes and eosinophils in tissue (J. Allerg. 115: 459, 2005).
 * If you are interested in allergic disease, ask:
* If you are interested in allergic disease, ask:
TYPE II IMMUNE INJURY IN HUMAN DISEASE
"Fixed antigens" bind antibodies.
In this type of hypersensitivity, antibodies attach to antigens on the surfaces of a cell, and then
something injures or destroys the cell.
If the antibodies are already circulating and fast-acting complement-fixers, the damage may be
complete within minutes.
If the antibodies need to be made for the occasion or are slow-acting, or if an anamnestic response
must take place, the injury will begin only after several days.
What can destroy an antibody-coated cell?
C9, at the end of the complement cascade, is cytolytic. Complement-fixing antibodies attaching to a
cell are likely to wreck it.
Cells with protruding Fc portions of IgG or coated with activated C3 bits are tasty to polys and
mononuclear phagocytes.
* Natural killer cells (NK-cells) and other cells with Fc receptors are supposedly able to destroy (i.e.,
cause apoptosis in) cells coated with IgG ("antibody-mediated cytotoxicity", supposedly important
in some endocrine diseases). Of course, the dying cells undergo apoptosis.
Better established is T-helper cell-mediated (you may
see this called "IV-B" instead of II, since T-cells do the damage)
cytotoxicity (Hashimoto's
disease, others). Apoptosis once again, of course. See below (and consider this a combination of
type II and type IV).
Transfusion reactions:
ABO incompatibility usually involves ready-made, complement-fixing IgM. So if your blood has
anti-A and you receive a unit of A red cells, the transfused cells will be destroyed in a few minutes
(and you'll be sick from all the potassium and stroma that was inside them!).
Rh incompatibility usually involves IgG which must be induced. If you are Rh ("D") negative, the
second time you encounter the Rh antigen, you may get a little sick when, beginning a few days
later, the transfused red cells are slowly destroyed.
In hemolytic disease of the newborn ("erythroblastosis fetalis"), the mother has become sensitized to
one of the father's red cell antigens (usually RhD)
which she does not share (probably during the birth of a previous
child, with mixing of fetal-maternal blood). If the isoantibody is IgG, it can cross the placenta and
wreck havoc on the fetus's red cells, causing anemia, normoblastic ("erythroblastic") hyperplasia,
etc. And when the baby is born, there's no placenta to carry all the breakdown products of
hemoglobin away, so the child becomes jaundiced. Review NEJM 339:
339, 1775, 1999.
"Autoimmune" hemolytic anemias result from the body's making antibodies against its own red cell
antigens (Rh-family antigens in the case of "Aldomet"-induced disease).
The same mechanism operates in some illnesses in which neutrophil precursors are wiped out.
Likewise, some people make antibodies against their own platelets, which are destroyed in the RE
system. (The best treatment is to remove the spleen.)
In most cases, why these antibodies develop is mysterious. Sometimes a hapten is involved
(high-dose penicillin in antibody-mediated hemolytic anemia, quinidine in some cases of
autoimmune thrombocytopenia.)
In paroxysmal cold hemoglobinuria, the antibody against the red cells (* "Donath-Landsteiner
antibody") is an IgM active only in the cold.
A typical story is the skier who falls in the snow, then passes dark brown urine (why?) when he or
she returns to the chalet.
The commonest cause, historically, is syphilis. Why this should be is utterly mysterious.
In Goodpasture's disease, the body makes antibodies against the basement membranes of the
glomeruli and lungs. Holes get punched in the vessels, and fibrin and blood fill and ruin the
nephrons and alveoli.
{00049} Goodpasture's, immunofluorescent view of antibody along glomerular basement membrane
In pemphigus and its relatives, the body makes antibodies against the molecules that hold the
epidermis together, and/or connect it to its basement membrane. The end result is blisters.
Some chronic autoimmune diseases feature antibodies against the cells that are being destroyed.
Whether these antibodies are pathogenic, or are the result of sensitization to proteins uncovered
following damage from cell-mediated (Type IV) injury is unknown.
These include juvenile-onset diabetes mellitus, lymphocytic (Hashimoto's) thyroiditis, autoimmune
("idiopathic") adrenocortical insufficiency, hypophysitis, parathyroiditis, Sjogren's syndrome, and
others.
Hyperacute rejection of a transplanted kidney occurs by this mechanism (see below; plus there's a
component of type III injury, why?)
We'll cover rheumatic carditis soon enough. The pathogenesis is complex.
A variant of type II immune injury involves antibodies against neutrophils (also
macrophage granules).
Probably substances are released from damaged phagocytes that in turn damage nearby vessels
and tissues. This is the underlying disease mechanism in Wegener's granulomatosis and small-vessel
polyarteritis.
We'll cover the anti-neuronal antibody syndromes throughout the course. These include:
the paraneoplastic encephalopathies (in which the autoantigen is in a cancer, and the immune
response to the tumor cross-reacts with brain or nerve), and
Lyme disease (antibodies against the bacterium cross-react with axon);
Sydenham's chorea, in which anti-streptococcal antibodies cause mood swings, obsessive-compulsive stuff, Tourette stuff, and
funny movements (see, for example, Ped. 93: 323, 1994).
One of the mechanisms by which uninfected T-cells are destroyed in AIDS is that debris from the
dead viruses coats T-cells and causes them to be destroyed by antibodies.
* An AIDS-like disease in mice caused by autoantibodies against your own CD4 and HLA
molecules: Nat. Med. 3: 37, 1997.
Antibody-mediated dysfunction
These are disorders in which autoantibodies do not destroy the cells or molecules to which they bind,
but cause them to malfunction.
"Circulating anticoagulants" are antibodies against a coagulation factor (usually VIII or
prothrombin activator).
These occur in many
patients with systemic lupus erythematosus (an autoimmune disease), and in
many hemophiliacs to whom the factor VIII they inject is a foreign protein.
Classic pernicious anemia is due to an auto-antibody that binds to intrinsic factor, rendering it
unable to carry vitamin B12 through the ileal mucosa.
A few cases of insulin-resistant diabetes mellitus are caused by autoantibodies that tie up insulin
receptors.
(And a few such antibodies stimulate the receptors, causing "autoimmune hypoglycemia". See
Lancet 1: 237 and 241, 1987.)
Diabetics injecting insulin of animal origin hope they will not start making antibodies against the
foreign protein. (If they do, they will have to switch to the recombinant human insulin, which is still
more expensive.)
In Graves' disease (which affected both Mr. & Mrs. George Bush), antibodies against hTSH
receptors of the thyroid bind and stimulate the receptor. The result is marked hyperthyroidism!
(Read about it in Hosp. Pract. 22(5): 147, May 15, 1987.
The autoantigen in celiac sprue / dermatitis herpetiformis is reticulin (Lancet 338: 724, 1991).
Induced by exposure to gluten in wheat, the exact way in which it causes harm is unclear.
* Another example of such injury is the rare "stiff-person syndrome", caused by an
autoantibody against glutamic acid decarboxylase, which synthesizes the neurotransmitter gamma-amino butyric acid (NEJM
318: 1012 and 1060, 1988). Similar (but not identical) is
neuromyotonia ("Isaac's disease"), with immune destruction of potassium channels (Lancet 338: 75,
1991). Yet another involves blocking antibodies to factors necessary for the growth of various
blood cells (NEJM 321: 97, 1989). Stay tuned. Chronic urticaria often results from autoantibodies
against the IgE receptor on mast cells (NEJM 328: 1599, 1993).
Aplastic anemia from autoantibodies against erythropoietin (as, after treatment with
the recombinant drug): NEJM 346:
469, 2002; Lancet 363: 1768, 2004.
TYPE III IMMUNE INJURY IN HUMAN DISEASE
"Soluble antigens" precipitate with antibodies. Usually this happens 2-4 hours
after exposure.
This sort of tissue injury is mediated by antigen-antibody complexes ("immune complexes")
If there is a great excess of either antigen or of antibody, mixtures of the two are readily soluble and
easily disposed of by the body (why?).
The problem occurs when antigen and antibody are present in just the right (wrong?) proportion.
They form huge lattices ("complexes").
The complexes get deposited around the body, typically in the walls of blood vessels (which
are nearby), the glomerulus (where proteins are concentrated),
the skin (where it's cold and things precipitate sooner),
and the synovium (nobody knows why). Complement
is fixed, vessels leak and spazz shut, polys and monos arrive and find nothing to attack (but attack
anyway), C9 punches holes in healthy membranes, and general havoc results.
* "Platelet involvement" in all of this might reasonably be explained by injury to the endothelium.
The process takes at least several hours to develop following exposure to the antigen (even if the
antibody is already present), but it can last for years.
* Patients with diseases thought to be caused by immune-complexes often (but not always) show
diminished ability of macrophages to devour such complexes. This is highly speculative, linked to
HLA-B8, DR3, etc., etc.
The model for localized immune-complex mediated tissue injury is the Arthus reaction, in which the
immune complexes form "in situ".
This accounts for some of the discomfort that develops several hours after an injection for
immunization. The whole-body counterpart is the horrible "serum sickness" following passive
immunization with horse serum. See below.
In "membranous glomerulopathy", antibodies complex with an antigen that is distributed at regular
intervals along the glomerular basement membrane. The immune complexes appear as a regular
series of bumps (and make the GBM look thick, hence the name).
When many or all vessels are involved with a severe type III hypersensitivity reaction, the classic
description is "serum sickness". (This term comes from the days when horse serum was
administered by vein for passive immunization, and people made anti-horse antibodies).
"Polyarteritis nodosa" is a serious disease sometimes due to type III hypersensitivity. In
around half of cases, the antigen is hepatitis B virus. Wait for changing definitions,
and remember that even your ordinary hepatitis B and hepatitis C patients
can get a vasculitis in the acute phase.
Rheumatoid factor is IgM antibodies again the Fc portion of IgG. These tend to precipitate in the
walls of vessels, producing a vasculitis.
Erythema nodosum is patches (vicious cycle) of vasculitis in the
subcutaneous fat, typically on the cool shins. It produces typical
red bumps. It's often secondary to some other disease or medicine,
but can be "idiopathic".
In other conditions, circulating immune complexes deposit in various tissues, and they are what gets
injured.
During acute infectious illnesses, we have all experienced several hours of joint aches. This is
probably due to immune-complex deposition (antibody plus bound infectious agent) in our synovial
membranes, with resulting edema and stretching of the joint capsules.
In the organic pneumoconioses ("farmer's lung", etc., diseases of the lungs due to inhalation of
organic dusts, ranging from mold spores to pigeon droppings), the problem is a pulmonary vasculitis
due to type III hypersensitivity.
In systemic lupus erythematosus, the patient makes antibodies against many of her own tissue
proteins and nucleic acids. Antigen-antibody ("immune") complexes are deposited in the glomeruli,
pleura, pericardium, synovium, skin, and elsewhere.
In drug reactions, systemic infections, carcinomatosis, etc., etc., "hypersensitivity angiitis" of small
arteries and small veins results from type III immune injury. The antigen is a drug, a micro-organism, a component of tissue
debris, etc., etc. -- i.e., you might not ever identify it. This is not an
uncommon problem in clinical medicine. A near-synonym is "leukocytoclastic vasculitis", because
of all the broken-down neutrophils seen in the vessel walls.
In AIDS and in several other viral illnesses, immune complexes of antibody-plus-virus adsorb onto
platelets. This results in their rapid destruction.
Vasculitis syndromes in autoimmune disease: Br. J. Rheum. 27: 251, 1998.
* Surprisingly, nobody's written anything on allergy shots
as possible causes of vasculitis for many years. It'd make sense... but if
it happens, we're not hearing about it.
TYPE IV IMMUNE INJURY IN HUMAN DISEASE
In type IV hypersensitivity, special T-helper cells (TD) programmed to recognize a particular
"altered self" antigen, are stimulated. They in turn coordinate other lymphocytes, macrophages, and
other tissue elements. The object is to destroy every cell bearing the "altered self" antigen.
This is great for ridding the body of virally infected cells, cells harboring intracellular parasites (TB,
some fungi), and perhaps tumor cells.
It is also the way the body acute-rejects transplanted organs (allografts).
The TD-cell programmed to respond to a particular antigen meets it in association with the class II
histocompatibility antigens (MHC-II, HLA-D, DR; "Ia's") of the dendritic macrophage that presents
it. This is a big deal.
The stimulated TD cell signals to other T-cells and macrophages, telling them that it is time for a
type IV hypersensitivity reaction.
All nearby resting T-CTL cells of all specificities are readied, and macrophages in the area are
stimulated ("become angry").
In addition, the TD cell produces interferon (helps anger the macrophages) and probably other
factors. (You will have to read about transfer factor yourself).
The now-stimulated T-CTL cell specialized for killing cells bearing a particular antigen will attack
when it encounters that antigen in association with the class I histocompatibility antigens (HLA-A,
B, C).
The T-CTL binds to the cell bearing the "altered self" antigen, and then may leave. A few hours
later, the cell bearing the "altered self" antigen bursts/undergoes apoptosis and dies. Unlike in
complement-mediated woes, "innocent bystanders" are spared. When this predominates, we talk
about "cell-mediated cytotoxicity"; some authorities call this "type V immune injury".
The molecular biology is now worked being worked out. A T-cell "kisses" the cell to be destroyed
on the fas antigen (J. Imm. 152: 1127, 1994), the common apoptosis trigger.
The angry macrophage has increased free radicals (including "superoxide"), more proteases, and
greater phagocytic ability. It even eats non-angered macrophages in which micro-organisms might
be growing.
Angry macrophages are the ones that become epithelioid cells.
Angry macrophages, unlike T-cells, aren't very smart and will eat whatever they can. This often
includes some of the surrounding healthy tissue.
"Cell-mediated immunity" is misleading today. It means that the sensitized and stimulated T-cell
that orchestrates the reaction can do it again when transferred alone to a non-sensitized host.
"Delayed type hypersensitivity" is another archaic term, from the days when only type I and type IV
hypersensitivity were known.
In any case, the reaction always takes a day or so to develop.
The model for type IV hypersensitivity is the tuberculin skin test.
A trace of extract from the TB microbe is injected into the dermis.
If TD cells specialized against TB microbes are abundant (i.e., the patient has previously met the TB
microbe), a brisk type IV hypersensitivity reaction will take place. Since macrophages dominate,
innocent bystanders will be hurt. A lump of angry macrophages and fibrin will be palpable beneath
the skin 48-72 hours later.
(If you know the person has had TB, don't do the test, or the angry macrophages will probably eat a
hole in the skin at the injection site.)
Lack of effective TD function occurs in some diseases (remember especially AIDS, sarcoidosis, acute measles, and any
disease that causes serious wasting)
and is called "anergy".
To test for anergy, do intradermal
skin tests using substances most everyone has once mounted a type IV
hypersensitivity reaction against (i.e., athlete's foot, candida yeast infection, mumps, tetanus toxoid). If there are no
lumps, the patient has "anergy".
Type IV hypersensitivity is familiar to anyone who has ever had poison ivy, a rash from a nickel
watch band, or a rash from * neomycin ointment. (All are haptens; suspect a hapten as at least part
of the problem in any case of contact dermatitis.)
{24955} dermatologist skin test; the guy was allergic to the ramrod (no, I don't know how it
happened or what it was made of)
Exposure to beryllium dust often excites an intense granulomatous reaction, due to the ability of TD
cells to recognize it.
Cell-mediated immunity also accounts for the inflammation of the skin in the viral exanthems.
(* The newest of these is the rash caused by AIDS virus.)
In viral hepatitis, the viruses may not really do the liver cells any harm, but they express their
antigens on the liver cell membranes. This upsets certain programmed TD cells, and soon
cell-mediated immunity is destroying the patient's own liver.
As noted above, type IV hypersensitivity may play a role in some autoimmune disorders.
Confusingly, most of these also feature antibodies against the tissue that is being attacked. Unlike in
classic type IV ("no antibodies") immune injury, the antibodies may be required for the injury to
proceed ("antibody-dependent cell-mediated cytotoxicity", "IV-B", thought to be important in
Hashimoto's autoimmune thyroiditis: NEJM 325: 238, 1991.)
* Or the antibodies might just be made in response to the release of damaged antigens following
type IV immune injury.
During the 1990's, it became clear that most cases of aplastic anemia (i.e., failure
of all three principal cell types in the bone marrow) result from T-cell mediated injury.
Spontaneous regression of pigmented nevi ("halo nevi") and malignant melanomas is attributed to
type IV hypersensitivity.
Type IV immune injury to trophoblast, apparently
a cause of chronic miscarriage (JAMA 273: 1933, 1995).
TRANSPLANT REJECTION
This is too complicated to discuss at the end of this lecture, and fairly esoteric. Worth remembering:
T-cells do most of the rejecting most of the time. The most antigenic cells of the graft are the
lymphocytes and donor macrophages.
Hyperacute rejection happens when the patient gets a allograft and already has antibodies against it
(oops!). There is a visible pattern of type III immune injury; type II has also occurred.
Acute rejection is mediated by T-cells ("acute cellular rejection")
and is basically done by cell-mediated immunity. Look for lymphocytes
in the parenchyma.
There may also be damage from antibodies and antigen-antibody complexes
("acute humoral rejection"), which shows as a vasculitis
with intimal edema and inflammation (lymphocytes, foam cells). Clinicians
say, "He's rejecting his kidney (or whatever organ)", even if it is suddenly happening years after the
transplant.
Chronic rejection is still rather mysterious, and is usual in old allografts. Mostly you will see
fibrosis of the organ and dense fibrous narrowing of the arterial lumens.
* The baboon liver xenograft: Lancet 341: 531 & 536, 1993. Do you think this was ethical or
unethical?
GRAFT VS. HOST DISEASE ("GVH")
When bone marrow or some other organ containing T-cells is transplanted into an immune-disabled
patient, T-cells in the graft attack the "foreign" histo-compatibility antigens of the recipient.
Natural killer (NK) cells may be responsible in humans, and lymphocytes are observed attached to
epithelial cells.
Acute graft vs. host disease may occur 20-100 days following a transplant, even if HLA antigens
appear identical.
It involves primarily the skin (dermatitis), intestine (diarrhea, malabsorption), and liver (biliary
epithelium -- jaundice, elevated serum alkaline phosphatase, portal fibrosis).
{12006} graft vs. host, skin lesions
In each organ, there is apoptosis of epithelial cells with only a scanty lymphocytic infiltrate, and
fibrosis in the lamina propria.
Chronic graft vs. host disease occurs after 100 days and is characterized by more widespread
involvement of epithelial surfaces and a more dense chronic inflammatory infiltrate. A
scleroderma-like syndrome can develop.
FINAL NOTES:
We have mentioned a number of interesting diseases during this unit. You will have plenty of time
to learn about them. For now, understand the big concepts.
Folk wisdom that "the mind affects the immune system" finds support from studies of the effects of
substances P and K (neuropeptides) on immune cells -- both stimulate production of interleukin 1,
interleukin 6, TNF, interferon beta-two (Science 241: several papers, 1988).
There are many experimental models in which psychological stress appears to promote the
development of certain diseases. At the same time, there are almost as many other experimental
models in which psychological stress prevents certain diseases. (I can supply both kinds of
references if you're interested. There's a lot of interest right
now in sympathetic overactivation -- super-stress, brain injury,
"sympathetic storm" -- and the subsequent release of interleukin-10
from monocytes -- which can be blocked by propranolol. Nat Med. June 1998.)
There is much we do not know about the relationship of the immune system and disease.
Speculating is fine, but be skeptical about grandiose claims. Today,
most proponents of unscientific remedies
claim whatever they do "strengthens the immune system" -- but they refuse to present data from
controlled studies. ("We will never treat 'whole persons' as statistics!") We look with hope on the
few "alternative practitioners" who are beginning to study their own methods fairly and honestly.
* Insects use lectins instead of antibodies; they have no B or T-cells, but they reject tissue transplants,
nobody knows how.
* Sir Winston Churchill, in hospital with an infection during World War II, looked at his hospital
chart and asked his physician, "What are these lymphocytes?" He was told: "We don't know, Prime
Minster." "Then why do you count them?" Churchill retorted. Retold in Nature 333: 804, 1988.
Now I lay me down to study
-- Author unknown!
 Allergic to packed red cells
Allergic to packed red cells
Pittsburgh Pathology Cases
 The coated cell was "opsonized", and "opsonin" is Greek for "relish", like on a hot dog.
The coated cell was "opsonized", and "opsonin" is Greek for "relish", like on a hot dog.
RhoGam, anti-Rh (* anti-D) antibody that is given to Rh-negative
women who have delivered or lost an Rh-positive baby, prevents sensitization.
This is now considered the premiere example of how to turn an immunogen
into a toleragen; ask a molecular biologist the details.
Goodpasture's disease
Linear fluorescence
WebPath photo
 Lupus kidney
Lupus kidney
Antibodies deposited in glomerulus
Urbana Atlas of Pathology
The molecular biology is only starting to be unravelled (Nat. Med. 6: 290, 2000).
 Transplant Immunology
Transplant Immunology
Great site
Transplant Pathology Internet Services
{12007} graft vs. host, skin lesions
Graft vs. Host in the lung
Lung pathology series; follow the arrows
Dr. Warnock's Collection
 Graft vs. host disease
Graft vs. host disease
Trust me; dead and dying cells
KU Collection
Graft vs. host
Biliary scarring and obstruction
WebPath photo
Graft vs. host
Biliary scarring and obstruction
WebPath photo
I pray the Lord I won't go nutty;
And if I fail to learn this junk
I pray the Lord that I won't flunk.
But if I do, don't pity me at all
Just lay my bones in the study hall;
Tell my teacher I did my best
Then pile my books upon my chest.
Now I lay me down to rest,
I pray I'll pass tomorrow's test.
If I should die before I wake
That's one less test I'll have to take.


| Visitors to www.pathguy.com reset Jan. 30, 2005: |
Ed says, "This world would be a sorry place if
people like me who call ourselves Christians
didn't try to act as good as
other
good people
."
Prayer Request
 Teaching Pathology
Teaching Pathology
PathMax -- Shawn E. Cowper MD's
pathology education links
Ed's Autopsy Page
Notes for Good Lecturers
Small Group Teaching
Socratic
Teaching
Preventing "F"'s
Classroom Control
"I Hate Histology!"
Ed's Physiology Challenge
Pathology Identification
Keys ("Kansas City Field Guide to Pathology")
Ed's Basic Science
Trivia Quiz -- have a chuckle!
Rudolf
Virchow on Pathology Education -- humor
Curriculum Position Paper -- humor
The Pathology Blues
 Ed's Pathology Review for USMLE I
Ed's Pathology Review for USMLE I
![]()
![]()
 | Pathological Chess |
 |
Taser Video 83.4 MB 7:26 min |

 Renal allograft rejection
Renal allograft rejection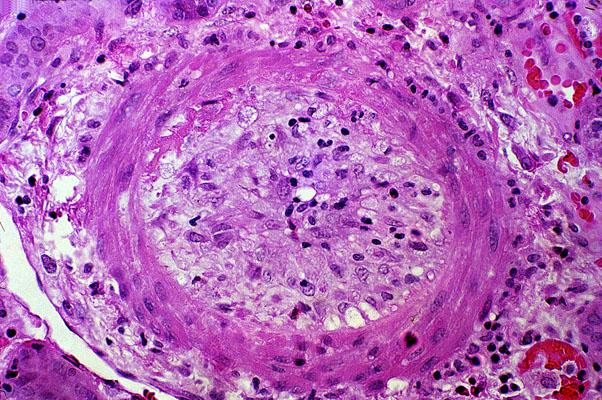 Acute transplant rejection
Acute transplant rejection Graft vs. host disease
Graft vs. host disease