Ed Friedlander, M.D., Pathologist
scalpel_blade@yahoo.com



Cyberfriends: The help you're looking for is probably here.
Welcome to Ed's Pathology Notes, placed here originally for the convenience of medical students at my school. You need to check the accuracy of any information, from any source, against other credible sources. I cannot diagnose or treat over the web, I cannot comment on the health care you have already received, and these notes cannot substitute for your own doctor's care. I am good at helping people find resources and answers. If you need me, send me an E-mail at scalpel_blade@yahoo.com Your confidentiality is completely respected.
 DoctorGeorge.com is a larger, full-time service.
There is also a fee site at myphysicians.com,
and another at www.afraidtoask.com.
DoctorGeorge.com is a larger, full-time service.
There is also a fee site at myphysicians.com,
and another at www.afraidtoask.com.
Translate this page automatically
 |
With one of four large boxes of "Pathguy" replies. |
 I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
Numbers in {curly braces} are from the magnificent Slice of Life videodisk. No medical student should be without access to this wonderful resource. Someday you may be able to access these pictures directly from this page.
Also:
Medmark Pathology -- massive listing of pathology sites
Freely have you received, freely give. -- Matthew 10:8. My
site receives an enormous amount of traffic, and I'm
handling about 200 requests for information weekly, all
as a public service.
Pathology's modern founder,
Rudolf
Virchow M.D., left a legacy
of realism and social conscience for the discipline. I am
a mainstream Christian, a man of science, and a proponent of
common sense and common kindness. I am an outspoken enemy
of all the make-believe and bunk that interfere with
peoples' health, reasonable freedom, and happiness. I
talk and write straight, and without apology.
Throughout these notes, I am speaking only
for myself, and not for any employer, organization,
or associate.
Special thanks to my friend and colleague,
Charles Wheeler M.D.,
pathologist and former Kansas City mayor. Thanks also
to the real Patch
Adams M.D., who wrote me encouragement when we were both
beginning our unusual medical careers.
If you're a private individual who's
enjoyed this site, and want to say, "Thank you, Ed!", then
what I'd like best is a contribution to the Episcopalian home for
abandoned, neglected, and abused kids in Nevada:
My home page
Especially if you're looking for
information on a disease with a name
that you know, here are a couple of
great places for you to go right now
and use Medline, which will
allow you to find every relevant
current scientific publication.
You owe it to yourself to learn to
use this invaluable internet resource.
Not only will you find some information
immediately, but you'll have references
to journal articles that you can obtain
by interlibrary loan, plus the names of
the world's foremost experts and their
institutions.
Alternative (complementary) medicine has made real progress since my
generally-unfavorable 1983 review linked below. If you are
interested in complementary medicine, then I would urge you
to visit my new
Alternative Medicine page.
If you are looking for something on complementary
medicine, please go first to
the American
Association of Naturopathic Physicians.
And for your enjoyment... here are some of my old pathology
exams
for medical school undergraduates.
I cannot examine every claim that my correspondents
share with me. Sometimes the independent thinkers
prove to be correct, and paradigms shift as a result.
You also know that extraordinary claims require
extraordinary evidence. When a discovery proves to
square with the observable world, scientists make
reputations by confirming it, and corporations
are soon making profits from it. When a
decades-old claim by a "persecuted genius"
finds no acceptance from mainstream science,
it probably failed some basic experimental tests designed
to eliminate self-deception. If you ask me about
something like this, I will simply invite you to
do some tests yourself, perhaps as a high-school
science project. Who knows? Perhaps
it'll be you who makes the next great discovery!
Our world is full of people who have found peace, fulfillment, and friendship
by suspending their own reasoning and
simply accepting a single authority that seems wise and good.
I've learned that they leave the movements when, and only when, they
discover they have been maliciously deceived.
In the meantime, nothing that I can say or do will
convince such people that I am a decent human being. I no longer
answer my crank mail.
This site is my hobby, and I presently have no sponsor.
This page was last updated February 6, 2006.
During the ten years my site has been online, it's proved to be
one of the most popular of all internet sites for undergraduate
physician and allied-health education. It is so well-known
that I'm not worried about borrowers.
I never refuse requests from colleagues for permission to
adapt or duplicate it for their own courses... and many do.
So, fellow-teachers,
help yourselves. Don't sell it for a profit, don't use it for a bad purpose,
and at some time in your course, mention me as author and KCUMB as my institution. Drop me a note about
your successes. And special
thanks to everyone who's helped and encouraged me, and especially the
people at KCUMB
for making it possible, and my teaching assistants over the years.
Whatever you're looking for on the web, I hope you find it,
here or elsewhere. Health and friendship!
QUIZBANK Blood & Lymph #'s 133-139, 178-333
 I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
Pathology Education Instructional Resource -- U. of Alabama; includes a digital library
Houston Pathology -- loads of great pictures for student doctors
Pathopic -- Swiss site; great resource for the truly hard-core
Syracuse -- pathology cases
Walter Reed -- surgical cases
Alabama's Interactive Pathology Lab
"Companion to Big Robbins" -- very little here yet
Alberta
Pathology Images --hard-core!
Cornell
Image Collection -- great site
Bristol Biomedical
Image Archive
EMBBS Clinical
Photo Library
Chilean Image Bank -- General Pathology -- en Español
Chilean Image Bank -- Systemic Pathology -- en Español
Connecticut
Virtual Pathology Museum
Australian
Interactive Pathology Museum
Semmelweis U.,
Budapest -- enormous pathology photo collection
Iowa Skin
Pathology
Loyola
Dermatology
History of Medicine -- National Library of Medicine
KU
Pathology Home
Page -- friends of mine
The Medical Algorithms Project -- not so much pathology, but worth a visit
National Museum of Health & Medicine -- Armed Forces Institute of Pathology
Telmeds -- brilliant site by the medical students of Panama (Spanish language)
U of
Iowa Dermatology Images
U Wash
Cytogenetics Image Gallery
Urbana
Atlas of Pathology -- great site
Visible
Human Project at NLM
WebPath:
Internet Pathology
Laboratory -- great site My team:
My team:Ed Lulo's Pathology Gallery
Bryan Lee's Pathology Museum
Dino Laporte: Pathology Museum
Tom Demark: Pathology Museum
Dan Hammoudi's Site
Claude Roofian's Site
Pathology Handout -- Korean student-generated site; I am pleased to permit their use of my cartoons
Estimating the Time of Death -- computer program right on a webpage
Pathology Field Guide -- recognizing anatomic lesions, no pictures

St.
Jude's Ranch for Children
I've spent time there and they are good. Write "Thanks
Ed" on your check.
PO Box 60100
Boulder City, NV 89006--0100
More of my notes
My medical students
Clinical
Queries -- PubMed from the National Institutes of Health.
Take your questions here first.
HealthWorld
Yahoo! Medline lists other sites that may work well for you

We comply with the
HONcode standard for health trust worthy
information:
verify
here. 

![]()
 Tulane Pathology Course
Tulane Pathology Course
Great for this unit
Exact links are always changing
Problems in Bone Marrow Path
Histopathology and essay
For pathologists
Lymph Node Exhibit
Virtual Pathology Museum
University of Connecticut
Hematology Atlas
Nivaldo Medeiros MD
Brazilian Pathologist
"Heme-Onc Pathology"
Virginia Commonwealth U.
Great pictures
Blood I
Introductory Pathology Course
University of Texas, Houston
Blood II
Introductory Pathology Course
University of Texas, Houston

Describe the distribution of lymphoid tissue in humans, with special reference to B- and T-cell zones. Describe the microanatomy of the lymph nodes. Sketch the sequence by which a B-cell develops into a plasma cell, and name each stage.
Distinguish relative and absolute counts of various white cells, and explain why absolute counts are more meaningful. Calculate an absolute count by multiplying the total and percentage counts. Give the healthy absolute counts for lymphocytes, monocytes, eosinophils, and neutrophils.
Given a name of a white cell marker, tell what cell(s) it identifies. Given a white cell type, mention its major markers.
Given a patient with neutropenia and a history, come up with a reasonable differential diagnosis. Describe the typical cause and course of agranulocytosis. Recognize the major causes of lymphopenia.
Give a reasonable differential diagnosis for granulocytosis, eosinophilia, and lymphocytosis. Tell how to distinguish chronic myelogenous leukemia from leukemoid reaction. Describe possible peripheral (i.e., circulating) white cell pictures in sepsis. Mention the significant disease association for increased absolute basophil count.
Describe the important non-neoplastic causes of lymphadenopathy, and how each looks under the microscope. Describe "infectious mononucleosis syndrome", and name its four principal etiologic agents.
Explain how a pathologist distinguishes a malignant lymphoma from a worrisome reactive (benign) lymph node. Do this yourself for an easy case.
Apply the unifying "rules" in this handout to clinical problems about non-Hodgkin's lymphomas. Explain how the classic Rappaport system differs from the International Working system and the Revised European-American system of lymphoma nomenclature. Recognize the names of the low, middle, and high grade lymphomas.
Given the name of a non-Hodgkin's lymphoma, recognize its distinctive features. Identify non-Hodgkin's lymphomas based on their idiosyncratic markers, etiologies, or epidemiologies.
Explain current thinking about the pathogenesis of Hodgkin's disease. Describe its epidemiology, subtypes, and prognosis. Given a description of the background, name the subtype, and vice versa.
Describe the major kinds of leukemia in detail. Cite their etiologies (if known), pathogenesis, natural histories, subclasses, diagnostic features, and current prognosis. Do the same for the myelodysplastic syndromes, polycythemia vera, and agnogenic myeloid metaplasia.
Describe the pathogenesis, symptoms, signs, lab findings, diagnosis, typical course, and major complications of plasma cell myeloma. Recognize and prognosticate the other "plasma cell disorders". Recognize the noteworthy causes of polyclonal gammopathy.
Explain current thinking about Langerhans cell histiocytosis (histiocytosis X).
Given an enlarged spleen and the opportunity to ask questions, come up with a reasonable differential diagnosis. Describe the common findings in spleens at autopsy.
Name the lymphoma and/or leukemia caused by with each of these viruses:
Epstein-Barr virus
HTLV-I
HTLV-II
HIV
Correctly define and use the following terms:
agranulocytosis
Auer rod
Bence-Jones protein
blast
bcr/abl oncogene
chloroma / granulocytic sarcoma
cleaved (clefted) lymphocyte
convoluted lymphocyte
cryoglobulin
Dohle body
gammopathy, monoclonal
gammopathy, polyclonal
leukemia
leukemia, aleukemic
leukocyte alkaline phosphatase
leukocytosis
leukoerythroblastic smear
leukopenia
lymphadenopathy
lymphoma
M-protein
myeloid / myelogenous
myeloma
neutropenia
paraprotein
Pautrier microabscess
Philadelphia chromosome
polycythemia (absolute, relative, 1,2)
pseudolymphoma
tingible body macrophage
toxic granulation
Identify the following elements in peripheral and/or marrow smears:
all five type of normal white cells
Pelger-Huet anomaly
circulating blasts
Auer rods
teardrop reds
Shown an appropriate peripheral smear, tell when each disease might be present:
Pelger-Huet anomaly
acute leukemia (subtype if possible)
chronic myelogenous leukemia
chronic lymphocytic leukemia
hairy cell leukemia
agnogenic myeloid metaplasia
Sézary's syndrome
Identify all the following cells in microscopic sections:
normal lymphocytes
small cleaved lymphocytes
large lymphocytes
immunoblasts
normal plasma cells
normal eosinophils
classic Reed-Sternberg cells and their major variants
Identify each of the following disease patterns under the microscope:
follicular hyperplasia
sinus histiocytosis
nodular non-Hodgkin's lymphoma
diffuse non-Hodgkin's lymphoma
Hodgkin's disease (& subtype if obvious)
Sézary's syndrome / Mycosis fungoides
Burkitt's lymphoma
myelofibrosis
extramedullary hematopoiesis in spleen
plasma cell myeloma
Draw or recognize a Birbeck granule and describe its significance.
INTRODUCTION
You will refer to this material every time you feel a large lymph node or spleen, or have a patient with an abnormal CBC.
This is also the most difficult unit in Medical Pathology except for glomerular disease. You can't learn it if you are not continually asking yourself, "Why?"
You are already familiar with the development of the different kinds of white cells, and the locations of lymphoid tissue throughout the body (lymph nodes, Waldeyer's ring, Peyer's patches, spleen, large airways).
T-cell zones: thymus, lymph node parafollicular cortex, splenic white pulp near arteriole
B-cell zones: germinal centers and their mantles, splenic white pulp at its margins
Among circulating lymphocytes, 80% are T-cells, and 20% are B-cells.
* You are also familiar with the common reaction patterns of various white blood cells: acute inflammation, pus, granulomas, and accumulations within phagocytes. (There's no need, for example, to talk right now about xanthomas, lipogranulomas, etc., etc.)
In discussing diseases that affect numbers of white blood cells in the peripheral blood, it is much more useful to talk about absolute cell counts than "percentage counts".
Of course, you can estimate the absolute count by multiplying the total WBC count x the % for a particular cell.
Healthy absolute counts:
Basophils: * few- 100/cu mcL
Eosinophils: few- 400
Lymphocytes: 1200-3400 (* 3000-7000 for kids)
T4 helper lymphocytes: >1000
Monocytes: 100- 590
Neutrophils: 1800-6500
Note that "95% lymphocytes" might mean either agranulocytosis (if the total white count is 2000) or chronic lymphocytic leukemia (if the total white count is 100,000).
* Current smokers average 25% higher neutrophil counts; those who've quit in the last five years still average higher (Am. J. Clin. Path. 107: 64, 1997). This won't matter in your clinical decision-making.
A good "normal range" for total white count is 4000-11000/cu mcL. "Leukocytosis" is present when the white count exceeds 12,000/cu mcL.
The most important "white cell diseases" are neoplastic. These are:
(1) the malignant lymphomas (Hodgkin's and non-Hodgkin's), solid tumors of lymphocytes (the rare tumors that truly arise from histiocytes are also included here; no one knows the true cell of origin of the malignant cells of Hodgkin's disease, which is also included here)
(2) the leukemias and their close relatives, the myeloproliferative disorders, in which sick hematopoietic stem cells proliferate
(3) the plasma cell disorders, which typically produce antibodies and/or fragments thereof
(4) the Langerhans cell histiocytosis family ("histiocytosis X"; "disseminated histiocytosis") of quasi-cancers, much less common than the others
Probably because it is so easy to harvest the cells, and since chemotherapy has been more successful for these diseases than for most other cancers, a tremendous amount of study has gone into clarifying their molecular pathology. Mega-review Am. J. Clin. Path. 112(1S1): S-76, 1999.
White cell markers oversimplified:
* PAS+ chunks ("blocks"): immature lymphocytes or M6 leukemia
TdT: immature lymphocytes
E-rosettes: T-cells
{16282} E-rosette, around a T-cell
CD4, CD8, others: T-cells (various kinds)
* CD68: common macrophages
CD1a (T6): some T-cells, all Langerhans macrophages (* works best on frozen sections)
CD10 (CALLA): most B-cells
CD45 ("common leukocyte antigen"): all white cells (* exception: Reed Sternberg cells)
Surface Ig(M, etc): B-cells
kappa, lambda: B-cell, plasma cells
cytoplasmic Ig: plasma cells
nonspecific esterase: monocytes
Fc receptor: B-cells, monocytes
TRAP: hairy-cell leukemia
HLA-D/DR /Ia: Langerhans cells and other antigen-presenting macrophages; some other cells
lysozyme: monocytes
* alpha1-antichymotrypsin: monocytes
erythrophagocytosis: monocytes
(myelo-)peroxidase: granulocytes
* Sudan black: granulocytes
* chloroacetate esterase: neutrophils, basophils, mast cells
platelet markers: megakaryocytes
* PAS+ diffusely: erythrocytes, megakaryocytes/platelets
* S-100, CD1/T6: dendritic ("Langerhans") macrophages
* {16517} neutrophil, chloroacetate esterase stain
NORMAL LYMPH NODE ANATOMY
Lymph nodes are soft (i.e., reticulin-framework) ovoids, up to about 2 cm in health. Afferent lymphatics penetrate and travel within their capsules (metastatic cancer first sets up here). Afterwards, lymph percolates through the cortex, and then the medulla, leaving by the hilum.
Within the cortex, there are generally some germinal centers ("lymphoid follicles"), sites of actively-proliferating B-cells. Each germinal center is surrounded by a mantle of resting B-cells, which are in turn surrounded by "parafollicular" T-cells. (If there is no antigenic stimulus, you'll see only "primary follicles" of sleepy B-cells in the cortex.)
The next time you get to look at a germinal center under the microscope, check out those proliferating B-cells. The sequence from small B-cell to plasma cell is interesting and unsung in most histology courses. You'll need to know this to understand lymphomas:

Within the medullary cords, expect to see a mix of B- and T-cells and plasma cells. The sinusoids are lined by fixed phagocytes.
Despite the elegant pictures in histology books, lymph nodes are almost never "normal", especially in adults.
NEUTROPENIA: A low absolute neutrophil count in the peripheral blood for any reason. (NOTE: "Leukopenia" is a not-very-useful word that describes any low total white count.)
Possible causes include
Suppression of granulopoiesis
"The aplastic anemias" (better, "bone marrow failure")
Bad stuff in the marrow
Space-occupying lesions ("myelophthisic anemias")
Solid cancers
Granulomas
Hematologic malignancies that suppress granulopoiesis (i.e., some ls and lymphomas)
DNA problems
Cancer chemotherapy
Radiation sickness
"The megaloblastic anemias"
* Lab machine didn't count them.
Hereditary cyclic (q. 3 wk., severe; molecular biology Blood 92: 2629, 1998; one cause is mutated neutrophil elastase; also Nat. Genet. 35: 90, 2003)
* Kostmann's hereditary agranulocytosis
* Shwachman-Diamond (genetic, also fatty pancreas)
Typhoid fever
Occasional virus infections (mild suppression, especially parvo B19)
* ALL with large granular lymphocytes
* Myelokathexis (group of genetic diseases with accelerated neutrophil precursor apoptosis; survivors are hypersegmented and have very long bars between nuclear lobes: Blood 95: 320, 2000; Am. J. Hem. 62: 106, 1999).
Idiopathic
Excess destruction of neutrophils
Autoimmune (rare, think of lupus)
Hypersplenism (see below)
Sequestration in a rapidly-growing abscess (??)
Idiopathic
Drugs: The mechanisms are typically obscure
Chlorpromazine (* ? anti-DNA synthesis)
Aminopyrine, sulfa drugs (* ? haptens, type II/III injury)
Phenylbutazone, chloramphenicol (* ?? mechanism)
Personal-trivial
Some Black people just have slightly low neutrophil counts
Some women get a mild neutropenia around their periods
Agranulocytosis is a time-honored misnomer for neutropenia sufficiently severe to put a person at risk for serious infection (i.e., neutrophil counts of 1000 or less, often much less; <500 is a big emergency).
The first sign is typically mouth ulcers ("there's lots of germs in there") with their pseudomembranes laden with infectious bacteria and/or fungi.
Later, the body is overwhelmed by bacteria, with death ensuing in a few days. Until the very end, patients are likely to complain only of "just not feeling quite right".
The usual cause of this nasty problems is medications. Future docs: If you notice that somebody has an absolute neutrophil count <1800 or so, stop all medications and check again in a week.
Lymphocytopenia is less common and less perplexing than neutropenia. Think of hereditary immunodeficiency, radiation injury, marasmus/kwashiorkor, Cushing's syndrome, or just "stress".
LEUKOCYTOSIS: It's worth remembering the following non-neoplastic causes of elevated white cell counts. Most of them make sense:
You remember that in health, about half the neutrophils in the blood are circulating, and the other half are marginated, at any time.
Lots of neutrophils ("granulocytosis"):
(don't forget surgery and myocardial infarcts)
glucocorticoids and epinephrine do the same thing;
glucocorticoids also prevent neutrophils from entering tissues
NOTE: Typhoid patients and some super-septic patients may become neutropenic because granulopoiesis is suppressed and/or all the neutrophils have emigrated from the blood. Beware of relying on white count as your chief marker for infection!
NOTE: The super-sick, septic patient is likely to have toxic granulation (extra-prominent azurophilic granules), cytoplasmic vacuoles ("from doing all that phagocytosis"), and/or Dohle bodies (rough endoplasmic reticulum remnants). By contrast, if the neutrophil count simply rises from acute pain and "stress", there will be no toxic granulation, vacuolization, or left shift. More about these in "Clinical Pathology".
{13646} Dohle body
{13661} Dohle body
{16213} Dohle body
* Future pathologists: The latter two "Dohle bodies" are fakes; they are from cases of May-Hegglin's (say "Muh-HAY-lun") semi-disease, an autosomal dominant trait with too-few, too-big platelets and lots of "Dohle bodies"; the neutrophils function normally. May-Hegglin "Dohle bodies" are actually non-muscle myosin A, gene mutated in May-Hegglin: Nat. Genet. 26: 106, 2000; Blood 97: 1147, 2001. There are several different phenotypes at the locus (Blood 102: 529, 2003).
* Morulae of ehrlichiosis can help you diagnose this famous "spotless fever"; this "granulocytic" variant of ehrlichiosis can be fatal (NEJM 334: 209, 1996).
NOTE: Left shift refers to presence of immature white cells in the peripheral blood, i.e., they're being mobilized early from the bone marrow. To tell an extreme case (WBC>up to 100,000 or so, i.e., a leukemoid reaction, as in sepsis, overwhelming TB, or carcinomatosis) from chronic granulocytic leukemia (see below), remember the following:
(1) In chronic granulocytic leukemia, the leukocyte alkaline phosphatase tends to be low. In sepsis and the non-leukemic myeloproliferative disorders, it tends to be high.
Leukocyte alkaline phosphatase is a completely different test from the "serum alkaline phosphatase" on the chemical profile. DON'T talk about them together.
(2) In chronic granulocytic leukemia, the absolute basophil count is generally high, too. This would be unusual in sepsis.
(3) In chronic granulocytic leukemia, there is virtually always a switch of material between chromosomes 9 and 22 (i.e., the Philadelphia chromosome (Ph') or at least its molecular equivalent). You won't see this except in cancer.
(4) And of course, toxic granulation / toxic vacuolization says "infection", not "leukemia".
Philologists: Right shift refers to the hypersegmented granulocyte nuclei of pernicious anemia (etc., any major impediment to normal DNA synthesis will produce this "megaloblastic" change). "Right" and "left" derive from spaces on the old do-it-by-hand tally sheets.
Lots of eosinophils (big review Mayo Clin. Proc. 80: 75, 2005):
type I immune injury
food allergy (supposedly)
hay fever (supposedly)
eczema (supposedly)
extrinsic asthma (supposedly)
bronchocentric granulomatosis (aspergillus superinfection in asthma; this one's important)
* hyper-IgE ("Job's") immunodeficiency
tissue parasites
ascariasis
filariasis (includes "tropical eosinophilia" of the far east)
onchocerciasis
strongyloidiasis
trichinosis
echinococcus
visceral larva migrans (dog and cat roundworms)
cutaneous larva migrans (dog and cat hookworms)
Drug allergy (most any; but notoriously gold therapy for arthritis, where eosinophilia is almost expected)
Hodgkin's disease (a large minority of cases)
Churg-Strauss (a vasculitis, often with granulomas, usually with ANCA; it's not clear whether this is a separate disease, or simply the way Wegener's / polyarteritis manifests in folks with allergies)
dermatitis herpetiformis
"idiopathic" nonfamilial hypereosinophilic syndrome ("Loeffler's" family; can damage organs)
Familial hypereosinophilia (locus unknown, autosomal dominant, mild: Blood 103: 4050, 2004)
* Well's eosinophilic cellulitis
eosinophilia-myalgia syndrome (from the tainted tryptophan)
* any AIDS patient with a rash (Am. J. Med. 102: 449, 1997)
* pemphigus (I don't know why)
* dermatitis herpetiformis
* acute liver transplant rejection (almost all have it, no one knows why)
* dermatomyositis
* others
polyarteritis nodosa (don't miss this one)
Loeffler's pneumonia/endocarditis (possibly eosinophilia itself damages the endocardium; "PIE syndrome", or pulmonary infiltrates with eosinophilia, is a severe Loeffler's)
* Kimura's disease (very high IgE, eosinophil-lymphoid pseudotumors of head and neck, marked peripheral eosinophilia; common in Asia, rare elsewhere; making the call Pediatrics 110: e-39, 2002; probably a low-grade lymphoproliferative disorder Am. J. Surg. Path. 26: 1083, 2002)
* Mastocytosis with eosinophilia (molecular signature known, response to imatinib/Gleevic likely)
* Idiopathic syndrome (rare -- T-cell clone makes interleukin 5: NEJM 341: 1141, 1999)
NOTE: In the developed world, among clinically healthy patients with isolated elevated eosinophil counts, you will often not find the cause.
NOTE: I've been doing CBC's for years on medical students, many of whom have hay fever, etc., and have never found one with an elevated eosinophil count.
NOTE: Remember that eosinophilic counts are up in the afternoon and down in the morning; I'd suggest taking a serious look at an absolute eosinophil count over 350 or so in the morning, and over 650 in the afternoon.
NOTE: The "Loeffler's eosinophilic" problems are a curious, mixed-bag of diseases with excessive numbers of eosinophils in various tissues.
* In other cases, the eosinophils themselves seem to be the mutated clone: Blood 93: 1651, 1999.
{14099} eosinophilic leukocytes (buffy coat)
{09207} eosinophil granule with crystal (electron micrographs; these crystals will combine to form large
Charcot-Leyden crystals under some conditions)
* Lots of monocytes:
typhoid fever
bad granulomatous problems
TB
brucellosis
Crohn's disease
leprosy
deep fungi
sarcoidosis
others
chronic autoimmune disease
rheumatoid arthritis is worth remembering
rickettsial disease
disseminated cancer (occasionally)
Lots of lymphocytes:
"infectious mononucleosis" (see below)
whooping cough ("pertussis"; the toxin keeps the T-cells from homing to lymphoid tissue)
infectious lymphocytosis (mild kids' disease, with T-cells, caused by various non-herpes viruses notably coxsackie B2; a "chronic form" also exists without marrow abnormalities)
"transient stress lymphocytosis" (absolute counts 4000-10000; on the evidence we've overlooked this for years; all major lymphocyte subsets go up, and neutrophils go up too: Am. J. Clin. Path. 117: 819, 2002)
* really bad "collagen-vascular disease"
* phenytoin ("Dilantin") or para-amino salicylic acid ("PAS") therapy
NOTE: Infectious mononucleosis is a family of diseases featuring fever, malaise, fatigue, lymphadenopathy, and circulating benign atypical lymphocytes. The syndrome results from first meeting one of these four micro-organisms: (1) Epstein Barr virus; (2) cytomegalovirus; (3) toxoplasmosis; (4) HIV. Benign atypical lymphocytes are activated cells (B- or T-) seen typically in the blood in "infectious mononucleosis" and ceratin other infections. The nucleoli are small, the nucleoplasm is reticulated, and the cytoplasm is typically blue, at least where the red cells indent them.
Lots of basophils:
chronic myelogenous leukemia
other "chronic myeloproliferative disorders"
polycythemia vera
* primary hemorrhagic ("essential") thrombocythemia
* supposedly in lots of other things, big deal.
NOTE: None of these "classic findings" is either particularly sensitive, or particularly specific, for any
particular disease. Use this information in the setting of the "whole person".
 Infectious mononucleosis
Infectious mononucleosis
Blood picture
WebPath Photo
ODD NEUTROPHILS:

Familial Mediterranean Fever, long-mysterious, has now yielded up its secrets.
Lacking pyrin, neutrophils mob body cavities every once in a while. In addition to fever, patients may have pleuritis, arthritis, peritonitis, and/or a hot rash (looks like a strep infection) on the ankles.
Colchicine, famous for its ability to slow down neutrophils (as in acute gout), controls the attacks and prevents the dread complication of secondary amyloidosis.
As you can imagine, FMF can mimic most diseases. Don't miss it.
Molecular genetic diagnosis: Ann. Int. Med. 129: 539, 1998.
You recall Chediak-Higashi syndrome, in which there are several problems with neutrophil membrane and platelet dense body synthesis synthesis.
{16208} Pelger-Huet, one dose
{16209} Pelger-Huet, one dose
{13658} Pelger-Huet, two doses
* Alder-Reilley anomaly merely refers to large, mucopolysaccharide-laden granules in some
of the storage diseases (Hunter's, Hurler's, Tay-Sach's, occasionally "all by itself").
* Thankfully rare: Lack of endothelial adhesion molecules for
phagocytes (J. Clin. Invest. 103: 97, 1999) or lack of
CD18 integrin on neutrophils (Blood 91: 1520, 1998).
Bacilli in neutrophil vacuoles: Usually DF2 (dog bite)
* And you know that drumsticks are the inactivated X-chromosomes of lyonization.
LYMPHADENITIS: Inflammation of the lymph nodes
Acute lymphadenitis described in "Big Robbins" is not much more than the hyperplasia in a reactive
node.
Localized lymphadenitis is most often due to a bacterial infection in the area drained by the lymph node.
Really bad cases have polys and even abscess formation within the nodes. The end result will be a
scarred-up lymph node. You have one or more.
Generalized lymphadenitis suggests a systemic viral infection.
"Mesenteric adenitis", often indistinguishable from acute appendicitis, is caused by Yersinia
enterocolitica.
Acute lymphadenitis, since it comes up suddenly and stretches the capsule, is likely to make the node
tender.
Chronic non-specific lymphadenitis falls in one of three distinctive patterns.
Follicular hyperplasia (i.e., lots and lots of big follicles) results from longstanding contact with
organisms or "other things" that stimulate the B-cells. If perplexed, think of:
{36371} toxoplasmosis; many bugs in a cell
Paracortical lymphoid hyperplasia (i.e., lots and lots of lymphocytes, including turned-on ones, in the
T-cell regions of the cortex) results from longstanding contact with organisms or "other things" that
stimulate the T-cells. If perplexed, think of
Sinus histiocytosis (i.e., sinusoids with swollen endothelial cells and lots of histiocytes). If perplexed,
think of:
Mixtures of the above cause diagnostic problems. In all the above, capillary endothelial cells are likely
to be hyperplastic (rare in cancer).
"Big Robbins" fails to mention perhaps the most common cause of "unexplained" lymph node
enlargement, especially in the groin: Dermatopathic lymphadenitis, melanin and sebum-laden nodes
draining chronically inflamed skin.
{35609} dermatopathic lymphadenitis (the red-brown is melanin, the white is sebum)
WARNING: Any of these patterns can be (and occasionally is) mistaken for malignant lymphoma by
the inept. Note that the finding of mitotic figures or necrosis doesn't necessarily point to malignancy,
while the presence of a variety of cell shapes actually suggests a benign diagnosis. Know your
pathologist, and ask for consultation if you are in doubt.
Mixed granulomatous-suppurative lymphadenitis
We've seen this list before. The causes of this curious, important reaction are (1) lymphogranuloma
venereum, (2) cat scratch fever, (3) brucellosis, (4) plague, (5) tularemia, (6) glanders-melioidosis, and
(7) miscellaneous yersinia infections.
* Angioimmunoblastic lymphadenopathy is a reaction pattern with proliferation of vessels and B- or T-immunoblasts.
Patients have systemic signs and often go on to die of immunoblastic lymphoma; HIV
is another cause, and herpes 8 is now implicated in yet other cases (Blood 87: 3903, 1996).
{23647} * angioimmunoblastic lymphadenopathy (note the vessels and the monomorphic cell infiltrate)
* Kikuchi-Fujimoto necrotizing histiocytic lymphadenitis: Nobody knows the cause of what seems to
be a viral illness (Arch. Path. Lab. Med. 118: 134, 1994); the molecular
biology is not that of a lymphoma: Am. J. Clin. Path. 117 627, 2002.
Nepalese study: Arch. Path. Lab. Med. 127: 1345, 2003.
Lymphadenopathy is a clinician's word for a big lymph node.
NON-HODGKIN'S LYMPHOMAS: By definition, monoclonal, malignant tumors of the B- or T-cells,
and not of plasma cells, and not Hodgkin's disease. Together, the lymphomas are common. By custom,
soft tumors of monocytes are included here because they look similar.
Update, with a focus on molecular markers: Br. Med. J. 362: 139, 2003; also Lancet 362:
139, 2003.
Big review: Cancer 75(S1): 370, 1995. Cancer of lymphocytes or maybe macrophages.
The non-Hodgkin's lymphomas are a subject of perennial fascination for pathologists. Making the
diagnosis ("benign or malignant?") is often tough, and classifying the non-Hodgkin's lymphomas
(hereinafter "lymphomas") was a major international sport through the 1970's.
Today, the ongoing fascination is in the chromosomal translocations that
are the primary way in which white blood cells acquire mutations. Especially
in the lymphomas, the genome is usually not destabilized.
Review of the translocations: Arch. Path. Lab. Med. 127: 1148, 2003.
Students often find this subject especially difficult to understand. Hence, the focus in this section on
"Rules".
RULE: All monoclonal proliferations of lymphocytes are best considered malignant. (Some monoclonal
plasma cell proliferations might be benign.)
RULE: Most lymphomas are somewhat more common in men, with the most pronounced difference
probably being T-lymphoblastic lymphoma (> 2:1).
RULE: Blacks and children almost never get nodular lymphomas.
RULE: A few lymphomas have one or more special risk factors (i.e., helicobacter in the stomach).
For most, however, the only known
risk factors are previous irradiation and immunosuppression.
Environmental risk factors for lymphoma
are poorly-understood; currently there's an interest in herbicides and pesticides
(I think it's probably real but a relatively minor risk -- Am. J. Epidem. 147: 891, 1998, Occup. Environ. Med. 60: E11, 2003;
others)
and hair-coloring agents (U.S.; review Cancer Inv. 18: 467, 2000 & Cancer Causes & Control 10:
617, 1999 from the FDA; relationship
if any is clearly weak; Am. J. Pub. Health 88: 1767, 1998 no animal model), as well
as the African poinsettia (Burkitt's).
RULE: At surgery or autopsy, lymphoma tissue feels like "fish flesh" (i.e., there is very little fibrosis)
or "firm rubber" (i.e., there is some fibrosis).
RULE: Fatigue, malaise, night-sweats, fever, and weight loss are the usual symptoms (if any) of these
diseases. Current thinking focuses on the production by the cancer of tumor necrosis factor-beta as a
cause (Br. Med. J. 305: 265, 1992), but nobody is sure.
A significant number (in some series, as many as half) of patients with "fever of unknown origin" prove
to have non-Hodgkin's or Hodgkin's lymphoma.
RULE: A majority of lymphomas arise in the lymph nodes (one or more groups). Several groups of
nodes may pop up at once. Nodular lymphomas almost always arise in lymph nodes.
RULE: A large minority arise in extra-nodal lymphoid tissue, i.e., Waldeyer's ring, stomach, terminal
ileum, skin, marrow.
RULE: When lymphomas arise in lymph nodes, they present as non-tender enlargement.
RULE: Lymphomas metastasize to other lymphoid tissues (nodes, spleen, etc.), and eventually to the
marrow, blood ("leukosarcoma", less often "lymphemia") and other organs. Low-grade lymphomas
metastasize as small nodules, while high-grade lymphomas metastasize as bulky masses.
RULE: Mitotic figure counts tell the growth rate of a lymphoma, but unless the mitotic figures are
bizarre, they do not help distinguish it from a benign lymph node. (Have you ever "counted mitoses"
in a normal germinal center? Try it!)
RULE: The lower the grade of the lymphoma, the more likely the bone marrow is to be involved at the
time of diagnosis. Paradoxical, no?
RULE: Lymphomas tend to spread to sites according to their B-cell or T-cell origin. Skin lymphomas
are usually of T-cell origin.
RULE: The malignant cells of lymphomas are more uniform than the mix of cells normally seen in
lymphoid tissue, and they recapitulate some phase in the life history of either normal B-cells or T-cells.
Don't expect to see much "cytologic atypia" in a lymphoma. Remember that the genome is usually
not destabilized in lymphomas. (Immunoblastic lymphomas can look
pretty wild.)
RULE: Lymphomas that grow as nodules within a lymph node ("trying to be germinal centers") are
called nodular or follicular (synonyms). They are always of B-cell origin, and the lymphoma cells will
closely resemble one of the forms in the sequence from resting B-lymphocyte to plasma cell.
The nodules will be back to back and lack good mantles.
{23581} nodular lymphoma
RULE: Nodular lymphomas are indolent lesions with natural histories that are relatively unaffected by
chemotherapy. However, they are not curable. Each nodular lymphoma has a better prognosis than its
diffuse counterpart, and is likely to transform into it sooner or later. This makes sense, since follicle
formation is a sign of good differentiation.
RULE: A large minority of patients with follicular lymphomas eventually get a high-grade B-cell
lymphoma ("diffuse large-cell" or "immunoblastic") that is rapidly fatal. (As noted above, other
nodular lymphomas simply turn into their more aggressive diffuse counterparts.)
* Future pathologists: If you happen to find a node in which this transformation is actually happening,
you've found a "composite lymphoma". All about this: Am. J. Clin. Path. 99: 445, 1993;
Am. J. Path. 154: 1857, 1999.
* RULE: Most nodular lymphomas of all kinds feature one of two characteristic translocations, either
t(11;14) or t(14;18). Each involves the immunoglobulin heavy-chain region on chromosome 14. This
is brought into contiguity either with the bcl1 / PRAD / cyclin D1 oncogene on chromosome 11 or the
bcl-2 oncogene on chromosome 18.
bcl-2 produces a protein on the inside of mitochondria that prevents the cell from
undergoing apoptosis.
* The biggest news in lymphoma recently is obtaining molecular remissions
(i.e., none of the 14;18 left on PCR) using a combination of a tumor
vaccine and colony stimulating factors, following chemotherapy:
Nat. Med. 5: 1124, 1999.
* RULE: Some of the T-cell lymphomas excite the local histiocytes and turn them into granulomas. This
doesn't mean much.
RULE: Small lymphocytic lymphoma ("well-differentiated lymphocytic lymphoma", "the solid phase
of chronic lymphocytic leukemia"), in which the cells perfectly resemble normal lymphocytes, is always
diffuse, never nodular.
RULE: The histologic type of a lymphoma is much more important than its stage in determining
prognosis. (This is the exact opposite of Hodgkin's disease.)
RULE: Large, polyclonal, benign proliferations of lymphocytes may occur anywhere there is lymphoid
tissue, and have earned the dubious name pseudolymphoma. Distinguishing these from real lymphomas
is a challenge.
Also remember that certain autoimmune diseases feature heavy polyclonal lymphoid infiltration of
salivary glands (Sjogren's), thyroid (Hashimoto's), islets (type I diabetes), or kidneys (autoimmune
interstitial nephritis).
&*nbsp;For some reason, Lyme disease produces pseudolymphomas in the ear lobes. No one has a clue why.
RULE: Pathologists trying to distinguish malignant lymphomas from benign lymph node hyperplasias
and pseudolymphomas pay special attention to:
(1) Effacement of the normal lymph node architecture;
(2) Cell uniformity ("monotony", suggests lymphoma, but even follicular lymphomas are infiltrated by
the same benign cells as grow in a germinal center);
* (3) Presence of macrophages laden with nuclear debris (tingible body macrophages, a sign that the
process is either benign or a high-grade lymphoma, because in low-grade
lymphomas you won't see much apoptosis);
* (4) Widespread bcl-2 protein staining is a pretty good sign that
this is lymphoma.
* (4) Vascular proliferation (new vessels suggest the process is benign), and;
(5) Invasion of surrounding tissue ("capsular transgression",
suggests lymphoma).
(6) Necrosis (apart from apoptosis)
is common in some lymphomas, and of course in necrotizing infections, but uncommon in
difficult benign lesions.
(7) If "follicles"/"nodules" are present, the absence of a mantle
of small lymphocytes around the light side of the follicle suggests
malignancy.
(8) Today, most pathologists ask for immunotyping; monoclonality for kappa or lambda indicates B-cell
lymphoma.
(9) Today's pathologist, asking "Is this lymphoma?", begins as follows:
If it is apparently made of large lymphoid cells, the pathologist will order a CD45
(leukocyte common antigen, positive in lymphomas), a few other lymphocyte markers,
cytokeratins (negative in lymphomas),
and a few melanoma markers (negative in lymphomas).
(9) We also want DNA studies for the typical gene rearrangements (immunoglobulin genes for B-cell
lymphomas, T-cell receptor genes for T-cell lymphomas), both for diagnosis and to look for residual
disease. (All about gene rearrangements in lymphomas and leukemias: Am. J. Clin. Path. 95: 347,
1991. * WARNING: Some high-grade lymphomas are still "null-genotype": Cancer 67: 603, 1991).
{09040} electron micrograph of a malignant lymphoid cell. Note the lack of distinguishing features.
* RULE: Lymphomas in the liver generally center on the portal areas. This also applies to Hodgkin's
disease.
RULE: Most lymphomas (Hodgkin's and non-Hodgkin's) may cause generalized dysfunction of benign
B-cells (hypogammaglobulinemia), with resulting tendency to infection.
Classification schemes:
Anyone using the terms "lymphosarcoma", "giant follicular lymphoma", or "reticulum cell sarcoma"
in today's medicine is terribly out of date.
The 1966 Rappaport classification is archaic but still popular. It was based on certain incorrect (but
once-useful) assumptions about the nature of the cells seen in these lesions:
"Well-differentiated lymphocyte"...
looks like a normal resting lymphocyte
"Poorly-differentiated lymphocyte"...
doesn't look like a normal resting lymphocyte, but is smaller than an endothelial cell
"Histiocyte"...
bigger than an endothelial cell, and has lots of cytoplasm
"Undifferentiated cell"...
bigger than an endothelial cell, and has only a little cytoplasm
Lymphomas were further sub-divided into "nodular" and "diffuse", depending on their growth pattern.
Despite its limitations, the Rappaport system was useful as lymphomas were being sorted out.
* The 1974 Lukes-Collins classification was based on immunotyping, rather than morphology, of cells.
Activated-type B-cells from small-cleaved through large-noncleaved cells were appropriately called
"follicular center cells".
The 1982 Working Formulation
was a consensus of experts based only on
morphology. It worked nicely until it was
superseded by the Revised European-American system.
You'll still find people using these terms.
Low grade lymphomas (survival around 10 years)
Small lymphocytic
Small lymphocytic, plasmacytoid
Follicular, small cleaved cell
Follicular, mixed small-cleaved and large cell
Intermediate grade lymphomas (survival around 5 years)
Follicular, large cell
Diffuse, small cleaved cell
Diffuse, mixed small-cleaved and large cell
Diffuse, large cell
High grade (quick death, but try for a chemotherapy cure;
disease-free for 2 years usually means cured)
Large-cell immunoblastic (B- or T-cell)
T-Lymphoblastic
Small noncleaved cell (Burkitt's, etc.)
Miscellaneous
Mycosis fungoides / Sézary syndrome
Adult T-cell leukemia/lymphoma with HTLV-1
I would ask you NOT to worry about differentiation markers
beyond what's been listed above.
It also includes the leukemias, and "Big Robbins" now follows
the current tendency to study lymphoid leukemias and lymphocytic lymphomas
together.
Precursor B-cell neoplasms
Precursor T-cell neoplasms
Peripheral B-cell neoplasms
Peripheral T-cell and natural killer neoplasms
Here are the common ones:
Small lymphocytic lymphoma ("well-differentiated lymphocytic lymphoma", "the solid phase of chronic
lymphocytic leukemia")
This B-cell lymphoma is composed of cells that look like never-stimulated, resting lymphocytes, of the
sort seen adjacent to germinal centers. They look normal but don't work. (* Maybe this is why this
lymphoma never forms nodules.)
{23575} small lymphocytic lymphoma. There is a small vessel running across the picture. Use the
endothelial cell nuclei to gauge the sizes of cells.
The bone marrow is always involved at the time of diagnosis, and if the cells spill into the bloodstream,
"chronic lymphocytic leukemia" is said to be present. See below.
Patients are generally older adults. Despite systemic involvement, the disease progresses very slowly,
and seldom kills.
Around 30% of these patients eventually develop a more aggressive B-cell lymphoma (including
1% who get a very aggressive one, i.e., Richter's
syndrome), as in CLL.
{23854} CLL, transforming into a more
aggressive cancer. Note the numerous small lymphocytes and the blasts.
Plasmacytoid small lymphocytic lymphoma, features cells with slightly more abundant, purple
cytoplasm and production of monoclonal paraproteins. As a rule, these diseases are somewhat more
aggressive than generic small cell lymphocytic lymphoma, and they usually produce a paraprotein.
Waldenstrom's macroglobulinemia produces large amounts of IgM pentamers. In addition to the
problems seen in any lymphoma, patients suffer with hyperviscosity syndrome (dizziness, eye problems,
other problems; look for "sausage link" retinal veins). Like "regular small lymphocytic lymphoma",
This is a disease of the elderly.
* Future pathologists: Look in the nuclei for "Dutcher bodies", masses of IgM (similar to the familiar "Russell
bodies", but in the nucleus). These let you be confident
that you're looking at lymphoma. Transformation
into a more aggressive
cancer can supervene as in the more familiar small
lymphocytic lymphoma.
* New suggested criteria for Waldenstrom's: Am. J. Clin. Path. 116: 420, 2001.
Alpha heavy-chain disease typically affects the small bowel and is fairly common in the Near-East.
Most victims are young adults, who present with malabsorption.
{13673} heavy chain disease; plasmacytoid cells in intestinal mucosa
* This transforms into the aggressive "Mediterranean abdominal lymphoma", a B-cell immunoblastic
lymphoma.
{19504} Mediterranean lymphoma, small bowel
Gamma heavy-chain disease is a marker for a more aggressive lymphoma that
generally affects the
elderly. Look for big tonsils.
Mu heavy-chain disease generally turns leukemic early.
Mantle cell lymphoma (Hum. Path. 31: 7, 2002)
It's a disease of older men, and often arises extranodally.
It grows wrapped around normal germinal centers.
MALT lymphoma (on mucosal surfaces, of course) features a trademark
translocation t(11;18) and fusion protein (API2/MALT1; AM. J. Path. 162: 1113, 2003). Remember that helicobacter
infection is the one known cause of this cancer in the stomach (Blood 102: 1012, 2003); if the mutation
is present, the lymphoid proliferation will not go away even if you get rid of the
helicobacter (Gastroenterology 122: 1286, 2002), but helicobacter elimination
is still the mainstay of treatment (Cancer 104: 532, 2005).
Marginal cell lymphoma (Am. J. Clin. Path. 117: 698, 2002)
* Trisomy 18, cited in "Big Robbins" as characteristic, is actually
present only in a minority of these tumors (Blood 88:
751, 1996).
Follicular lymphoma
Formerly divided into "small-cleaved", "mixed small-cleaved
and large cell" and "large-cell" subcategories,
it's now pretty clear that most of them are mixed.
The "small cells"
look like normal lymphocytes except
for one or more clefts up the nucleus ("buttock cell", etc.),
and they lack the marbly heterochromatin.
The "large cells" can be cleaved or noncleaved.
Both kind of cells are "centrocytes", since you find them in
the active regions of germinal centers.
Patients are usually older adults. The bone marrow is usually involved at the time of diagnosis.
The translocation t(14;18), with bcl2, is usual.
About half of these transform into a diffuse B-cell lymphoma.
{23599} mixed lymphoma; use the endothelial cell at 2:30 as a size marker
{23596} nodular large-cell; at this power, just appreciate the nodularity
Note that even large-cleaved lymphocytes are larger than endothelial cells.
Diffuse small cleaved lymphoma
A common, more aggressive counterpart of follicular small-cleaved B-cell lymphoma.
{23590} diffuse small cleaved lymphoma (all
you can tell is that it is small cleaved)
{23581} nodular lymphoma
Diffuse large-cell lymphoma
This is several diseases, B-cell (more aggressive than its follicular counterpart; * many are now known to
have the same myc translocations as Burkitt's; genes updated Blood 106: 114, 2005), and the slightly less-common (* "post-thymic") T-cell
lymphoma.
* Anaplastic large T-cell lymphoma is rather less aggressive
than the other large ones; it features
t(2;5) with production of a fusion product oncogene (NPM/ALK, Blood 93:
3088 & 3913, 1999) and is now called "ALK+".
So far, the new biotech therapies don't seem to help for the T-cell
lymphomas: Cancer 103: 2091, 2005.
{08787} large-cell lymphoma
Results with chemotherapy are quite good, with a majority of patients apparently cured (Blood 77: 942,
1991).
* These diseases may be indistinguishable histologically from the rare true histiocytic lymphoma (an
oxymoron; histiocytes are not lymphocytes). Never mind.
{23674} true histiocytic lymphoma, trust me
Large B-cell Lymphoma
These lymphomas, composed of huge cells with big centrally-located nucleoli and turned-on nuclei, may
be of B-cell (the majority). The cells may resemble normal immunoblasts,
or be bizarre
in other ways.
{00245} immunoblastic lymphoma
Noted subcategories of "large B-cell lymphoma"...
{10935} lymphoma arising in thyroid; my case
Unlike most lymphomas, these tumors often arise extranodally, and rapidly spread to many different
organs.
{08017} lymphoma in the heart
These tumors are aggressive, but chemotherapy can be curative. * Elaborate subclassification schemes
exist; their usefulness remains speculative.
T-Lymphoblastic lymphoma
This is the most important pediatric lymphoma (typically a teenaged's guy's disease); it is the solid
counterpart to T-cell acute lymphoblastic leukemia.
* These smallish T-cells have convoluted (i.e., more than one cleft) nuclei, though they are not as
complex as in Sézary syndrome (below). Immunologists note similarities with baby, intra-thymic T-cells.
* The usual t(14;21) and its molecular biology: Proc. Nat.
Acad. Sci. 97: 3497, 2000.
In keeping with its thymocyte origin, it typically presents itself in the anterior mediastinum (i.e., thymus
area).
The prognosis has historically been not-so-good. Try a new chemotherapy protocol.
{00242} T-lymphoblastic lymphoma. Trust me.
Burkitt's lymphoma ("small non-cleaved cell lymphoma", * one of Rappaport's "undifferentiated
lymphomas")
A famous B-cell tumor endemic in children in the African malaria belt. Most often, the African variant
arises in the jaw.
{46189} African Burkitt's
The Epstein-Barr virus is part of the cause, but obviously not the whole story. These tumors also have
a famous translocation that places the oncogene myc on chromosome 8 under the control of the
IgH regulator on chromosome 14. (* Less often, myc joins the kappa chain gene on
2, or lambda on 22).
NOTE: We've already seen that many lymphomas in immunosuppressed patients, both inside and
outside the CNS, are strongly linked to the Epstein-Barr virus. For an update, see Cancer 67: 444 &
536, 1991; Cancer 68: 1285, 1991. Nowadays we call these
"post-transplantation lymphoproliferative disorders", and they tend to
regress if immunosuppression can be discontinued.
The lymphoma cells are strikingly uniform, with big blue nuclei, and deep blue cytoplasm laden with
lipid droplets. Tingible body macrophages loaded with this lipid appear as white "stars" against the blue
"sky".
The "starry sky" appearance of Burkitt's is a favorite exam question. Just to confuse you, tingible body
macrophages appear as similar "stars" against the paler "sky" of a normal lymph node.
Despite "Big Robbins", the stars of Burkitt's are more conspicuous than other
tingible-body macrophages because
they are heavily laden with lipid.
{46326} African Burkitt's, tonsils
African Burkitt's is generally curable with chemotherapy, if you can get it to the victims.
By contrast, American Burkitt's, a sporadic disease of young people not related (?) to Epstein-Barr
virus, can produce masses most anywhere, and has a worse prognosis.
* A Burkitt's-like lymphoma is also common in AIDS, and is less lethal than other AIDS-associated
lymphomas: Eur. J. Haem. 76: 506, 1991.
* A non-Burkitt's small non-cleaved lymphoma occurs in young adults, with more variable cells and
poorly-understood natural history.
Mycosis fungoides / Sézary syndrome
Lymphomas of the epidermis and upper dermis, composed of large T4-cells with very elaborately
infolded ("cerebriform") nuclear membranes. The distinctive "Pautrier microabscesses" (misnamed)
are clusters of these T-cells within the epidermis.
In "mycosis fungoides" (Latin for "Toadstools! Toadstools!"), patients suffer from red, peeling skin for
some years, then enter a plaque and eventually a tumor phase, in which the patient looks horrible and
has lymphoma throughout the body.
{40003} mycosis fungoides
In "Sézary syndrome", the red skin does not transform into tumors. Instead, the cells circulate in the
blood as a leukemia. The disease is slowly progressive, and survival for many years is usual.
* To tell mycosis fungoides from HTLV-I leukemia on skin biopsy, you need to use a probe for the
virus: Am. J. Path. 144: 15, 1994.
{12757} Sézary patient
Adult T-cell leukemia-lymphoma
A rare, very aggressive malignancy of T-helper cells.
It is strongly linked to the HTLV-I retrovirus, which is transmitted like AIDS, binds to the same
receptor (CD4), is neurotrophic, and lies dormant for a long time. (All about
HTLV-1: Lancet 353: 1951, 1999).
We now check all donor blood for this virus.
* The malignancy is preceded by polyclonal T-cell hyperplasia, due to induction of T-cell IL-2 receptors
by the virus.
* For some obscure reason hypercalcemia is common in this disease.
The disease (like the virus) is more common in Japan and the Caribbean. HTLV-I in Japan: Lancet
343: 213, 1994.
* Darwin's world. HTLV-I is as old as the great human migrations of the stone age. See Proc. Nat.
Acad. Sci. 91: 1124, 1994.
* Malignant histiocytosis ("histiocytic medullary reticulosis"), a very aggressive, fortunately rare cancer
of blood-cell-eating macrophages, is worth mentioning here. So is the dread hemophagocytic lymphohistiocytosis,
a sometimes-genetic (often perforin), sometimes-acquired (viral-triggered?) illness.
{23668} malignant histiocytosis with erythrophagocytosis
* KSHV is responsible for the effusions-but-nothing-solid lymphomas of AIDS
(inclusions: Arch. Path. Lab. Med. 123: 257, 1999).
HODGKIN'S DISEASE ("Hodgkin's lymphoma"; NEJM 326: 678, 1992; Cancer 75(S1): 357, 1995)
A common (7500 cases/year in the U.S.), generally curable cancer that typically affects young adults.
(There is a second peak in older adults; their disease tends to be more aggressive.)
Risk factors are ill-defined, and "epidemics" could perhaps be statistical accidents. Family members
are at several times increased risk, and a monozygous twin is at 100 times the base risk (NEJM 332:
413, 1995).
A previous history of Epstein-Barr infectious mononucleosis supposedly triples one's risk for Hodgkin's
disease. Epstein-Barr virus RNA transcripts are present in the
malignant cells in many (but by no means most!) cases of Hodgkin's disease. See NEJM 320: 502, 529
& 689, 1989; Blood 77: 1781, 1991; the gene is * EBNA-1: Blood 94:
244, 1999.
* I remain very skeptical. For example, the T-cells in Hodgkin's tissue are a very heterogeneous lot, not
the oligoclonal populations we'd expect if they were fighting a virus (Am. J. Clin. Path. 101: 76, 1994;
more doubts Am. J. Clin. Path. 99: 604, 1993). Stay tuned on this to see how it comes out.
It is most plausible that the cell of origin of the Reed-Sternberg cell is the Reed-Sternberg-like cell seen
in infectious mononucleosis tissues. I'm not the only one who thinks this (Am. J. Path. 146: 379, 1995).
* Hodgkin's disease is rare in the Orient. For some reason, pediatric Hodgkin's is common in the
poor nations.
* A genetic basis for early-onset Hodgkin's, interacting with environmental stuff: NEJM 332: 413, 1995.
* Hodgkin's disease is being recognized more and more as a complication of AIDS. Not surprisingly,
AIDS patients with Hodgkin's disease tend to lack lymphocytes (Cancer 67: 1865, 1991).
The malignant cell is the Reed-Sternberg cell, but until the late stages of the disease, the tumor masses
are composed primarily of inflammatory cells responding to the cancer.
{23560} Reed-Sternberg cell
Everybody accepts the 1965 Rye Classification of Hodgkin's disease.
Lymphocyte predominance: A background of normal, monotonous, small lymphocytes, * often with
histiocytes.
{46338} Lymphocyte predominance Hodgkin's
Reed-Sternberg cells of any kind may be rare! See NEJM 319: 246, 1988.
This variant generally announces itself in a single group of nodes, and almost all patients get cured by
today's therapies.
In the "nodular" type, the RS cells don't even immunostain like in other forms of Hodgkin's (they
are CD15-,
CD45+, B-cell markers are positive), and it's
probably "not really Hodgkin's, maybe a dysplasia":
Blood
87: 2428, 1996;
Am. J. Path. 146: 812, 1995; different mutations Blood 101: 706, 2003.
The main reason to "type" Hodgkin's is to rule this in or out.
Don't diagnose "chronic lymphocytic leukemia" or "small lymphocytic lymphoma" in a young person
until you've sectioned through the block in your search for the diagnostic cell.
Mixed cellularity: There are many Reed-Sternberg cells and variants, in a background of lymphocytes,
plasma cells, eosinophils, and histiocytes. This variant can present at any stage.
{23539} mixed cellularity Hodgkin's disease
* Lymphocyte depletion: Mostly cancer cells, little else.
I believe this is a B-cell lymphoma superimposed on or arising from the same
soil as the Hodgkin's disease.
* The background may be lots of poorly-woven collagen ("diffuse fibrosis variant") or just reticulin
("reticular variant"), with wildly anaplastic cells.
The disease often (but not always) presents at late stage.
Future pathologists: You won't make this diagnosis unless there's a recognizable Reed-Sternberg cell
or a previous diagnosis of Hodgkin's disease.
{23524} lymphocyte depleted Hodgkin's disease. Just plain anaplastic.
Nodular sclerosis: This features lacunar Reed-Sternberg variants and a tendency for the lesion to
become crisscrossed by dense collagen bands. The prognosis is generally good.
{23542} nodular sclerosing Hodgkin's disease
NOTE: There are subtypes of each common type....
Sex ratios: Nodular sclerosis is a bit more common in women. All the other forms are more common
in men.
Having described this elegant classification scheme, I am almost sorry to have to add that the prognosis
for any particular case of Hodgkin's disease is determined by stage, rather than by type. Almost all
patients with stage I or IIA disease are now cured. This drops to around 50% for patients presenting
at stage IV.
Lymphocyte predominance presents at low stage, mixed cellularity at low or high stage, lymphocyte
depletion presents at high stage, and nodular sclerosis is often a mediastinal mass. These differences
account for "different prognosis for different Hodgkin's types".
Reed-Sternberg variants are also malignant.
Mononuclear Reed-Sternberg-like cells
("Hodgkin cells")
have single-lobed nuclei and one nucleolus. They may be seen
in any variant of Hodgkin's disease.
* LP cells (* "L&H cells") have scanty cytoplasm, big knobby nuclei, and small nucleoli. They are seen in lymphocyte
predominance Hodgkin's disease.
Lacunar Reed-Sternberg cells have abundant, pale cytoplasm (* an artifact of formalin fixation). They
are seen in nodular sclerosis Hodgkin's disease.
Polylobated Reed-Sternberg cells ("popcorn cells") look like good Reed-Sternberg cells, except that the
nucleoli aren't so impressive. They are typical of mixed cellularity Hodgkin's disease.
* Pleomorphic Reed-Sternberg cells are
anaplastic versions of the familiar form. They make up the bulk
of the tumor in lymphocyte depletion Hodgkin's disease, if you
believe in this entity.
Reed-Sternberg cell rules:
While a classic Reed-Sternberg-like cell may appear in other diseases (even "infectious mono"), its
presence in the proper background (see below) gives the diagnosis of Hodgkin's disease.
You must see a classic Reed-Sternberg cell before making the diagnosis.
Hodgkin's begins as an enlarged node or group of nodes. * While we do not test you on staging,
everybody knows these basics:
Stage I... one node group or organ
Stage II... one side of the diaphragm
Stage III... both sides of the diaphragm
Stage IV...marrow, or two extra-lymphatic organs
"A" means no systemic symptoms
"B" means fever, weight loss (>10%), or night-sweats.
* The classic Hodgkin's fever is the "Pel-Ebstein", or intermittent spiking fever.
{20056} Hodgkin's disease in a cervical node (we
would of course diagnose this only with microscopy)
Hodgkin's disease spreads predictably along contiguous groups of lymph nodes.
As it spreads, there may be transformation: Lymphocyte predominance turns into mixed cellularity or lymphocyte depletion.
Mixed cellularity turns into lymphocyte depletion.
Nodular sclerosis generally keeps its type.
Minor mysteries of medicine:
(1) Hodgkin's patients often notice pain at sites of disease after they drink alcohol.
(2) Hodgkin's patients often have cutaneous anergy, even early in their disease.
Hodgkin's therapy today includes heavy-duty chemotherapy and re-infusion of the patient's own, purged
bone marrow (Lancet 341: 1051, 1993).
INTRODUCING THE LEUKEMIAS
Leukemia ("white blood"), discovered by * Virchow, is a generic term for replacement of the bone
marrow by cancerous blood cells. These usually (but not always; many acute leukemias are initially
"aleukemic") are spilling over into the bloodstream; in any case, expect a "packed marrow" except in
early CLL.
{23848} packed marrow; * this was late-stage CLL
* The genetic-chromosomal mysteries of the leukemias have yielded up their secrets faster than any other
cancer. If you like this sort of thing, see NEJM 330: 328, 1994.
Acute leukemias ("poorly differentiated leukemias") are overgrowths of cells
that fail to mature (blast
cells). These diseases are very aggressive, and cause death in weeks or months.
{16243} blast with Auer rods
How to spot a blast: (review from "Histology")
Future pathologists: You cannot tell whether a generic, undifferentiated "blast cell" is lymphoid or
myeloid without doing special stains noted above. You'll learn below that Auer rods are sure markers
for myeloid differentiation.
These cells are not especially fast-growing, but they fail to mature. Even if they do not "crowd out"
their healthy neighbors, they tend to inhibit normal production of other blood cells.
Acute leukemia presents abruptly as one of the cytopenias (anemia, neutropenia, and/or
thrombocytopenia). Bone pain is likely to result from expansion of the marrow and infiltration of the
periosteum.
Later, involvement of other organs is common. Brain involvement is especially troublesome. T-cell
leukemias often produce a mass in the anterior mediastinum (why?).
{23842} acute lymphocytic leukemia, brain
Death typically results from hemorrhage (cerebral, GI, other), and/or infection (neutropenia,
chemotherapy), and/or complications of bone marrow transplantation.
{06269} fatal cerebral hemorrhage in leukemia
The biology of the acute leukemias is very well-studied (Lancet 349: 118, 1997). The refractory ones
have pumps to remove chemotherapy drugs, etc., etc.
By contrast, chronic leukemias ("well-differentiated leukemias") feature cancer cells
that do mature
(more or less), and which have a natural history measured in years.
Like acute leukemia patients, these patients may present with a cytopenia problem. Or they may have
problems from a high white ("leukostasis" plugging small vessels), or may notice lymphadenopathy or
organomegaly, or the high white count may be an incidental finding on "routine lab".
RULE: Marrow cells (most leukemias, extramedullary hematopoiesis) in the spleen involve the red
pulp. Lymphomas in the spleen (at least the B-cell type) involve the white pulp.
RULE: Any leukemia can involve the lymph nodes and make them large, but the enlargement is seldom
so spectacular as in Hodgkin's or non-Hodgkin's lymphoma.
RULE: Any leukemia (or lymphoma) can involve the liver, but enlargement is usually not spectacular.
Hodgkin's and non-Hodgkin's lymphomas will first appear in the portal areas.
Lymphocytic leukemias recall the various kinds of normal lymphocytes, and myeloid ("myelogenous",
or better, "granulocytic") leukemias recall a normal granulocyte.
You remember that myelocytes, the precursors of granulocytes, are the most common cell in normal
bone marrow (myelo-); hence their name.
Cell turnover in the leukemias (and the closely-related polycythemia vera and agnogenic myeloid
metaplasia) is much increased, placing these patients at risk for gout. The risk increases further when
cancer cells are dying by the pound during therapy. The thoughtful oncologist gives prophylactic
medication.
ACUTE LYMPHOBLASTIC LEUKEMIA ("ALL"; diagnosis Am. J. Clin. Path. 111:
467, 1999)
This is the familiar "childhood leukemia", with peak age in four year old kids. Adult ALL is less
common.
{12410} ALL (all you can tell from the smear is "blasts")
ALL seems to strike at random. Radiation exposure is a known risk factor, Down's syndrome kids are
at 15x the normal risk, a patient's identical twin has a 20% risk, and * whites are affected at double the
rates of nonwhites.
* A curious claim that could be true is the idea that leukemia is an unusual response to one
or more as-yet-unidentified viruses met at the wrong age; one finding that seems to be robust is a
strong correlation between leukemia rates and the diversity of origins, i.e., new immigrants, in an area
(Br. Med. J. 313: 1297, 1996; Lancet 349: 344, 1997.)
* Among the most influential and egregious
cases of lying with statistics was
the claim, in a certain hugely-influential and still-acclaimed book,
that pesticides
had caused an epidemic of childhood leukemia. The evidence? During the late 1940's and the 1950's,
pesticide use became widespread, and at the same time, the number of cases
of childhood leukemia,
and the percentage of childhood deaths due to
leukemia, increased strikingly. Most of the increase in the number of cases
was due to the baby boom (a fact that the author did not point out.)
And of course,
the real explanation
(which again
the author didn't tell the readers)
for the increased percentage of deaths due to leukemia
was the introduction of antibiotics, which cut the number of fatal infections so dramatically. Whether
there was an increase due to pollution and/or nuclear testing is unclear, but if there was any change in
the true incidence of leukemia during those times, it was hardly dramatic.
I do not know whether this was done deliberately or thoughtlessly,
But you'll run into this fallacy
from bunko-science proponents (left-wing, right-wing) many times.
I propose that it be named for this author.
Your lecturer is concerned about the environment, and thinks
that telling the truth is best.
* Pathologists and oncologists have subclassified acute lymphoblastic leukemia by blast morphology
("FAB classification"; stands for "French-American-British"):
L1: 85%...
Cells <= 2x the diameter of a normal lymphocyte; smooth nuclei; more common in kids
L2: 14%...
Bigger cells, lots of clefts, often nucleoli; more common in adults
L3: 1%...
Even bigger cells, Liquid Burkitt's lymphoma; t(8;14) and everything
{23746} L1
L3 is a distinct entity, but L1 and L2
aren't especially useful. Most people prefer the immunologic classification:
B-cell... 80%... * CD19+...* several subclasses exist
T-cell... 15%... * "intra-thymic markers, like T-lymphoblastic lymphoma"; chances of a cure are much less than with
B-cell disease
Nothing...less than 5%...* markers are negative; there is only HLA-DR.
Apart from the fact that all L3's (Burkitt's) are B-cell tumors, there is little correlation between the two
systems.
* More for subclassifiers:
Hyperdiploidy (>50 chromosomes), present in a large minority of B-cell ALL's, confers a good
prognosis.
* The translocation t(12;21) brings the AML1 and TEL genes together.
* The translocation t(1;19), also present in a large minority of B-cell ALL, gives a bad prognosis (review:
Blood 77: 324, 1991).
* The translocation t(5;14), a marker for pre-B leukemia, scrambles interleukin 3.
Adults with ALL are often "Philadelphia-positive", and kids can be, too (* the latter
confers a bad prognosis: NEJM 342: 998, 2000).
The break-point in bcr is different in ALL and CML (Blood 77: 324, 1991). * In adults or children,
this gives a bad prognosis (Blood 77: 435, 1991), especially if combined with monosomy 7 (Blood 77:
1050, 1991). An older review of the Philadelphia chromosome and its variants: NEJM 319: 990, 1988.
Myeloid antigen expression (see the reference) imparts a bad prognosis for both B-cell and T-cell acute
leukemia (NEJM 324: 800, 1991).
Almost all children with ALL get a complete remission on current therapy. The majority (71% reported
in 1993) now get apparent cures.
The prognosis for adults is still not so good.
* All about the treatment of ALL: NEJM 329: 1289, 1993. The big deal for those who don't get cured
is super-heavy-duty chemotherapy followed by autologous bone marrow infusion; the results are dismal,
and the whole story reads like "the case for unjustifiable cancer therapy" or "the law of inverse care":
Lancet 346: 873, 1995.
* One piece of surprising news is that the large majority of T- and B-cell ALL's have rearrangements of
the T-cell receptor -chain gene (Blood 77: 141, 1991). Stay tuned on this one.
{23857} ALL in the liver
* Coby Howard, who had ALL and a relapse, didn't get his bone marrow transplant because of Oregon's
health-care rationing, which spent the money where it was most likely to do the most good. Some of
the pressure groups (liberal, conservative), of course, had a field-day with Coby's death. Remember
Coby's name, and the principle.
ACUTE MYELOBLASTIC LEUKEMIA ("AML", "poorly differentiated granulocytic leukemia",
"acute non-lymphocytic leukemia", "ANLL", etc.)
This is the common acute leukemia of adults (seldom over age 40, occasionally children are affected).
Although most cases are idiopathic, many things are known to increase risk. These include:
The cancer arises out of a background of mutated marrow cells that typically include granulocytic
and other (erythroid and/or monocyte precursors). All are likely to show some abnormalities (* good
tipoff: megakaryocytes with non-lobulated nuclei).
The FAB classification (Ann. Int. Med. 103: 614 & 620, 1985) is worth knowing at the recognition
level (though it is of little interest to practicing oncologists, who are today much more concerned about
the molecular lesions):
M0: undifferentiated myeloblasts without myeloperoxidase (* new criteria Am. J. Clin. Path. 115: 876, 2001)
M1: undifferentiated myeloblasts with myeloperoxidase
M2: some promyelocytic differentiation, maybe a few Auer rods; * t(8;21) is distinctive (newly-discovered gene on 21 named
AML1: Proc. Nat. Acad. Sci. 88: 10413, 1991; see this article for
information about other translocations)
M3: very granular promyelocytes, often many Auer rods, DIC
(* from annexin II on the surfaces that activates plasmin:
NEJM 340: 944, 1999); * t(15;17)
and * t(11;17) are distinctive, and (KNOW:)
involve the vitamin A receptor (Blood 77: 1418 & 1657,
1991; Proc. Nat. Acad. Sci. 91: 1178, 1994).
All-trans retinoic acid
(* "tretinoin") matures these cells: NEJM 324: 1385, 1991;
NEJM 27: 385, 1992;
Blood 85: 2643, 1995; Blood 94: 39, 1999
(* discovered by the Red Chinese, who attributed their success to lack of
regulation of human research.... Do any of you "ethicists" want to "refuse to use this data which was
acquired immorally"?)
* Retinoic acid plus G-CSF for the difficult t(11;17) subtype:
Blood 94: 39, 1999.
Diagnostic stain Blood 86: 862, 1995.
M4: myeloid and monocytic differentiation
M5: monocytic differentiation only; * t(9;11)(p22;q23); 9p22 is beta-interferon receptor, while 11q23
is the nearly-characterized MLL
(myeloid-lymphoid leukemia gene; common
in infant and adult leukemias, though not childhood leukemias
(Proc. Nat. Acad. Sci. 88: 10735,
1991; Blood 94: 283, 1999)
* Fun to know: MLL also forms a fusion product with MEN-1 (which
is adjacent) and a src-like gene on chromosome 19 (Proc. Nat. Acad.
Sci. 94: 2563, 1999) in t(11;19)
leukemias; this fusion product inhibits p53's product (Blood 93:
3216, 1999).
M6: features of red cell precursors predominate; "Di Guglielmo's erythroleukemia" (* future
pathologists: look for d-PAS-positive chunks in the cytoplasm)
M7: platelet markers; acute marrow fibrosis (* PDGF effect; reticulin)
We distinguish these leukemias from one another, and from ALL, by morphology and by the stains
listed earlier in the unit. Auer rods are red-staining, rod-shaped crystalloids made of primary granules.
If present, they prove that a blast is "myeloid" and not "lymphoid".
{12338} AML. Note promyelocyte in center.
* There are many sub-variants with distinctive genetic fingerprints and oncoprotein and so forth, which
impart good or bad prognosis with chemotherapy (for example, Proc. Nat. Acad. Sci. 90: 5484 & 7884,
1993). Don't worry about these.
Today, a majority of AML patients succeed in a buying a year or so of life with chemotherapy. There
is talk of cures in around 10% of cases.
THE MYELODYSPLASTIC SYNDROMES ("THE PRELEUKEMIAS", Carl Sagan's disease):
Mayo Clin. Proc. 70: 673,
1995; Am. J. Clin. Path. 119(S1): S-58, 2003.
This is a family of disorders in which there are problems in producing red cells, granulocytes, and
platelets. What has happened is that the normal precursor cell that gives rise to all three has been
replaced by a mutant clone.
* t(3;5), nucleophosmin and other newly-discovered genes: Am.
J. Path. 155: 53, 1999.
* Isochromosome 17q, still mysterious, is a
common lone abnormality (Blood 94: 225, 1999); my late mother,
who received radiation as a child for osteomyelitis, had this
signature;
this is also the most common known hit in CML's progression to
blast crisis.
* Subclassification is useful. The old FAB classification:
1. Refractory anemia (poor hemoglobinization, too few red cells)
2. Refractory anemia with ringed sideroblasts (>15% of nucleated red cells)
3. Refractory anemia with excess blasts (5-20% myeloblasts)
4. Refractory anemia with excess blasts in transformation (20-30% myeloblasts)
5. Chronic myelocytic leukemia
Ask your hematologist what this all means. If you are really gung-ho,
there's an easier system in Blood 89: 2079, 1997.
Most patients are older adults, who sometimes are symptomatic. In the more aggressive forms, death
follows in a few years. Often these patients are asymptomatic, and the problem is detected on routine
screening.
As you would expect, this disease pattern has a propensity to transform into acute myelogenous
leukemia, and does so in a large minority of cases.
CHRONIC MYELOID LEUKEMIA ("chronic myelogenous leukemia", "well-differentiated
granulocytic leukemia"): all about it Am. J. Med. 100: 555, 1996.
Ann. Int. Med. 131: 207, 1999.
This is cancer of the myeloid stem cells in which there is overgrowth of normally-maturing myeloid cells
Radiation and exposure to chemicals (notably benzene) are known risk factors. Most of the time, the
disease seems to strike at random.
Patients typically have high counts of neutrophils and their precursors (and almost always basophils).
These are normal (functionally and morphologically) for all intents and purposes, except that for some
reason they lack cytoplasmic alkaline phosphatase.
Preposterously high white counts (>100,000 or so) are likely to result in white cells plugging important
small vessels ("leukostatic ischemia" of the brain, etc.)
While the spleen is likely to be enlarged in all the common leukemias, chronic myeloid leukemia
typically produces huge spleens (down almost to the pubic hair). * There will usually be some little
infarcts.
Occasional CML cases have predominance of basophils (itchy) or eosinophils. * Serum vitamin B12 is
likely to be elevated due to elevation of its binding protein; this can happen in other myeloproliferative
disorders.
{10769} CML, splenomegaly
Both granulocytic series and "benign" monocytes and erythroid precursors bear the distinctive
Philadelphia chromosome, a translocation between chromosomes 9 and 22. This produces a new gene
(bcr/c-abl) which is a potent oncogene. Even "Philadelphia negative" cases have this new gene.
{12371} Philadelphia chromosome
* Molecular biologists: It's now clear that the bcr product, long a mystery, modulates GTPase activity
by a ras product homolog (Nature 351: 400, 1991).
* The new gene was the first target of a successful anti-sense cancer therapy (Proc. Nat. Acad. Sci. 91:
4504, 1994).
The disease eventuates, after a few years, in blast crisis, with or without (50%/50%) a previous
accelerated phase. Blasts appear in the circulation in large numbers, and death follows quickly as they
overwhelm the marrow and body. This is not very treatable.
{23869} CML, blast crisis
Traditional chemotherapy with busulfan or hydroxyurea
controls symptoms during the chronic phase but neither
speeds nor delays blast crisis.
Newer therapies (alpha-interferon with or without cytarabine)
suppress the leukemic clone and do prolong survival.
The only hope for a cure so
far is allogenic bone marrow transplantation.
In around 30% of these cases, the blasts express lymphoid differentiation (TdT, etc.) T-cell blast crisis:
Am. J. Cln. Path. 107: 168, 1997.
WARNING: The following "myeloproliferative diseases" are all "tumors of the multipotent myeloid
stem cell", and can transform into one another (usually from a mild one to a bad one):
polycythemia vera rubra
1 hemorrhagic ("essential") thrombocythemia
agnogenic myeloid metaplasia
idiopathic "aplastic anemia"
chronic myelogenous leukemia
Historically, many patients have been exposed to drugs or chemicals.
Exposure to benzene, which used to be
a household chemical, is notorious.
In the 1990's, it became clear that most cases of aplastic anemia are caused
by T-cell-mediated attacks on the hematopoietic marrow. This explains why...
CHRONIC LYMPHOCYTIC LEUKEMIA ("CLL", "well-differentiated lymphocytic leukemia"; "the
liquid phase of well-differentiated lymphocytic lymphoma", etc.) NEJM 333: 1093, 1995.
This indolent cancer is a clone of B-cells that multiply slowly and do nothing useful.
T-cell CLL is much less common, but does occur: Blood 86: 1163, 1995.
The one known risk factor is ataxia-telangiectasia (homozygotes,
very likely heterozygotes), and not
surprisingly, this gene is often mutated in sporadic cases
(Lancet 353: 26, 1999.)
* Nothing much has come of a proposal to divide CLL into "typical" and
"atypical".
* CLL has a few common genetic markers but they also occur in other B-cell neoplasms
(Semin. Hem. 36: 171, 1999.
The disease is often an incidental finding, when a CBC shows preposterously a high lymphocyte count.
(* Future hematologists: These cells are fragile on smears, and crushed CLL cells are called "smudges").
{08784} CLL
Paraneoplastic syndromes are more troublesome in this disease than in most other leukemias.
Around 15% of patients get autoimmune hemolytic anemia.
The lymphocytes do somewhat suppress the heathy plasma cells, and the patients have troubles with
infections.
* A few percent develop a marker paraprotein, usually kappa IgM, or get mu heavy chain disease.
Patients with anemia or thrombocytopenia from CLL survive around 2 years. Asymptomatic people
with CLL as an incidental finding generally survive more than ten years.
A few percent of patients develop a diffuse large-cell lymphoma. This is the rapidly-fatal Richter's
syndrome (NEJM 324: 1267, 1991); predisposing
factors remain mysterious (Cancer 67: 997, 1991.
* Around 1% of CLL terminates as ALL ("blast crisis of CLL").
* Prolymphocytic leukemia is an uncommon, aggressive variant of CLL.
Chemotherapy for end-stage CLL: NEJM 330: 319, 1994. No miracles.
HAIRY CELL LEUKEMIA
This distinctive leukemia is named for the many hair-like projections on its surface.
It was of unknown histogenesis (* confusing surface markers) until "rearranged immunoglobulin genes
that are expressed" established it as a B-cell neoplasm" ("Big Robbins").
There is a modest male predominance. Patients have pancytopenia and circulating "hairy lymphocytes";
they survive for several years. The distinctive physical finding is massive splenomegaly. Bone marrow
aspiration is likely to be unsuccessful "because the cellular hairs tangle with one another."
The hairs are quite distinctive, and the diagnosis is clinched by the finding of tartrate-resistant acid
phosphatase (TRAP) in these cells.
A suggested link to HTLV-II didn't work out, but stay tuned for some other virus.
Until recently, the only treatment for this disease was splenectomy, which helped. Nowadays, alpha-interferon is a mainstay
of treatment (Cancer 67: 1943, 1991), and there are claims of long-term
remission following administration of 2-chlorodeoxyadenosine (NEJM 322: 1117, 1990).
* Hairy cell leukemia and adolescent mediastinal T-lymphoblastic lymphoma
are both much more common among men. Maybe this means they're virus-related.
Somebody might ask you this sometime.
{23872} hairy cell leukemia
POLYCYTHEMIA VERA ("Osler's polycythemia", "P. V. rubra", etc.; Mayo Clin. Proc. 78: 174, 2003)
By convention, polycythemia (a better synonym is erythrocytosis) describes an abnormally high
hemoglobin. Classification:
Absolute polycythemia (i.e., increased circulating red cell mass):
Primary polycythemia (i.e., the main problem is with the red cells)
Polycythemia vera rubra
NOTE: Cancer of the normoblasts (i.e., AML-M6) isn't considered a polycythemia
Secondary polycythemia (i.e., the main problem is elsewhere)
Effective renal arterial hypoxia
Emphysema
Tetralogy of Fallot
Hemoglobins with too much oxygen affinity
Etc., etc.
Erythropoietin-producing tumors
Renal cell carcinoma
* Hepatocellular carcinoma
* Cerebellar hemangioblastoma (?!)
Anabolic steroid users
Sleep apnea
After kidney transplant (over-zealous proximal tubule produces erythropoietin)
Altitude (above about 10,000 feet for a long time? Expect problems.
Stroke risk: Stroke 26: 562, 1995. Pulmonary vein thrombosis:
Hum. Path. 21: 601, 1990.
"Primary familial polycythemia" (truncated
erythropoietin receptor;
(J. Clin. Invest. 102: 124, 1999)
* NOTE: "Gaisbock's stress erythrocytosis",
an alleged polycythemia of middle-aged men
with low erythropoietin, remains elusive: Red Cells 22: C1, 1997. I suspect
the original patients had sleep apnea and were on diuretics for
hypertension.
* Erythropoietin-dependent polycythemias (altitude, post-transplant) can
be ameliorated using ACE inhibitors, which is puzzling: Lancet 359:
663, 2002.
Relative polycythemia (i.e., dehydration)
Polycythemia vera is a proliferation of stem cells (again, the common precursors of red cells,
granulocytes, and megakaryocytes). This time, they are very erythropoietin-sensitive and mostly mature
into red cells.
The cells are the common ancestors of red cells, neutrophils, and megakaryocytes. Over the course of
years, these stem cells replace the normal stem cells of the marrow. Their progeny, however, are fully
functional. (Neutrophils even have normal alkaline phosphatase levels.)
In addition to a high red cell count, white cells and platelets are likely to be high.
On biopsy, expect to see a very hypercellular marrow, with all cell lineages increased. In the late stages,
there is often
marrow fibrosis ("burned out PVR", * PDGF effect) or replacement by blasts (transformation to acute
myelogenous leukemia -- still no good treatment Cancer 104: 1032, 2005).
This is a disease of older middle-age. Until the last stages, patients are troubled primarily by the
increased volume of hyperviscous blood.
This causes congestion of most organs ("the plethoric face", etc.)
More troubling, the stasis of gooey blood in the veins promotes clotting.
Or distended veins can rupture (GI bleeding, hemorrhagic stroke). Eventually these patients get platelet
problems, too, which does not help the bleeding tendency.
Minor mystery of medicine: Itching after taking a hot shower is very suggestive of PVR.
The mainstay of treatment for polycythemia vera is regular phlebotomy, to keep the red cell count down.
Patients can expect to survive for ten years or more, with control of most of their problems, until the
disease transforms into something else.
The once-popular practice of giving these patients radioactive phosphorus resulted in a greatly increased
rate of transformation to acute leukemia, turning a not-so-bad, easy-to-control disease into a lethal,
untreatable one.
* Criteria for the diagnosis of PVR:
A1... Increased RBC mass ( >36 mL/kg; >32 mL/kg)
A2... Normal arterial PO2
A3... Splenomegaly
B1... Platelets greater than 400,000/L
B2... WBC >12,000/L
B3... Leukocyte alkaline phosphatase over 100 in the absence of evidence of infection
B4... Elevated serum vitamin B12.
Make the diagnosis if:
(1) You have A1 + A2 + A3, or
(2) A1 + A2 + any two B's.
New criteria will probably be changed to (1) low serum erythropoietin
and (2) studying the ability of cultured normoblasts to grow without
erythropoietin (Mayo Clin. Proc. 74: 159, 1999).
* Thrombosis, the most troublesome aspect of this disease,
seems to be much less of a problem if patients are simply given low-dose aspirin
(NEJM 350: 114, 2004).
AGNOGENIC MYELOID METAPLASIA and MYELOFIBROSIS
Agnogenic myeloid metaplasia is a proliferation of neoplastic stem cells in the bone marrow (which merely becomes
hypercellular)
and the red pulp of the spleen (which enlarges greatly).
As in polycythemia vera, the cells that enter the blood are fully functional. This time, there is no
tendency to over-produce red cells; neutrophils may be super-abundant and "left-shifted" (Philadelphia-chromosome negative, of
course), or there may be neutropenia, or the WBC may be normal. Platelets
are unaffected or even increased (until maybe very late).
This is a disease of older adults. Patients are most likely to be troubled by feeling full after they've eaten
just a little (why?).
Examine the peripheral smear. Red cells made in the spleen tend to be teardrop-shaped (one form of
"poikilocyte"), and nucleated red-cell precursors from the spleen are more likely to escape into the
circulating blood.
{12302} teardrop reds
NOTE: The important term leukoerythroblastic smear refers to the presence in the bloodstream of young
red cells and young granulocytes. You'll see this when they are "being pushed out of their place of
origin too fast":
bone marrow infiltration
agnogenic myeloid metaplasia
metastatic carcinoma
lymphoma
leukemia
bone marrow hyperplasia / extramedullary hematopoiesis
severe hemolysis, etc.
After this process has been underway for several years, the bone marrow undergoes dense fibrosis. Long
mysterious, it is now clear that the marrow fibroblasts are responding to over-production of PDGF
(platelet-derived growth factor) and * transforming growth factor-beta produced by abnormal
megakaryocytic cells.
{13799} myelofibrosis, marrow core biopsy
Patients ultimately die of cytopenia or transformation to acute leukemia.
The term "agnogenic" means "of unknown cause" (i.e., it's a synonym for "idiopathic"; * ask
Dr. Thomas Huxley for cognates).
* Diagnosticians: Unexplained myelofibrosis without splenomegaly suggests M7 AML, burning-out
CML, or burned-out polycythemia vera; look also for carcinoma cells.
* Autoimmune myelofibrosis may result from lupus or "just happen";
future pathologists recognize it by the absence of any abnormalities of the
remaining marrow cells, and clusters of lymphocytes. Am. J. Clin. Path. 116: 211, 2001.
PLASMA CELL MYELOMA ("multiple myeloma", "malignant plasmacytoma") NEJM 336: 1657,
1997; Lancet 363: 875, 2004.
This is cancer of the plasma cells (i.e., cancer of B-cells that are differentiated enough to secrete an
immunoglobulin and/or a light chain (kappa or lambda, though of course never both), or at least to look
like plasma cells).
Myeloma is only slightly less common than leukemia or lymphoma. The typical
patient is in his or her fifties.
The etiology is obscure, and the disease seems to strike at random.
* Blacks have a slightly increased rate.
The term "multiple myeloma" comes from its tendency to make multiple holes ("lytic lesions") in the
bone marrow ("myelo-") and nearby cortex. The effect is mediated, at least in part, by lymphotoxin
(TNF-beta). Cancer of plasma cells always involves bone, but only about half of cases feature good
"punched-out" x-ray lesions. The remaining patients have diffuse disease and suffer precocious
osteoporosis.
{08462} bony lesions of myeloma (skull and spine)
The monoclonal protein (immunoglobulin or chain) produced by an abnormal clone of multiple
myeloma cells is called the M-protein.
If there's a complete antibody, you'll see it on serum protein electrophoresis.
Free light chains may be produced along with, or instead of, a complete immunoglobulin. They pass
easily through the glomerular basement membrane, so you will probably not find them in the
bloodstream if the kidneys are working. Instead, they accumulate in the urine, where they are called
Bence-Jones protein. About 2/3 of myeloma patients produce Bence-Jones protein.
Later on, Bence-Jones protein plugs up the renal tubules, and contributes to "myeloma kidney", which
we'll study in the "renal pathology" section.
You remember that plasma cell myeloma is an important cause of amyloidosis B ("AL"), which doesn't
help renal function, either.
Here's a breakdown on types of M-proteins: 55%...IgG
A paraprotein is an abundant, useless, monoclonal protein in the bloodstream. All M-proteins are
paraproteins; you'll meet others. Lots of an M-protein will produce rouleaux formation; we'll talk more
about this in "Clinical Pathology".
NOTE: As a rule, plasma cell myeloma does not make IgM pentamers. Waldenstrom's does this, and
you won't see the typical bone changes.
To make the diagnosis, you will want to find an overabundance (>15% or so) or sheets of plasma cells
(typical or weird-looking) on bone marrow.
{16554} plasma cell myeloma, cells
Normally, only around 3% of bone marrow cells are plasma cells, but whenever there is widespread B-cell activation, their
number can increase substantially.
* Future pathologists: In reactive plasmacytic disorders, plasma cells encircle the vessels. In plasma cell
myeloma, you'll probably find plasma cells encircling fat cells.
Patients look forward to several years of good-quality survival on chemotherapy. They face the
following problems:
{17273} myeloma kidney, Bence-Jones casts with foreign body reaction
The tumor generally excites no fibrous or osteoblastic response. At autopsy, the tumor masses (if
distinguishable) look and feel like reddish-gray jelly.
Prognosis is much better, due both to chemotherapy and to bisphosphonate management
of bone disease. The monoclonal bortezomib is very promising.
Thalidomide for refractory
myeloma NEJM 341: 1565, 1999.
OTHER PLASMA-CELL PROBLEMS ("plasma cell dyscrasias", an archaic term)
There are a variety of other monoclonal plasma cell proliferations.
We already looked at Waldenstrom's macroglobulinemia and the heavy-chain diseases under "non-Hodgkin's
lymphomas". These are cancers of small lymphocytes with "plasmacytoid" features.
Solidary plasmacytomas may appear benign grossly and microscopically, and they may or may not
produce immunoglobulins.
Those in bone almost always recur as plasma cell myeloma.
Those in extra-osseous sites ("plasmacytic lymphoma") may often be resected for cure.
Monoclonal gammopathy of uncertain significance ("MGUS", the old "benign monoclonal
gammopathy") affects maybe 3-10% of older adults ("Big Robbins" wrongly suggests that it is less
common than plasma cell myeloma).
This is best considered a benign, disseminated proliferation of plasma cells with some potential to
transform into malignancy.
The tumor cells produce a single, complete immunoglobulin
(usually IgG) that may be detected on serum protein
electrophoresis.
Maybe 1/4 of these people eventually go on to get sick from plasma cell myeloma, amyloidosis B, or
macroglobulinemia (Mayo Clin. Proc. 68: 26, 1993); newer work gives the rate
at about 1%/year (NEJM 346: 564, 2002)
Amyloidosis B may arise in this setting, and probably all non-cancer-related amyloidosis B cases have
a hyperactive clone of plasma cells.
* Workup of a monoclonal gammopathy: Arch. Path. Lab. Med. 123:
106 & 108 & 114, 1999).
* POEMS may arise: polyneuropathy, organomegaly, endocrinopathy (thyroid/gonads), monoclonal
gammopathy (usually IgA-lambda), and skin changes.
The cause must be cytokines, but the exact etiology remains elusive
(Am. J. Resp. Crit. Care Med. 157: 907, 1998).
* Cryoglobulinemia type I is a monoclonal immunoglobulin of marginal solubility. More about this in
"Clinical Pathology"!
Follow these people up for decades, and around one in four will get some kind of serious gammopathy
(Mayo Clin. Proc. 68: 26, 1993).
Polyclonal activation of plasma cells ("polyclonal gammopathy") is a common finding in clinical
medicine. Situations worth remembering:
THE LANGERHANS CELL HISTIOCYTOSIS FAMILY ("Histiocytosis X", "disseminated
histiocytosis"; * R&F "differentiated histiocytosis" is a typo); review for clinicians
J. Ped. 127: 1, 1995;
Cancer 85: 2278, 1999.
A group (probably a continuum) of lesions that are probably honest-to-goodness tumors of
Langerhans-type histiocytes, a class of dendritic macrophages.
Langerhans cells in health and disease are characterized by intracellular Birbeck granules ("histiocytosis
X bodies"), pentalaminar tennis-racket shaped structures of unknown significance.
{09095} Birbeck granules
In tissue, you will probably see a range of cells from "blasts" to well-differentiated Langerhans cells.
The former claim that histiocytosis X is "polyclonal" probably resulted from confusion of the tumor cells
with non-neoplastic inflammatory cells that had entered the tumor. The current work indicates clonality
(NEJM 331: 154, 1994; Br. Med. J. 310: 74, 1995; Lancet 344: 1717, 1994).
* You know T4 and T8 antigens from your study of AIDS. Future pathologists: Histiocytosis X and the
dendritic macrophages from which it derives stain for CD1/T6. They also stain with S-100.
* The old names belong to medical history, but you'll see the syndromes:
Letterer-Siwe disease ("acute disseminated histiocytosis") affects small children and involves most of
the body's organs. These children are now often cured with elaborate chemotherapy.
{23392} Letterer-Siwe disease. Weird histiocytes ("coffee-bean nuclei, even"). Trust me.
Eosinophilic granuloma (an unfortunate misnomer) causes solitary bone lesions in young people. The
histiocytes have coffee-bean nuclei and are admixed with eosinophils. Modest treatment generally is
curative.
{13688} eosinophilic granuloma
Hand-Schüller-Christian disease affects the skull bones and other body parts. It's intermediate between
the other two in severity.
{10481} Hand-Schüller-Christian disease. Weird histiocytes. Trust me.
The healthy spleen weighs 150 gm or less. * "Big Robbins" has a nice review of its structure and
functions.
Splenomegaly must be substantial (800 gm or so) to be palpable. Causes worth remembering:
Infections
Malaria (huge spleens)
Infectious mononucleosis family (see above)
Bacterial endocarditis (don't miss this one)
Most other bad infections (NOTE: A "septic spleen" feels soft, unlike most of the other big spleens)
Congestion (if longstanding, becomes "fibrocongestive")
Cirrhosis
Right-sided heart failure
Splenic vein thrombosis
Sludging of red cells
Sicklers
Polycythemia vera
Waldenstrom's
Others
Others
Diseases of white cells
Chronic myelogenous leukemia (huge spleens)
Agnogenic myeloid metaplasia (huge spleens)
Hairy cell leukemia (very large spleens)
All the other ones
Splenic over-destruction of blood cells
Hereditary spherocytosis
Hemoglobinopathies and bad thalassemia
Immune hemolytic anemia
Immune thrombocytopenic purpura
Immunoreactive hyperplasia
Lupus
Rheumatoid arthritis
Graft rejection
Storage diseases (huge spleen)
Gaucher's (very big, wadded-kleenex macrophages)
Niemann-Pick's (very big, foamy macrophages)
Hunter's
Hurler's
Sarcoidosis
Amyloidosis (sago, lard)
Hypersplenism is said to be present when an enlarged spleen destroys formed elements of blood too
readily. The three causes most worthy of remembering: (1) cirrhosis; (2) rheumatoid arthritis (the
serious "Felty's syndrome"), and (3) Gaucher's disease.
{00239} Gaucher's disease, spleen
The only proof that hypersplenism was the problem is that the blood counts get better when the spleen
is removed.
Accessory spleens (one or more) are present somewhere in the abdomen in about 25% of autopsies. If
you need a splenectomy for a medical disease (i.e., immune thrombocytopenic purpura, hereditary
spherocytosis), you must hope that your surgeon does not overlook a large accessory spleen.
Septic spleen ("nonspecific acute splenitis") is typical of serious bacterial infections. Loaded with polys
and abnormally soft, the old gourmet pathologists made the comparison to "tomato paste" (yuck).
Hyperplastic spleen usually means large germinal follicles in the white pulp. Think of systemic
autoimmune disease, infectious mononucleosis, graft rejection, etc., etc.
In infectious mononucleosis, the spleen also becomes infiltrated with activated T-cells that give a
malignant appearance. Don't expect to actually see such a spleen removed at surgery unless you first
palpate these patients really hard....
* Future pathologists: Telling hyperplasias from lymphomas in the spleen is one of your toughest calls.
For help, see Am. J. Clin. Path. 99: 486, 1993.
Infarcts are common in the spleen, and may result from atheroembolization (the twisty splenic artery
is the most severely affected in the body), left-sided endocarditis, or infiltrative disease.
* Necrosis in a blood-bloated spleen (typically, in sicklers) is likely to produce iron- and calcium-rich
scars called Gamna-Gandy bodies. The "autosplenectomized" spleen of an older sickle-cell disease
patient is mostly composed of such scars.
Primary neoplasms of the spleen are uncommon. Benign tumors are almost never of any importance.
Any lymphoma or endothelial neoplasm can arise here. Metastases to the spleen are expected in most
leukemias and Hodgkin's and non-Hodgkin's lymphomas, but carcinomas and sarcomas very seldom
grow in the spleen.
Ruptured spleen results from blows (hard if you're healthy, lighter blows suffice for those with infectious
mononucleosis; remember CPR as a cause Br. Med. J. 322: 480, 2001).
Intraperitoneal hemorrhage results in a trip to surgery. If a lot of pulp escapes into the
peritoneal cavity, the patient may heal with hundreds of mini-spleens over the peritoneal cavity
(splenosis).
You remember
the difference between sections and smears, right? "It is futile," I said,
You lie," he cried,
--Stephen Crane
10110 ff blood
{10766} leukemia, hairy cell and normal
Pelger-Huet
Blood picture
WebPath Photo
{40654} toxoplasmosis; tissue reaction (lame-looking granulomas)
Follicular hyperplasia
WebPath Photo
Lymphomas
Cornell
Class notes with clickable photos
 Lymphomas and Plasma Cell Neoplasms
Lymphomas and Plasma Cell Neoplasms
"Pathology Outlines"
Nat Pernick MD
Lung lymphoma
Lung pathology series
Dr. Warnock's Collection
* Ataxia-telangiectasia (homozygotes, probably heterozygotes)
is a risk factor for most lymphomas and lymphoid leukemias.
Diffuse lymphoma
WebPath Photo
Tingible body macrophages
WebPath Photo
* In AIDS, mantles are likely to absent. Why?
If it is apparently made of small lymphoid cells, the pathologist stains
for kappa and lambda (monoclonality is lymphoma, polyclonality is non-malignant),
and a bcl2 stain if there are nodules (positive staining indicates lymphoma).
Lymphoma in lymph node
Invasion of surrounding fat
Tom Demark's Site
* Prognosticating and depth-analyzing aggressive B-cell lymphomas by their
mutations: Nat. Med. 8: 13 & 68, 2002. More: NEJM 350: 1828, 2004.
This may be important in the future.
The 1993 Revised European-American Classifications of Lymphoid Neoplasms
("REAL") is based on newer work with differentiation markers;
its present formulation includes slight alterations
by the W.H.O.
Precursor B lymphoblastic leukemias and lymphomas
Precursor T lymphoblastic leukemias and lymphomas
Chronic lymphocytic leukemia / small lymphocytic lymphoma
Lymphoplasmacytic lymphoma
Mantle cell lymphoma
Follicular cell lymphoma, cytologic grade I
Follicular cell lymphoma, cytologic grade II
Follicular cell lymphoma, cytologic grade III
Marginal zone lymphoma
MALT lymphoma ("mucosal-associated lymphoid tissue" of stomach, thyroid, salivary glands, etc.)
Hairy cell leukemia
Plasmacytoma / plasma cell myeloma
Diffuse B-cell lymphoma
Burkitt's lymphoma / leukemia
T-cell chronic lymphocytic leukemia
Large granular lymphocytic leukemia
Mycosis fungoides / Sezary syndrome
Peripheral T-cell lymphoma, unspecified
Angioimmunoblastic T-cell lymphoma
Angiocentric NK/T-cell lymphoma
Intestinal T-cell lymphoma
Adult T-cell leukemia/lymphoma
Anaplastic large-cell lymphoma
Adults (all are peripheral B-cell lesions):
Chronic lymphocytic leukemia / small lymphocytic lymphoma
Children:
Follicular lymphoma
Plasmacytoma / plasma cell myeloma
Diffuse large B-cell lymphoma
Precursor B-cell leukemia
Precursor T-cell leukemia
Burkitt's lymphoma / leukemia
Pathologists often identify "proliferation centers", discrete clumps of somewhat
larger cells that supposedly give rise to the normal-looking tumor
cells. These are supposed to be pathognomonic of CLL/SLL.
Well-differentiated lymphocytic lymphoma
Tom Demark's Site
* Most of these feature the translocation t(9;14), causing aberrant
expression of PAX5.
Small lymphocytic lymphoma
with amyloidosis
Great discussion
Rockford Case of the Month
A B-cell tumor that always features t(11;14), involving BCL1 (cyclin D1)
(assay Am. J. Path. 154: 1449, 1999; Blood 93:
1372, 1999, easy to stain for in sections).
An indolent lymphoma that often arises extranodally.
{23683} mixed lymphoma
{23581} nodular lymphoma
{23593} diffuse small cleaved lymphoma (all you can
tell is that it is diffuse)
{46344} diffuse small cleaved lymphoma, marrow
Small cleaved lymphocyte in blood
Ed Lulo's Pathology Gallery
{15389} large-cell lymphoma
Peripheral T-cell neoplasm
Virginia
Good pictures
 Primary thymic lymphoma
Primary thymic lymphoma
Virginia
Good pictures
The old "immoblastic lymphoma" of the Working Classification
was a mix of several of these lymphomas and T-cell lymphomas.
{10691} immunoblastic lymphoma, cytology
{10724} immunoblastic lymphoma
{10772} immunoblastic lymphoma
{23623} immunoblastic lymphoma
{23689} immunoblastic lymphoma
{10937} lymphoma arising in thyroid; my case. Notice that the lymphocytes are growing within a
follicle.
Body cavity lymphoma and Hodgkin's
Lung pathology series
Dr. Warnock's Collection
Post-transplant lymphoproliferation
Pittsburgh Pathology Cases
Post-Transplant Neoplasia
Great site
Transplant Pathology Internet Services
{11630} lymphoma in the pericardial space
{11633} lymphoma, primary in the heart
{20227} lymphoma, primary in the stomach
{15446} lymphoma, primary in the stomach
{15542} lymphoma, primary in the stomach
{49035} African Burkitt's
Epstein-Barr
Post-transplantation lymphoproliferative disorder
WebPath Photo
{23620} Burkitt's lymphoma, lipid drops
{46336} Burkitt's lymphoma, lipid drops
{23611} Burkitt's lymphoma, good starry sky
{46332} Burkitt's lymphoma, good starry sky
{23641} * Burkitt's, methyl green pyronine (the red "pyroninophilia" merely tells us that the cytoplasm
is rich in ribosomes)
{40004} mycosis fungoides
{12747} mycosis fungoides, plaque phase
{12751} mycosis fungoides
{12754} mycosis fungoides
{13117} mycosis fungoides
{13781} mycosis fungoides
{13784} mycosis fungoides
{24740} mycosis fungoides, histopathology; note Pautrier microabscesses
{12759} mycosis fungoides, Pautrier microabscesses
{13793} mycosis fungoides, Pautrier microabscess
{13796} mycosis fungoides cells in a lymph node (look
how wiggly the nuclear membranes are)
{09042} mycosis fungoides cell, electron micrograph
{16544} Sézary cell
{23722} Sézary cell
{15409} Sézary cell
Primary Effusion Lymphoma
This is usually from KSHV
Virginia Pathology Cases
Tomorrow's medicine: Rituximab "Rituxan", an antibody against CD20, is revolutionizing
treatment of B-cell lymphomas (Am. J. Clin. Path. 119: 472, 2003;
Blood 101: 949, 2003; lots more).
Also watch for Y-ibrituxomab tiuxetan (Blood 99: 4336, 2002;
Cancer 94: 1349, 2002). Best so far: I131-toditumomab, radioactive anti-CD20,
with a high five-year symptom-free survivals in follicular lymphomas.
 You must recognize the classic Reed-Sternberg cell:
You must recognize the classic Reed-Sternberg cell:
{20057} Reed-Sternberg cell
{36398} Reed-Sternberg cell, not H&E; cytology
{36401} Reed-Sternberg cell, not H&E; cytology
{40423} Reed-Sternberg cell, mitosis
Reed-Sternberg Cell
Spectacular photomicrograph
Brazilian Medical Students
{46339} Lymphocyte predominance Hodgkin's
{46342} mixed cellularity Hodgkin's disease
{46343} mixed cellularity Hodgkin's disease
* Prognosticating based on biopsy: Blood 101: 4063, 2003.
{23545} nodular sclerosing Hodgkin's disease
{23548} lacunar Reed-Sternberg variants
{23551} lacunar Reed-Sternberg variant
{46348} Hodgkin's disease in the spleen
{46349} Hodgkin's disease in the spleen
Leukemia / myelodysplasia
"Pathology Outlines"
Nat Pernick MD
{36032} packed marrow; * this was AML
{12347} packed marrow; * this was AML
{29475} lymphoid blasts, pap stain. Big pale nuclei.
* Auer rods in preleukemia: Am. J. Clin. Path. 124: 191, 2005.
{08734} acute leukemia, liver; as you would expect, the leukemia is blue
{08735} acute leukemia, liver
{08736} acute leukemia, liver
{01735} brain and dura, acute leukemia
 ALL
ALL
Pittsburgh Pathology Cases
* Authoritative mega-review for pathologists considering
a diagnosis of leukemia in a child: Am. J. Clin. Path. 109(4S1):9S, 1998.
{23833} L1, special stain (cytoplasm is brown)
{23860} L2
{13982} L2, bone marrow
{23758} L3; note the lipid
{13985} L3
"pre-B"/"null", with surface Ig and TdT, carries a good prognosis;
Burkitt's / L3 is ominous
{32027} ALL in the liver
{34513} ALL in the brain
{49316} ALL in the kidney
{49343} ALL in the testis
Bloom's
ataxia telangiectasia
Fanconi's anemia (a complex genetic disorder; * gene
FancC Blood 94: 1, 1999.)
{16245} blast, and not much else, M1
{13988} blasts, and not much else, M1
{23830} blast, * chloroacetate-esterase (+), M1
{13940} blast, * chloroacetate-esterase (+), M1
{23839} blast, M1; note nucleolus.
{23770} blasts with a few granules, M2
{13991} blasts with a few granules, M2
{16249} blast with Auer rod, M2
{12344} blast with Auer rod, M2 or maybe M3
{14010} blast with great auer rods
{23776} blasts with lots of granules, M3
{13994} blasts with lots of granules, M3
{16254} blasts with lots of granules, M3
{10109} blasts with lots of granules, M3
{13997} semi-monocyte like blasts, M4; note indented nucleus and gray cytoplasm
{10133} semi-monocyte like blasts, M4
{13937} non-specific esterase in M4
{23800} monocyte-like blasts in M5
{40449} monocyte-like blasts in M5
{40451} monocyte-like blasts in M5
{23803} non-specific esterase in M5
{14001} monocyte-like blasts in M5
{13928} non-specific esterase in M5
{23949} erythroleukemia, M6. If you don't recognize the malignant cells as red-cell precursors, please
check out a histology book.
{14007} erythroleukemia, M6
{16267} erythroleukemia, M6
{23836} erythroleukemia, M6
{23806} erythroleukemia, M6
{16273} erythroleukemia, M6, PAS-positive chunks
{16274} megakaryocytic blasts, M7. See the platelets budding?
{23812} megakaryocytic blasts, M7
{23821} megakaryocytic blasts, M7
{23818} megakaryocytic blasts, PAS-positive, M7
{46340} gingival involvement; this is common in M4 & M5
Various karyotypic abnormalities have been described in the majority of
these people (Virch. Arch. A 421: 47, 1992).
 Gross pathology buffs: A solid growth of myeloblasts is a chloroma or granulocytic sarcoma. This most
malignant of solid tumors turns green (Greek "chloros",
as "chlorine" or "chlorophyll") on exposure to air (why?)
Gross pathology buffs: A solid growth of myeloblasts is a chloroma or granulocytic sarcoma. This most
malignant of solid tumors turns green (Greek "chloros",
as "chlorine" or "chlorophyll") on exposure to air (why?)
{10763} CML, peripheral blood
{12359} CML
{23863} CML (note the basophil)
{23866} CML,
leukocyte
alkaline phosphatase stain (black; note the cells are not stained black)
Chronic granulocytic leukemia
Automated profile
WebPath Photo
Imatinib (STI571, Gleevic), which inhibits the kinase produced by this new
gene, and some others cancer kinases,
is one of the great successes of biotechnology (NEJM 346
645, 2002; NEJM 347: 472, 2002; for blast crisis Cancer 103: 2099, 2005). Watch for more.
Chronic granulocytic leukemia
Philadelphia chromosome
WebPath Photo
{12365} CML, blast crisis
"APLASTIC ANEMIA" (updates Ann. Int. Med. 136: 534, 2002;
Lancet 365: 1647, 2005)
This uncommon, dread illness features the disappearance of the precursors of
granulocytes, erythrocytes, and platelets. (It is poorly-named.)
a marrow transplant from an identical twin never takes;
Other cases of acquired aplastic anemia
seem to be the result of running out of telomere length
during aging. Some families and some individuals
have less telomerase than others (to oversimplify, but
the impact seems real): NEJM 352: 1413, 2005.
Aplastic anemia
WebPath Photo
CLL
Smudge cells
Great discussion
Rockford Case of the Month
CLL and melanoma together in marrow
Pittsburgh Illustrated Case
We know of no other specific risk factors, not even a history of radiation.
{12389} CLL
{12404} CLL going bad (some blasts)
{12386} CLL with smudges
* Future pathologists: The other "hairy" B-cell neoplasm is "lymphoma with
villous lymphocytes", usually in the spleen. The distinctions are subtle, and
the immunotyping of tumors is often variable. Arch. Path. Lab. Med. 124: 1710, 2000.
{10766} hairy cell leukemia, spleen (top; normal at bottom)
{16543} hairy cell leukemia, TRAP stain (red)
{23875} hairy cell leukemia, TRAP stain (red)
{13925} hairy cell leukemia, TRAP stain (red)
{16541} hairy cell leukemia, TRAP stain (red)
{23881} hairy cell leukemia, bone marrow biopsy (trust me)
{42117} big spleen in hairy cell leukemia, foot ruler
Hairy cell leukemia
Case and photos
Loyola Med
{24788} myelofibrosis, marrow core biopsy
{13802} myelofibrosis, reticulin stain
5q- syndrome
Virginia
Good pictures
* The common translocation t(4;14) brings the fibroblast growth factor 3
receptor (on 4; Nat. Genet. 16: 260, 1997) and a novel gene
(Blood 92: 3025, 1998) into control of IgH, the heavy chain gene,
on 14.
{27327} bony lesions of myeloma (skull)
{13769} skull lesions of myeloma
{10760} skull lesions of myeloma
{10754} bone lesions of myeloma
{10757} osteoporosis of myeloma
{46197} femur lesions in myeloma
{46198} rib lesions in myeloma
{27329} spike, probably monoclonal gammopathy of uncertain significance, since normal albumin and
gamma seem not to be suppressed
25%...IgA
1%... IgE, IgD, or IgM monomer
18%... Bence-Jones protein only
1%... no M-protein.
{16556} plasma cell myeloma, cells
{13772} plasma cell myeloma, marrow aspirate
{27330} plasma cell myeloma, marrow aspirate
{13775} plasma cell myeloma, bone marrow section
{10751} * "grape cell"
{42054} * "flame cell" (named for its staining properties)
{17274} myeloma kidney, Bence-Jones casts with foreign body reaction
MGUS
Pittsburgh Pathology Cases
* Langerin, a lectin specific to Langerhans cells, when stimulated
induces its formation (Immunity 12: 71, 2000).
{09097} Birbeck granules
 Histiocytosis X
Histiocytosis X
Pittsburgh Illustrated Case
Histiocytosis X with Birbeck granules
Lung pathology series
Dr. Warnock's Collection
Eosinophilic granuloma of the lung
Lung pathology series
Dr. Warnock's Collection
{13691} eosinophilic granuloma
{09043} eosinophilic granuloma, EM, coffee-bean nucleus (left) and eosinophil (right)
{21779} skull in Hand-Schüller-Christian disease
Spleen
Cornell
Class notes with clickable photos
* Every man has his own ways of courting
the female sex. I should not, myself, choose to do it with photographs
of spleens, diseased or otherwise.
-- Agatha
Christie, "The Moving Finger"
Gaucher's disease
Easy call on biopsy
Loyola Med
{09864} Gaucher's disease, spleen
{16216} Gaucher's disease, watered-silk ("wadded kleenex") cell from spleen
Gaucher's
Photo and mini-review
Brown U.
Exactly why the spleen becomes like this in deaths from sepsis,
and never anything else, remains as mysterious as sepsis itself.
You'll see profound loss of the B-cells and T-helper cells
around the white pulp,
and apoptosis of the dendritic reticular cells that maintain the structure
of the spleen (NEJM 348: 138, 2003).
Sickle cell disease
Autosplenectomy
WebPath Photo
* I SAW A MAN PURSUING
I saw a man pursuing the horizon;
Round and round they sped.
I was disturbed at this;
I accosted the man.
"You can never -- "
And ran on.
(1871-1900)
 * SLICE OF LIFE REVIEW: BLOOD CELLS
* SLICE OF LIFE REVIEW: BLOOD CELLS
{12275} anemia, iron deficiency; normal
{13715} lymphocyte, normal
{13868} red blood cell, normal blood
{13910} red blood cell, normal
{14702} polymorphonuclear leukocyte, normal
{14703} polymorphonuclear leukocyte, normal
{14704} polymorphonuclear leukocyte, normal
{14705} polymorphonuclear leukocyte, normal
{14705} polymorphonuclear leukocyte, normal
{14706} polymorphonuclear leukocyte, normal
{14707} polymorphonuclear leukocyte, normal
{14708} eosinophil, normal
{14709} eosinophil, normal
{14710} basophil, normal
{14711} basophil, normal
{14712} monocyte, normal
{14713} monocyte, normal
{14714} monocyte, normal
{14715} monocyte, normal
{14716} lymphocyte, large
{14717} lymphocyte, large
{14718} lymphocyte, normal
{14719} lymphocyte, normal
{14720} lymphocyte, normal
{14721} lymphocyte, normal
{14722} reticulocytes, normal
{14723} reticulocytes, normal
{14724} red blood cell, abnormal
{14725} red blood cell, abnormal
{14726} platelets, normal
{14727} platelets, normal
{14728} pronormoblast, normal
{14729} pronormoblast, normal
{14730} basophilic normoblast, normal
{14731} basophilic normoblast, normal
{14732} normoblast
{14733} normoblast
{14734} polymorphonuclear leukocyte & * lymphocyte
{14735} polymorphonuclear leukocyte & * lymphocyte
{14736} normoblast series
{14737} normoblast series labelled
{14738} myelocyte, normal
{14739} myelocyte, normal
{14740} * granulocyte series
{14741} * granulocyte series (labelled)
{14742} myelocyte, band form
{14743} myelocyte, band form
{14744} myelocyte, normal
{14745} myelocyte, normal
{14746} myelocyte, normal
{14747} myelocyte, normal
{14748} myelocyte, normal
{14749} myelocyte, normal
{14750} myelocyte, normal
{14751} myelocyte & megakaryocyte, normal
{14752} myelocyte & megakaryocyte, normal
{15193} plasma cell, #23
{15205} thymus, adult
{15564} thymus, normal
{15565} thymus, normal
{15566} thymus, normal
{15567} thymus, normal
{16175} red blood cell, normal
{20782} polymorphonuclear leukocyte, normal
{20783} monocyte
{20784} platelets, circulating blood
{20785} monocyte
{26230} polymorphonuclear leukocyte, normal
{40179} thymus, norma
{46538} red cell, normal
 * SLICE OF LIFE REVIEW: LYMPHOID ORGANS
* SLICE OF LIFE REVIEW: LYMPHOID ORGANS
{11750} spleen, normal
{11751} spleen, normal
{11753} lymph node, normal
{11797} spleen, normal
{11805} spleen, normal unfixed
{14753} thymus, human fetal
{14754} thymus, human fetal
{14755} thymus, juvenile
{14756} thymus, juvenile
{14757} thymus, adult
{14758} thymus, adult
{14759} thymus, juvenile
{14760} thymus, juvenile
{14761} hassall's corpuscles
{14762} hassall's corpuscles
{14763} hassall's corpuscles
{14764} hassall's corpuscles
{14765} thymus (septum)
{14766} thymus (septum)
{14767} spleen, normal
{14768} spleen, normal
{14769} spleen, pulp
{14770} spleen, pulp
{14771} spleen (trabeculae), normal
{14772} spleen (trabeculae), normal
{14773} spleen (trabecular artery), normal
{14774} spleen (germinal center), normal
{14775} spleen (germinal center), normal
{14776} spleen (venous sinus), normal
{14777} spleen (venous sinus), normal
{14778} spleen (scanning em)
{14779} spleen (scanning em)
{14780} lymph node, normal
{14781} lymph node, normal
{14782} lymph node cortex, normal
{14783} lymph node cortex, normal
{14784} lymph node, medulla
{14785} lymph node, medulla
{14786} lymph node, normal
{14787} lymph node, normal
{15189} lymph node and subcapsular sinus, #23
{15190} lymph node, primary nodule
{15191} lymph node, germinal center
{15192} lymph node, medulla
{15194} spleen, #24
{15195} spleen, * red pulp and white pulp
{15196} spleen, central artery
{15197} spleen, central artery and germinal cent
{15198} spleen, trabeculae
{15199} thymus, #25
{15200} thymus, cortex
{15201} thymus, hassall's corpuscle
{15202} thymus, medulla
{15203} thymus, epithelial reticular cell
{15568} spleen, normal
{15569} spleen, normal
{15570} spleen, normal
{15571} spleen, normal
{15769} spleen, normal
{15770} spleen, normal
{20200} spleen, normal
{20799} lymph node, overview
{20800} lymph node, cortex
{20801} lymph node, medulla
{20802} lymph node, subcapsular sinus
{20803} lymph node, secondary nodule
{20804} lymph node, primary nodule
{20805} spleen, normal histology
{20806} spleen, red pulp
{20807} spleen, white pulp
{20808} spleen, central artery
{20809} spleen, red pulp
{20810} spleen, secondary nodule
{20811} spleen, trabecula
{20812} thymus, overview
{20813} thymus, medulla
{20814} thymus, cortex
{20815} thymus, hassall's corpuscle
{20827} tonsil, palatine
{20828} tonsil, pharyngeal
{24782} lymph node, normal
{24783} lymph node, normal
{36344} lymph node, normal
{36347} lymph node, normal
{36350} lymph node, normal cytology
{36353} lymph node, normal cytology


| Visitors to www.pathguy.com reset Jan. 30, 2005: |
Ed says, "This world would be a sorry place if
people like me who call ourselves Christians
didn't try to act as good as
other
good people
."
Prayer Request
 Teaching Pathology
Teaching Pathology
PathMax -- Shawn E. Cowper MD's
pathology education links
Ed's Autopsy Page
Notes for Good Lecturers
Small Group Teaching
Socratic
Teaching
Preventing "F"'s
Classroom Control
"I Hate Histology!"
Ed's Physiology Challenge
Pathology Identification
Keys ("Kansas City Field Guide to Pathology")
Ed's Basic Science
Trivia Quiz -- have a chuckle!
Rudolf
Virchow on Pathology Education -- humor
Curriculum Position Paper -- humor
The Pathology Blues
 Ed's Pathology Review for USMLE I
Ed's Pathology Review for USMLE I
![]()
![]()
Metastatic malignant melanoma
Virginia
Good pictures
Hairy cell leukemia
Virginia
Good pictures

Pathological Chess

Taser Video
83.4 MB
7:26 min

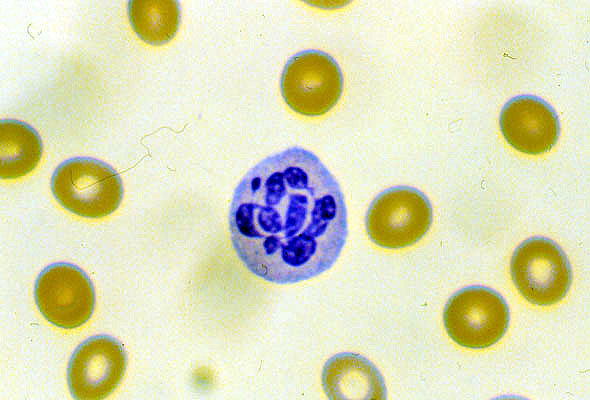 Hypersegmented poly
Hypersegmented poly
 Nodular lymphoma
Nodular lymphoma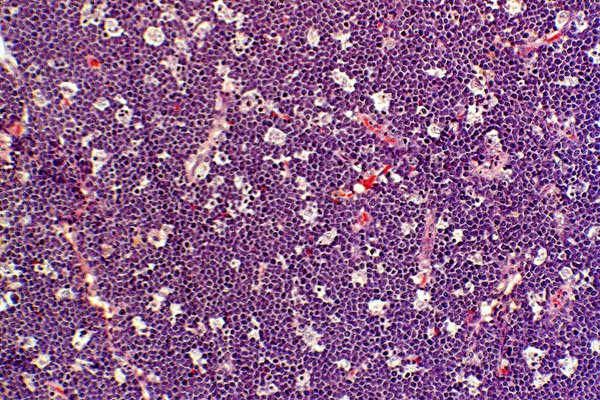 Burkitt's lymphoma
Burkitt's lymphoma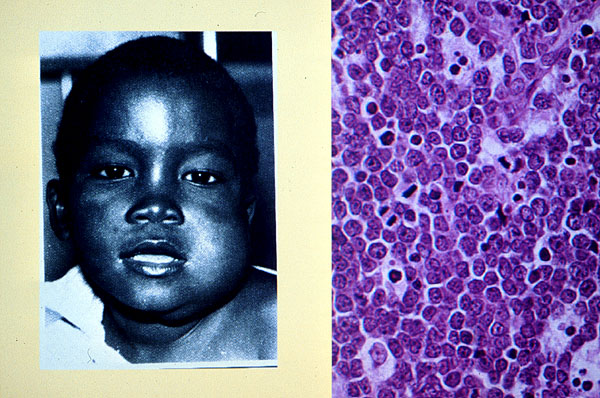 Burkitt's lymphoma
Burkitt's lymphoma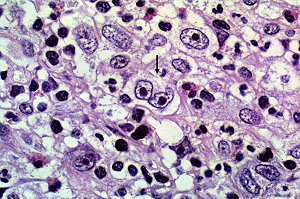 Hodgkin's disease
Hodgkin's disease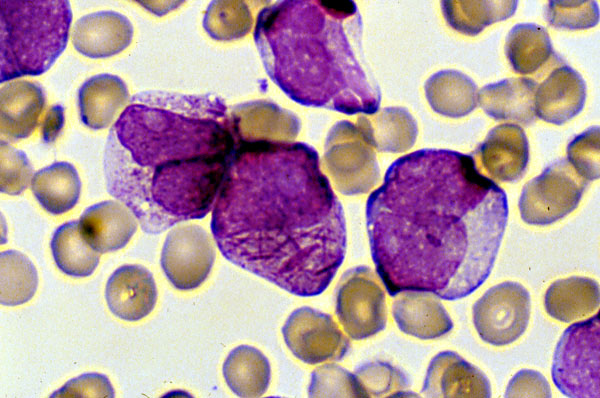 Acute promyelocytic leukemia
Acute promyelocytic leukemia Acute Lymphoblastic Leukemia
Acute Lymphoblastic Leukemia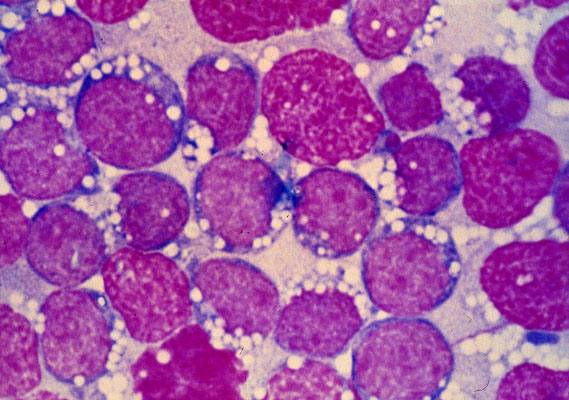 Burkitt's leukemia
Burkitt's leukemia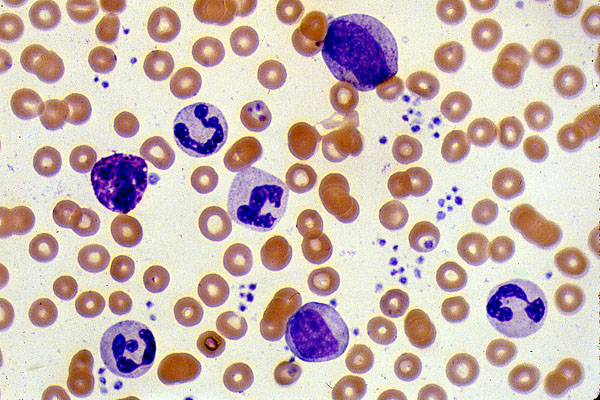 Chronic myelogenous leukemia
Chronic myelogenous leukemia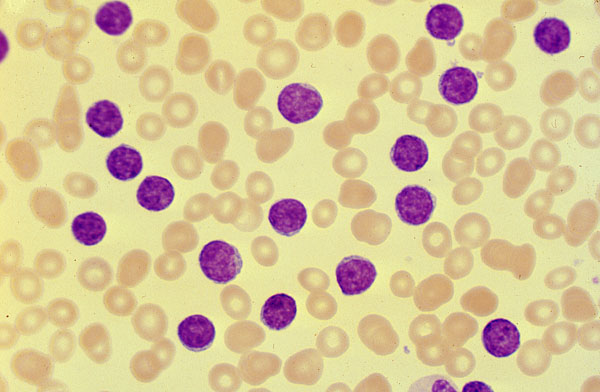 Chronic lymphocytic leukemia
Chronic lymphocytic leukemia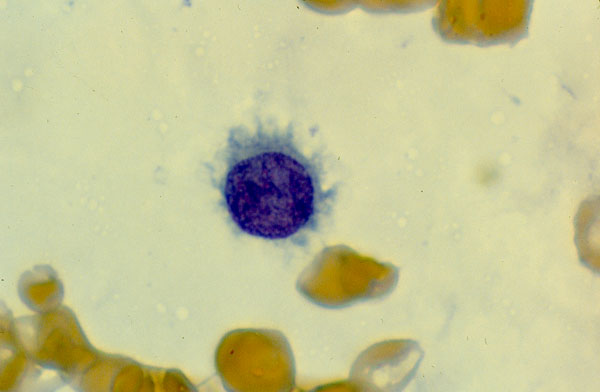 Hairy cell leukemia
Hairy cell leukemia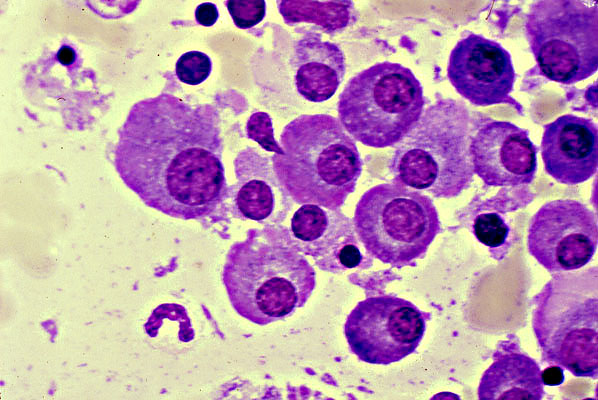 Plasma cell myeloma
Plasma cell myeloma