Ed Friedlander, M.D., Pathologist
scalpel_blade@yahoo.com



Cyberfriends: The help you're looking for is probably here.
Welcome to Ed's Pathology Notes, placed here originally for the convenience of medical students at my school. You need to check the accuracy of any information, from any source, against other credible sources. I cannot diagnose or treat over the web, I cannot comment on the health care you have already received, and these notes cannot substitute for your own doctor's care. I am good at helping people find resources and answers. If you need me, send me an E-mail at scalpel_blade@yahoo.com Your confidentiality is completely respected.
 DoctorGeorge.com is a larger, full-time service.
There is also a fee site at myphysicians.com,
and another at www.afraidtoask.com.
DoctorGeorge.com is a larger, full-time service.
There is also a fee site at myphysicians.com,
and another at www.afraidtoask.com.
Translate this page automatically
 |
With one of four large boxes of "Pathguy" replies. |
 I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
Numbers in {curly braces} are from the magnificent Slice of Life videodisk. No medical student should be without access to this wonderful resource. Someday you may be able to access these pictures directly from this page.
Also:
Medmark Pathology -- massive listing of pathology sites
Freely have you received, freely give. -- Matthew 10:8. My
site receives an enormous amount of traffic, and I'm
handling about 200 requests for information weekly, all
as a public service.
Pathology's modern founder,
Rudolf
Virchow M.D., left a legacy
of realism and social conscience for the discipline. I am
a mainstream Christian, a man of science, and a proponent of
common sense and common kindness. I am an outspoken enemy
of all the make-believe and bunk that interfere with
peoples' health, reasonable freedom, and happiness. I
talk and write straight, and without apology.
Throughout these notes, I am speaking only
for myself, and not for any employer, organization,
or associate.
Special thanks to my friend and colleague,
Charles Wheeler M.D.,
pathologist and former Kansas City mayor. Thanks also
to the real Patch
Adams M.D., who wrote me encouragement when we were both
beginning our unusual medical careers.
If you're a private individual who's
enjoyed this site, and want to say, "Thank you, Ed!", then
what I'd like best is a contribution to the Episcopalian home for
abandoned, neglected, and abused kids in Nevada:
My home page
Especially if you're looking for
information on a disease with a name
that you know, here are a couple of
great places for you to go right now
and use Medline, which will
allow you to find every relevant
current scientific publication.
You owe it to yourself to learn to
use this invaluable internet resource.
Not only will you find some information
immediately, but you'll have references
to journal articles that you can obtain
by interlibrary loan, plus the names of
the world's foremost experts and their
institutions.
Alternative (complementary) medicine has made real progress since my
generally-unfavorable 1983 review linked below. If you are
interested in complementary medicine, then I would urge you
to visit my new
Alternative Medicine page.
If you are looking for something on complementary
medicine, please go first to
the American
Association of Naturopathic Physicians.
And for your enjoyment... here are some of my old pathology
exams
for medical school undergraduates.
I cannot examine every claim that my correspondents
share with me. Sometimes the independent thinkers
prove to be correct, and paradigms shift as a result.
You also know that extraordinary claims require
extraordinary evidence. When a discovery proves to
square with the observable world, scientists make
reputations by confirming it, and corporations
are soon making profits from it. When a
decades-old claim by a "persecuted genius"
finds no acceptance from mainstream science,
it probably failed some basic experimental tests designed
to eliminate self-deception. If you ask me about
something like this, I will simply invite you to
do some tests yourself, perhaps as a high-school
science project. Who knows? Perhaps
it'll be you who makes the next great discovery!
Our world is full of people who have found peace, fulfillment, and friendship
by suspending their own reasoning and
simply accepting a single authority that seems wise and good.
I've learned that they leave the movements when, and only when, they
discover they have been maliciously deceived.
In the meantime, nothing that I can say or do will
convince such people that I am a decent human being. I no longer
answer my crank mail.
This site is my hobby, and I presently have no sponsor.
This page was last updated February 6, 2006.
During the ten years my site has been online, it's proved to be
one of the most popular of all internet sites for undergraduate
physician and allied-health education. It is so well-known
that I'm not worried about borrowers.
I never refuse requests from colleagues for permission to
adapt or duplicate it for their own courses... and many do.
So, fellow-teachers,
help yourselves. Don't sell it for a profit, don't use it for a bad purpose,
and at some time in your course, mention me as author and KCUMB as my institution. Drop me a note about
your successes. And special
thanks to everyone who's helped and encouraged me, and especially the
people at KCUMB
for making it possible, and my teaching assistants over the years.
Whatever you're looking for on the web, I hope you find it,
here or elsewhere. Health and friendship!
 I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
Pathology Education Instructional Resource -- U. of Alabama; includes a digital library
Houston Pathology -- loads of great pictures for student doctors
Pathopic -- Swiss site; great resource for the truly hard-core
Syracuse -- pathology cases
Walter Reed -- surgical cases
Alabama's Interactive Pathology Lab
"Companion to Big Robbins" -- very little here yet
Alberta
Pathology Images --hard-core!
Cornell
Image Collection -- great site
Bristol Biomedical
Image Archive
EMBBS Clinical
Photo Library
Chilean Image Bank -- General Pathology -- en Español
Chilean Image Bank -- Systemic Pathology -- en Español
Connecticut
Virtual Pathology Museum
Australian
Interactive Pathology Museum
Semmelweis U.,
Budapest -- enormous pathology photo collection
Iowa Skin
Pathology
Loyola
Dermatology
History of Medicine -- National Library of Medicine
KU
Pathology Home
Page -- friends of mine
The Medical Algorithms Project -- not so much pathology, but worth a visit
National Museum of Health & Medicine -- Armed Forces Institute of Pathology
Telmeds -- brilliant site by the medical students of Panama (Spanish language)
U of
Iowa Dermatology Images
U Wash
Cytogenetics Image Gallery
Urbana
Atlas of Pathology -- great site
Visible
Human Project at NLM
WebPath:
Internet Pathology
Laboratory -- great site My team:
My team:Ed Lulo's Pathology Gallery
Bryan Lee's Pathology Museum
Dino Laporte: Pathology Museum
Tom Demark: Pathology Museum
Dan Hammoudi's Site
Claude Roofian's Site
Pathology Handout -- Korean student-generated site; I am pleased to permit their use of my cartoons
Estimating the Time of Death -- computer program right on a webpage
Pathology Field Guide -- recognizing anatomic lesions, no pictures

St.
Jude's Ranch for Children
I've spent time there and they are good. Write "Thanks
Ed" on your check.
PO Box 60100
Boulder City, NV 89006--0100
More of my notes
My medical students
Clinical
Queries -- PubMed from the National Institutes of Health.
Take your questions here first.
HealthWorld
Yahoo! Medline lists other sites that may work well for you

We comply with the
HONcode standard for health trust worthy
information:
verify
here. 

![]()
This chapter is absolutely pivotal to your learning medicine. The handout, which is relatively short, is really all mastery material. You need to learn the content at the recall level.
Recognize what things that happen to a person result in inflammation, and distinguish its acute and chronic phases.
Give a full account of the stereotyped processes of acute inflammation. Explain the pathophysiology underlying the classic "rubor, calor, dolor, and tumor", and a complete account of vascular caliber and permeability changes during acute inflammation.
Give a complete account of white cell behavior in acute and chronic inflammation. Tell what white cells are (and aren't) recruited in various kinds of inflammation, and in response to which invaders. Tell the means by which white cells are recruited, the weaponry they carry, and how they find and destroy invaders.
Explain when and how pus forms, and account for its familiar properties and variable appearances. Mention factors that interfere with leukocyte function.
Describe the acute phase reaction and the physiology of the erythrocyte sedimentation rate. Give a short account of the "systemic inflammatory response" and mention why it's deadly.
Describe the role of mononuclear phagocytes in inflammation. Tell how and when granulomas form, and why they are important.
Give a good basic account of how tissues regenerate, injuries heal, and scars form. Given the name of a cell, tell whether it is labile, stable, or permanent, and why it matters. Explain how fibrosis forms in chronic inflammation. Describe how a fibrin meshwork is transformed into a fibrous scar. Distinguish healing by primary and secondary intention, and cite the factors that promote and oppose good wound healing.
Describe the activities of the following mediators of inflammation and/or healing, and when an activity is mentioned, remember which molecule or molecules mediates the effect:
bradykinin
C3a
C3b
C5a
histamine
IgE
interferon
interleukin 1
leukotrienes
membrane attack complex
platelet-derived growth factor
prostacyclin
prostaglandin E
serotonin
transforming growth factor β
thromboxane A2
Use each the following terms properly, and recall the term, given the definition:
abscess
acute inflammation
acute phase reaction
adhesion molecules
arachidonic acid
chemokinesis
chemotactic agent
chemotaxis
chronic inflammation
contact inhibition
degranulation
empyema
emigration
eosinophil
erosion
exuberant granulation
exudate
fibrin/fibrinous
fibrinogen
fibrous/fibrosis
free radicals
granulation tissue
granuloma
hyperemia
infection
inflammation
keloid
labile cell population
left shift
leukocyte
leukemoid reaction
leukocytosis
lymphocyte
lysosomes
macrophage (AKA...)
margination
myeloperoxidase
neutrophil
neutrophilia
opsonization
organization
permanent cell pop.
phagocytosis
plasma cell
pseudomembrane
purulent
pus
regeneration
resolution
scar
stable cell population
suppurate
transudate
ulcer
Describe how problems with inflammation cause or exacerbate the following illnesses:
Chediak-Higashi syndrome
chronic granulomatous disease
 Be sure you can recognize each of the following under the microscope:
Be sure you can recognize each of the following under the microscope:
edema (when obvious)
eosinophils
fibrin
giant cells (both types)
granulation tissue
granulomas
neutrophils
macrophages
mast cells (when stained)
plasma cells
pus
red cells
scar tissue
ulcers
Use and apply the common suffixes for surgical operations properly.
QUIZBANK
Inflammation (all)
Healing (all)
|
|
|
|
|
|
|
|
LEARN FIRST
Acute inflammation is a stereotyped response to recent or ongoing injury. Although the process is
complex, the principal features are dilatation and leaking of vessels, and involvement
of circulating
neutrophils.
You can recognize neutrophils in tissue sections by their segmented nuclei. Pus is neutrophils plus
liquefaction necrosis. Usually, the neutrophils themselves
caused most of the necrosis.
Chronic inflammation ("late-phase inflammation") is a response to prolonged problems, orchestrated
by T-helper lymphocytes. It may feature recruitment and activation of T- and B-lymphocytes,
macrophages, eosinophils, and/or fibroblasts. Again, the process is complex. You will recognize
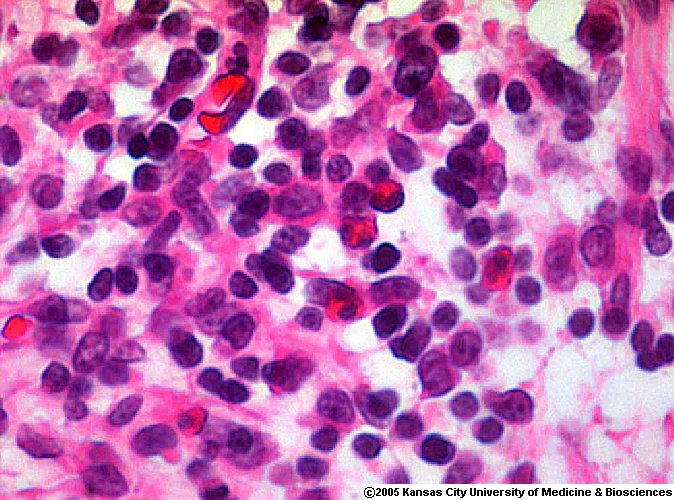
lymphocytes in tissue section by their small, "blue button" nuclei.
Granulomas are seen in certain chronic inflammation situations. They are clusters of macrophages
that have stuck tightly together, typically to wall something off. Such macrophages are called
epithelioid cells. You will recognize granulomas in tissue sections by their characteristic
appearance, or the presence of giant cells.
Fibrin is fibrinogen released from damaged vessels, and activated by the clotting cascades when
blood meets tissue juices. Fibrin forms the meshwork that controls bleeding, and then becomes the
framework for fibroblasts and angioblasts that will form the scar. Until the new scar is complete,
the whole meshwork of immature scar is called granulation tissue.
When the scar has matured, it contracts.
INTRODUCTION
War is the metaphor for inflammation. Both are necessary evils. Both are more-or-less
stereotyped responses to outside threats. There are specialized troops (white cells), including
suicide-commandos (neutrophils), long-term siege armies (granulomas), and many others. There are
supply routes (vessels), communications and intelligence (mediators), and a huge array of lethal
weapons (inflammatory enzymes). In war as in inflammation, there will be damage to both the
enemy and to friendly forces, and there will very likely be severe damage to the battlefield itself.
Despite idealistic rhetoric about "the laws of war", when the fighting starts, there is really only one
law for the soldiers: "Kill your enemy." Like it or not, if you want peace, you must be prepared to
fight under certain conditions. Like it or not, if you want to be healthy, your body must be able to
mount an inflammatory response. Force will always rule our world. Our best hope is that this will
be the force of good laws. And the best for which we can hope from the inflammatory response is
that, for most of our lives, it will do us more good than harm.
Probably your own death will be caused by your last
inflammatory response.
"Big Robbins" defines inflammation as "the reaction of vascularized living tissue to local injury".
Inflammation is the name given to the more-or-less stereotyped ways our tissues respond to noxious
stimuli, with blood vessels and white blood cells as its twin centerpieces and a host of proteins as
actors. Inflammation "destroys, dilutes, or walls off the injurious agent" and sets in motion the
limited powers of the body to heal itself. Inflammation and repair can and do themselves damage
the body.
Strictly speaking, "immunity" is all the things the body does in defense against invaders (growing
skin, making neutrophils, etc., etc.) As used today, the unmodified word
immunity refers
to the activities of B ("humoral immunity") and T ("cellular immunity") lymphocytes.
Beginning medical students have a tendency to equate "inflammation" and infection, at least
unconsciously. This is plain wrong. Several infectious diseases feature no inflammation
(Creutzfeldt-Jacob disease, yellow fever, and many of the opportunistic infections in AIDS are only
three examples.) Noxious, non-infectious things that produce inflammation include trauma,
radiation injury, various poisons, chemical or thermal burns, tissue necrosis itself (except
apoptosis),
and any of the four major types of immunologic injury. (You'll learn about all of these soon
enough.) A sunburn or a red scratch are inflammation, just like mosquito bites, pimples, plague and
leprosy.
Obviously, there are differences among inflammatory reactions. Acute inflammation is almost
completely stereotyped -- over minutes to a few days, blood vessels dilate and leak, and neutrophils
enter the surrounding tissues. Chronic inflammation is more variable, with variable participation by
lymphocytes, plasma cells, macrophages, and healing cells (fibroblasts and angioblasts).
Whole body inflammation, formerly a popular term used especially
by surgeons for the patients who they could not save, is going out of fashion
in favor of multiple organ failure. Whatever you call it,
in super-sick people, various cytokines increase tremendously in the bloodstream;
this situation interacts with ischemia, free radical production, and leakage
of heatshock proteins from cells to create a vicious downward cycle into
irreversible shock. See
JAMA 271: 226, 1994; Surg. Clin. N.A. 80: 885, 2000;
Crit. Care Med. 28:
537, 2000; Crit. Care Med. 29(7S): S-99, 2001.
"Subacute inflammation"
does not describe a distinct pattern.
We suggest that you first try to understand inflammation at the light microscopic level. You are
already acquainted with fibrinogen and fibrin. Only when you have a clear picture of acute
inflammation, chronic inflammation, and wound repair should you go back and learn the host of
molecular mediators that derive from cells and plasma. All those mediators: J. Allerg.
Clin. Imm. 103: S-378, 1999; or if you really want to go deep,
J. Allerg. Clin. Imm. 106: 817, 2000.
Still deeper: The genes / proteins that modulate the inflammatory response:
Nature 420: 846, 2002.
Dozens are known, each has an associated clinical syndrome in patients
bearng mutations, and each is a potential target for therapy.
The suffix that indicates inflammation is "-itis" (the plural is "-itides". Philologists: "-osis" means
"full of".)
* The public recognizes inflammation, and the words "inflame" and "inflammatory" have found their
way into journalism and law.
Terms for abnormal accumulations of fluid: A transudate is protein-poor salt water squeezed
through blood vessels by hydrostatic pressure, i.e., it has specific gravity of extracellular fluid, 1.010
or thereabouts. An exudate is an abnormal, protein-rich fluid that has leaked out of inflamed
vessels.
A body fluid (either an exudate or an area of liquefaction necrosis) containing neutrophilic
leukocytes and necrotic debris is pus. The preferred adjective to describe things with lots of pus is
purulent. To produce pus is to suppurate. Pus that literally fills an important body cavity is
called an empyema. (This is most common in the pleural cavities.) If you've got a lot of pus, you
need it drained by a surgeon. Pus requires no description, but it is worth mentioning at this point that is not always the same color
or thickness. Pus always has a yellow-green tinge because of myeloperoxidase. Classic yellow pus
(as in a staphylococcal boil) also includes some lipid from necrotic tissue. Without necrosis (as in a
streptococcal phlegmon), pus is more yellow-gray. Pseudomonas bacteria make a dye that
imparts a blue-green fluorescence to pus.
{26419} normal neutrophil in a smear; finely granular
cytoplasm and segmented, dark nucleus
Increased interstitial fluid is called edema.
HISTORICAL HIGHLIGHTS: "Big Robbins" lists, or might have listed....
Cornelius Celsus (ancient Rome) described rubor (redness), calor (heat -- this applies only to the
skin), dolor (pain), and tumor (which then simply meant "swelling") as the "cardinal signs of
inflammation".
John Hunter (the great early surgeon, * 1793, * parodied by William Blake as "Jack Tearguts") first
characterized inflammation as a nonspecific body response.
Rudolf Virchow added functio laesa (loss of function) as the fifth cardinal sign of inflammation, and
his student, Julius Cohnheim, provided the basic studies of the pathologic microanatomy of
inflammation.
Elie Metchnikoff (* 1892) was the first to observe and study phagocytosis. (* This is the same
Metchnikoff who popularized yogurt as a "health and longevity food". He died at age 70.)
Paul Ehrlich developed the idea of humoral immunity early in the 20th century. (This is the same
Ehrlich who developed the "magic bullet" for syphilis, and most of the stains we still use.)
Thomas Lewis demonstrated that inflammation is brought about by chemical mediators, most of
which act locally. Someone may still ask you about the "triple response of Lewis" to a superficial
scratch (after the momentary vasoconstriction): (1) a red scratch mark; (2) then a red flare around the scratch mark; (3) then a red
swollen area ("wheal") around the flare. (Try it!) Dr. Lewis found that he could eliminate the flare,
but not the others, by cutting the autonomic nerve supply (i.e., preventing the "axon reflex"). This
experiment led to the discovery of histamine, which mediates events 1 and 3.
ACUTE INFLAMMATION: A stereotyped response to most kinds of noxious stimuli. Something a
part of the body does when it knows it's been hurt.
* Mega-review: Med. Clin. N.A. 81: 1, 1997.
Textbooks describe "acute inflammation" as lasting from moments to a maximum of 1-2 days. This
is a simplification, as anyone with a persistent pimple knows. (* Your handout author
has lots of experience with this.)
The hallmarks of acute inflammation are (1) vasodilatation and increased
vascular permeability; (2) entry of neutrophils into the tissues.
The first event is transient arteriolar constriction, lasting a few seconds (if at all; scratch yourself and
see) up to a few minutes (after a trivial burn -- you have probably noticed it takes a while for a
minor burn to turn red.) This vasoconstriction helps control blood loss in case vessels have been
severed.
When the arteriolar constriction phase is over, the arterioles dilate and stay dilated as long as acute
inflammation continues. This produces the redness and (since heart's blood is warmer than exposed
body parts) the sensation of heat. The slightly increased pressure that this causes in the capillaries
may produce some transudation of fluid into the tissue spaces.
Hyperemia is a generic term for extra blood in an organ due to dilation of the arterioles. More about
this soon.
Soon after injury, the small vessels (mostly the venules 20-60 microns)
become permeable to some or all plasma proteins. This increases the osmotic ("oncotic") pressure of
the interstitial fluid, water is drawn out of the vessels, and inflammatory edema ("swelling") results.
As protein leaks out into the interstitial spaces, the local concentration of cells in the blood increases.
Red cells pack small vessels ("red cell
stasis"), neutrophils stick to endothelium, and the viscous blood flows more
slowly ("stasis"). The water that follows the protein out of the vessels contributes to edema.
Much of this fluid will return to the circulation only via the lymphatics.
The physicochemical changes that cause the increased permeability to protein are only partly
understood. The key seems to be opening gaps in the intercellular junctions ("endothelial cell
contraction"). Another factor seems to be loss of various polyanions from the basement membrane
surrounding the endothelial cells. Of course, if the vessels are damaged by the first injury, or by the
neutrophils, or are themselves regenerating, they will leak.
The worse the injury, the larger the protein molecules that can pass through the vessel walls. In the
worst injuries (and, of course, if the vessel is severed), fibrinogen escapes into the tissue fluids, and
under these circumstances is certain to be transformed to fibrin (by your
clotting cascade, of course).
Of course, the fibrin controls bleeding and provides a mechanical barrier. If needed, it will also
serve as the framework while the new scar tissue will be laid down. Students often confuse fibrin
and collagen. "The difference between fibrin and collagen is the difference between a scab and a
scar." NOTE: When unqualified, the word fibrous means "composed of type I collagen". Fibrinous
always means "composed of fibrin".
{10901} gonorrheal salpingitis; note tremendous swelling and redness of both oviducts
Experimentalists use colloidal carbon (i.e., fine-grain India ink) to demonstrate the increased
vascular permeability. In the lab, there are three separate phases of vessel leakage:
(1) The familiar immediate-transient response begins at once, peaks at 5-10 minutes, and is over by
30 minutes. It involves only the venules, involves contraction and separation of endothelial cells,
and is attributed to prostaglandins, histamine, serotonin and a host of other chemical mediators.
(2)
The more persistent, equally-familiar immediate-sustained reaction ("immediate prolonged") is seen
only when the injury is severe enough to cause direct endothelial cell damage, and persists until
thrombosis or regeneration ends it. Obviously this can affect any blood vessel.
(3)
The delayed-prolonged leakage phenomenon is seen only after hours or days. Venules and
capillaries exude protein, again because their junctions separate. (Other
vessels' walls are too thick to exude much protein.)
The prototype is the swelling that
accompanies a sunburn, radiation therapy, and all but the worst thermal burns. Long-mysterious,
we now know that the underlying mechanism is apoptosis of the endothelial cells.
(4) White cells do some damage "just passing through".
(5) And of course new blood vessels (young scar, or cancers) are leaky.
The final key event in acute inflammation is the accumulation of neutrophils ("polys", "segs";
nobody calls them * "microphages" nowadays) in the injured tissue. (Most of the time, these
predominate for the first 24-48 hours after injury, and are more or less replaced by macrophages
after this time.)
The laws of physics cause neutrophils to marginate ("pavement", i.e., lie along the inner walls of
vessels) whenever blood flow is slowed. They roll along for a while.
Adhesion to the walls of vessels, especially venules, results
when leukocyte adhesion molecules on the surface of the neutrophils interact with endothelial
adhesion molecules on the endothelial cells.
Leukocyte adhesion molecules go by names such as LFA-1 and MO-1. These are members of a
homologous set.,
* LAD I: Lack a CD11b/CD18 integrin; LAD II: lack the selectin-binding Lewis X glycoprotein.
Newer variants Blood 97: 767, 2001.
Endothelial adhesion molecules include ELAM-1 (for neutrophils)
and ICAM-1 (for neutrophils, lymphs, and monos). Various mediator proteins increase the numbers
of some or all of these.
* Stay tuned: Pain itself (i.e., stimulation of pain fibers) causes the local
neutrophils to lose their ability to express
L-selectin adhesion molecules. This seems to be one
mechanism of feedback that limits the acute inflammatory response
(Nat. Med. 5: 1057, 1999).
* Stay tuned: Specific inhibitor of selectin (efomycine M and its family)
as anti-inflammatories: Nat. Med. 8: 366, 2002. Watch this especially for psoriasis.
Emigration ("diapedesis")
of neutrophils from the vessels into the tissues occurs when the cells squeeze through the
widened endothelial cell gaps, then get through the basement membrane
by digesting it with enzymes. (Of course this damages the blood
vessels, but the endothelial cells repair the damage soon enough.)
The other white
cells also leave vessels by this route.
Various chemical mediators cause chemokinesis (increased random locomotion) and chemotaxis
(directional migration) of neutrophils and other cells. Chemotactic agents include a plethora of
bacterial breakdown products, complement components (remember C5a), and leukotriene B4. Most
small molecules that are chemotactic for neutrophils are also chemotactic for macrophages and
vice versa.
Chemotactic factors act on the cell membrane, signalling a poorly-understood process involving the
microskeleton (remember calmodulin, the calcium-binding protein that polymerizes myosin, as a
key player here) that eventually results in cell movement.
Certain lymphokines (factors produced by lymphocytes) and monokines (factors produced by
monocytes / macrophages) are chemotactic for neutrophils and/or other white cells. Mast cells,
activated in parasitic infestations and classic IgE-mediated allergy, release "eosinophilic chemotactic
factor of anaphylaxis".
* Someone may ask you about key enzymes in the production of prostaglandins and leukotrienes.
"Phospholipase A" releases arachidonic acid from a host of biologic membranes and is inhibited by
glucocorticoids. "Cyclo-oxygenase" turns arachidonic acid into prostaglandins and is inhibited by
aspirin. "5-lipo-oxygenase" turns arachidonic acid into leukotrienes.
Once they have found their way to the tissues, the neutrophils phagocytize things that shouldn't be
there. They also degranulate, releasing enzymes into the interstitial fluid.
Phagocytosis requires that the particle be recognized and attach to the neutrophil. Most particles
must be coated (opsonized) by IgG (subtypes 1 or 3) or C3b. There are receptors for both on the
neutrophil surface. The particle will then be engulfed and a lysosome membrane fused with the
phagosome membrane, causing digestion within the phagolysosome. (If only C3b is present in the
opsonin, additional molecules will be required to trigger engulfment.) Some of the lysosomal
enzymes will leak out of the neutrophil and into the intercellular fluid.
Killing of phagocytized bacteria is mediated through the H2O2-myeloperoxidase-halide
system and
other, less-effective oxygen-dependent and oxygen-independent systems.
Exactly how this happens is still under investigation
(see for example a claim based on generating charge differentials
across membranes in Ann. Rev. Immuno 23: 197, 2005).
(We retain ancient
microbe-killing proteins including lysozyme and lactoferrin.)
Neutrophil products, including lysosomal enzymes, H2O2, free radicals, and
arachidonic acid
metabolites are released during the process by "regurgitation during feeding", "frustrated
phagocytosis" (i.e., the neutrophil tries to eat something too big, such as a huge immune complex or
a splinter; it can't engulf it so it drools), and "cytotoxic release". The latter is a euphemism for stuff leaking out of dead
cells.
Notable exceptions to the "neutrophils first, monocytes later" rule: (2) In classic allergy and in some parasitic
infections, eosinophils dominate from start to finish; (3) In typhoid fever, the predominant cells are
always the macrophages; (4) In most forms of acute dermatitis, lymphocytes are most abundant;
(5) In clostridial gas gangrene, don't expect to see any white cells; (6) In many kinds of bacterial
infections (including chlamydial ones), there are few or no other cells besides the neutrophils.
Here's something to help you appreciate neutrophils and what they do to normal
tissue. You know that after you've had a cold and runny nose for a few days,
the skin at the inner edge of your nostril becomes cracked and sore; this is the
effect of enzymes from the neutrophils that have responded to the viral tissue
injury. By contrast, in a runny nose from hay fever, there are no neutrophils,
hence to injured skin on your nose.
Neutrophil defects worth learning now:
1.
Insufficient circulating neutrophils ("neutropenia"; "agranulocytosis"), as in radiation injury, cancer
therapy, drug sensitivity
2.
Neutrophil adherence molecule defects, due to heredity,
glucocorticoid administration, diabetes, or ethanol in the bloodstream.
3.
Failure of neutrophils to move properly (notably in diabetes) or to respond to chemotactic stimuli
4. Failure of neutrophils to phagocytize (diabetics, people with complement or immunoglobulin
deficiencies)
5.
Defective microbial killing. This may be due to
6.
Mixed defects. Remember that diabetes and glucocorticoids interfere with most white blood cell
functions. In Chediak-Higashi syndrome (a problem with membrane synthesis), there are too few
neutrophils, they do not respond properly to chemotactic stimuli, and their (abnormally large)
lysosomes fail to fuse with phagosomes.
Future nuclear medicine experts: Tc99 ("technetium 99")
is taken up by neutrophils. This is a great way to "light up"
hidden abscesses.
Unless the injury is trivial, mediators produced by other cells will cause increased production and
early release of neutrophils from the bone marrow. Increased neutrophils in the blood stream is
neutrophilia (or, sloppy, "leukocytosis"), and the presence of young neutrophils ("bands", etc.) is
called a left shift, after the column positions on the old hematologists' counting pad. You'll learn
later how to tell real leukemia from a severe inflammatory response (leukemoid reaction).
{26191} mature neutrophils
Viral infections, and certain unusual bacterial infections (typhoid, rickettsial disease) produce a
neutropenia instead. You may see the same thing in an overwhelming infection.
Once acute inflammation has begun, there are four possible outcomes:
1.
Complete resolution, i.e., there has been no damage to the connective tissue framework or non-recoverable cells of any
part of the body.
2.
Healing by scarring (see below)
3.
Abscess formation. Pus in a confined space is called an "abscess". As proteases continue to work on
the fluid itself, the osmotic pressure within the abscess becomes greater and greater, causing it to
swell ("ripen" -- ever had a pimple?) While the body might succeed in walling it off, usually you
still have to drain pus.
4.
Progression to chronic inflammation (see below). This happens when, and only when, the
neutrophils and their fast-acting molecular allies cannot remove the noxious agent.
MONONUCLEAR PHAGOCYTES
This is a generic term for blood monocytes and the cells to which they give rise. They are important
in acute inflammation, as well as being a key element in chronic inflammation. Much of what you
have just learned about neutrophils is equally applicable to monocytes.
{26440} monocyte in smear; most monocytes you see
will not have such good vacuoles
Like neutrophils, monocytes bear Fc and C3b receptors on their surfaces, in order to recognize
opsonized materials for phagocytosis, and they will also engulf other kinds of particles. In addition
to their famous role as scavengers, these cells ("all derived from the circulating blood monocyte")
perform a host of other functions. Lone mononuclear phagocytes in the tissues are macrophages
("histiocytes", "dirt-bags", etc.), and may be fixed or mobile (but never so speedy as neutrophils).
Certain factors (notably gamma interferon from T-cells) make macrophages angry ("activated"),
increasing their ability to kill any organisms they have devoured, and sometimes causing the
macrophages themselves to adhere to form "granulomas" (see below). Other factors (notably
transforming growth factor β,
also called "activin") de-activate them. Macrophages themselves
generate a host of biological molecules.
* Macrophages that harbor many intracellular pathogens take on the appearance of "foam cells",
just as if they had eaten lots of free fat. We'll see these in leprosy, leishmaniasis, rhinoscleroma,
malakoplakia, and xanthogranulomatous pyelonephritis.
ACUTE INFLAMMATORY MEDIATORS
You will find yourself overwhelmed if you try to learn all the effects of the chemical mediators of
inflammation. This section includes items that are worth knowing for medical undergraduates.
Vasoactive amines include histamine and serotonin, the classic mediators of immediate vascular
permeability.
Histamine is immediately available from our mast cells. (Serotonin is found in rat mast cells.)
These amines are released by trauma, cold, binding of antigen to the IgE on the mast cell surface,
C3a and C5a, interleukin-1, and a host of histamine releasing factors from other white cells.
Histamine and serotonin are also released form our platelets ("the platelet release reaction").
Pharmacologists and clinicians: H1 receptors mediate the effects of histamine in inflammation.
The complement system is a group of 20 plasma proteins that are activated in cascades by the
classic or alternate pathways (don't worry about the details now, just remember that the alternate
pathway bypasses C4) or individually. Antigen-antibody complexes, dead tissue, and even plasmin
activate ("fix") complement. Perennial test-bank items:
C3a and C5a ("the anaphylatoxins") increase vascular permeability, at least in part by releasing
histamine from mast cells. C5a also liberates various chemotactic and noxious factors (notably
arachidonic acid metabolites) from neutrophils and macrophages.
C3b is the great opsonin of the complement system.
C5b-9 is the membrane attack complex, which punches holes in membranes of both friend and foe.
The kinin system is another group of proteins, which ultimately produce the nonapeptide bradykinin.
Bradykinin increases vascular permeability, dilates blood vessels, contracts non-vascular smooth
muscle, and causes pain. (Remember the last -- bee venom is largely bradykinin.)
* Kallikrein, another factor in the system, is chemotactic for neutrophils, and both activates and is
activated by factor XII. Don't worry about the pathways of activation for these substances.
The clotting system is a third system of proteins that you know. For now, just remember that
activating the intrinsic pathway at its origin (factor XII) is one way to activate the kinin system, and
that plasmin activates C3.
* Discussions of these cascades often make clotting factor XII ("Hageman factor") seem utterly
central to the body's defenses. However, the real Mr. Hageman, who lacked the factor named for
him, seemed none the worse for his deficiency -- he only learned late in life that his blood would not
clot in a glass tube.
Prostaglandins: products of the cyclooxygenase pathway of arachidonic acid metabolism.
(Review:
The pathways in "Big Robbins", including the names of enzymes, are
USMLE I pathology favorites.) Worth remembering:
Thromboxane A2 (TXA2), from platelets, aggregates platelets, constricts blood vessels. Great
for
hemostasis.
* Thromboxane probably causes the cough due to the popular ACE-inhibitor antihypertensives
(Lancet 350: 3, 1997). Stay tuned for picotamide, the thromboxane inhibitor,
which may someday come into use for various vascular diseases.
Prostacyclin (PGI2), from the vessel wall, prevents platelet aggregation, dilates vessels. Great for
whenever hemostasis is unnecessary.
Prostaglandin E (PGE) is also a potent vasodilator (probably the most important one), greatly
potentiates the ability of bradykinin to cause pain, and seems to be the local mediator of fever
production for the hypothalamus. Both PGE and prostacyclin potentiate permeability-increasing
and chemotactic mediators.
Other prostaglandins exert a host of effects.
Aspirin, the non-steroidal anti-inflammatory drugs, and glucocorticoids inhibit cyclooxygenase,
preventing the formation of the whole family.
Leukotrienes: products of the lipooxygenase pathway of arachidonic acid metabolism. They are
produced by all of the inflammatory cells except lymphocytes. Formerly
called SRS or slow-reacting substance(s). Review:
J. Imm. 174: 589, 2005. Worth
remembering:
Leukotrienes C4 and its products D4, and E4 increase vascular permeability
and constrict smooth muscle, and leukotriene
B4 makes polys adhere
to endothelium and is a potent chemotactic agent.
Diets rich in omega-3 fatty acids prevent production of leukotrienes (and, to a lesser extent,
prostaglandins). Leukotriene receptor antagonists may someday be a part of the regular drugs used
by clinicians; so may inhibitors of leukotriene synthesis (Arth. Rheum. 39: 515, 1996).
Term: prostaglandins and leukotrienes are examples of autocoids, i.e., short-range, locally-active
hormones.
Lysosomal constituents:
We have already seen that neutrophils release the contents of their granules during inflammation.
For now, remember these neutrophils proteins:
Remember that monocytes produce acid hydrolases, collagenase, and elastase. Eosinophil specific
granules contain several cationic proteins that seem to help fight the larger parasites.
Regardless of their sources, the proteases and free radicals released from inflammatory cells are can
and do harm the body's own tissues. For reviews, see Hum. Path. 16: 973, 1985; NEJM 320: 365,
1989; Neth. J. Med. 36: 89, 1990. Havoc wrought by free radicals: J. Royal Coll. Phys. 23: 221,
1989; specifically by neutrophil free radicals: Am. J. Path. 139: 1009, 1991.
The inflammatory response is often excessive. This is why, for example, it's probably best to put
cold, rather than heat, on athletic and other minor injuries throughout the time they're healing.
(* Tip from my best D.O. sports medicine consultant.)
The body has several proteins (notably α1-antitrypsin inhibitor, also known as
"α1-protease inhibitor") to prevent them
from ruining our own tissues while we are still young. Remember that
H2O2 and free radicals are also released from neutrophils and macrophages.
Platelet activating factor, a small molecule, is generated on demand by various cells. Its various
contributions to inflammation are only now being worked out
(activates neutrophils and platelets, constricts smooth muscle, recruits and
degranulates eosinophils), but the total effect is massive (Nature
374: 501, 1995). It is important because a new class of anti-PAF agents is under investigation.
Nitric oxide: Dilates vessels locally (very fast), helps kill bacteria over the following several days,
and has goodness-knows-how-many other effects: Hosp. Pract. 31: 69, 1996.
Cytokines are polypeptide mediators made by lymphocytes
("lymphokines") and macrophages ("monokines"). Long familiar from immunology, it is now clear
that they modulate the acute inflammatory response as well. Don't worry about the details in "Big
Robbins".
The monokines interleukin-1
and tumor necrosis factor α ("cachectin" or "TNF-α")
are key actors in the acute phase reaction,
part of "just being sick" with an inflammatory illness.
During the acute phase reaction, there is somnolence, poor appetite, increased production and early
release of neutrophils, and altered rates of hepatic synthesis of most of the major plasma proteins
(albumin and transferrin go down; α1-antitrypsin inhibitor, serum amyloid-associated
protein, the
complement components, fibrinogen, haptoglobin, and the atavistic (?) C-reactive protein go up.)
* The acute phase reaction can be induced by the physical and psychological distress of military
school hazing: Am. J. Clin. Nut. 53: 126, 1991. This is probably important new knowledge.
* CD16, the marker for the acute phase reaction: Am. J. Clin. Path. 107: 187, 1997.
* Interleukin 6 is up and down by the end of the first day after uncomplicated surgery.
C-reactive protein is up and down by two days. Fibrinogen rises more slowly
and is back down by 8 days or so.
The change in levels of plasma proteins is responsible for the increased red cell sedimentation rate,
described by Hippocrates and still used to monitor the course of inflammation.
* The lymphokine lymphotoxin ("tumor necrosis
factor β") has not received much
attention in the past decade.
The systemic inflammatory response ("total-body inflammation") represents toxicity from excessive
production of the cytokines and/or other white-cell products.
Venous return to the heart (i.e., venous responsivity) is compromised, perhaps myocardial function
is depressed, etc., etc., etc., etc., etc.
When it is caused by bacterial infection of the bloodstream, it's called sepsis.
* Deltibant ("Bradycor"), an anti-bradykinin antagonist, seems to improve survival in sepsis: JAMA 482: 277,
1997; neuroprotection J. Neurotrauma 16: 431, 1999.
CHRONIC INFLAMMATION
The hallmark of chronic inflammation is infiltration of tissue with mononuclear inflammatory cells
("mononuclear cells", "round cells", i.e., monocytes, lymphocytes, and/or plasma cells). Generally,
good tissue has been (and is being) destroyed, and there will be some evidence of healing (scarring,
fibroblast proliferation, angioblast proliferation).
{10973} lymphocytes and plasma cells in chronic inflammation
In clinically significant disease, we believe that the tissue macrophages are almost all recruited
directly from the bloodstream monocytes. Plasma cells produce antibodies against the persistent
antigen or the altered tissue components. Lymphocytes are likely to be present even where there is
no involvement of the immune system.
Plasma cells appear in chronic inflammation as a result of T-helper cells
activating B-lymphocytes. Interleukin 1 causes the B-cells to divide.
The transformation into plasma cells
is mediated (at least in part) by interleukin 4.
If IgE or worms are involved, you will probably see eosinophils. Their granules
contains several alkaline ("basic") proteins that are noxious to worms. (These are now targets for
specific therapies: J. Allerg. Clin. Imm. 113: 3, 2004).
You may also see some
neutrophils.
{14708}
eosinophil in smear
* Review of the harm mediated by chronic inflammation: J. Allerg. Clin. Imm. 98: S-291, 1996.
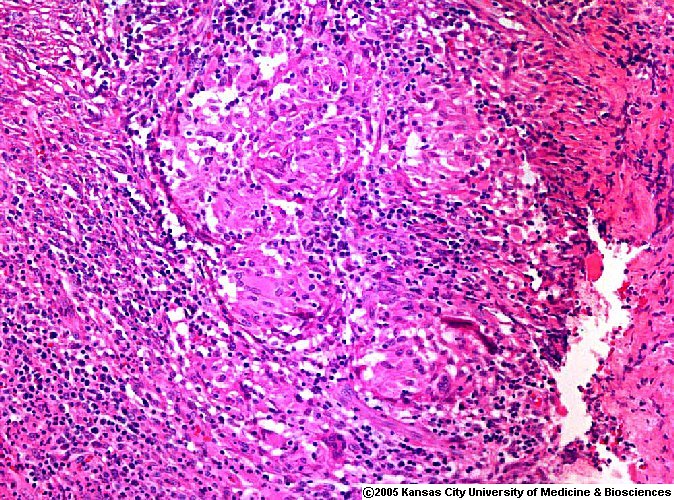
Granulomatous inflammation is a special kind of chronic
inflammation that occurs in the presence of indigestible material and/or cell-mediated immunity
("type IV hypersensitivity"; more about this in a few days). Ignore the definitions offered in textbooks.
A granuloma is an abnormal structure built from at least two activated macrophages adhering to one
another. Such macrophages are (confusingly) called epithelioid cells. Granulomas serve to wall off
stuff (splinters, the caseous debris of TB, etc., etc.)
In the absence of a very large foreign body, a granuloma will almost always contain at least a few T-lymphocytes (though this
is not absolutely mandatory).
The cells in a granuloma are activated by gamma-interferon (and/or α-TNF or whatever).
However, not all activated macrophages stick together. The current best candidate for "granuloma
glue" is osteopontin (Proc. Nat. Acad. Sci. 94: 6456, 1997;
Science 287: 860, 2000; update Am. J. Path. 164: 567, 2004).
Whatever makes them the way they are, granulomas vanish as soon as the disease is effectively
treated.
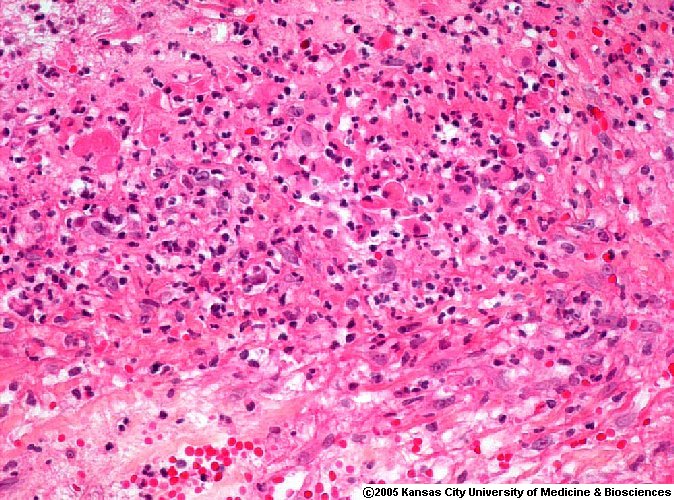
You must learn to recognize granulomas. Epithelioid cells have abundant pink cytoplasm, indistinct
borders, and elongated, euchromatin-rich, reticulated nuclei oriented helter-skelter. My favorite
gestalt: blue rice-crispies (nuclei) scattered on a frayed, pink tablecloth (cytoplasm).
{17629} granulomas in the lung
Granulomas can (but need not) contain syncytial giant cells
(polykaryons). These fused clusters of epithelioid cells
take a week to form. For our purposes, there are two kinds. Langhans giant cells have their
nuclei arranged in a horseshoe around the edge, and foreign body giant cells, with nuclei dispersed
more or less evenly. The distinction is of no known significance.
{17628} epithelioid giant cell
The giant cells of granulomas occasionally contained altered cytoskeletal components in the shapes
of stars, or asteroid bodies. They are pretty, but of no known significance. Or you may see
laminated calcified nuggets, called Schaumann bodies (* "conchoid bodies"), also of no known
significance.
{25626} asteroid bodies in giant cells
The classic granulomatous diseases include tuberculosis, leprosy, foreign body reactions
(* including the reactions to everything from sutures to schistosome eggs), the deep fungal
infections, berylliosis, and the mysterious disease "sarcoidosis". * "Big Robbins" lists syphilis
(the granulomas, if any, are small and loose) and
silicosis (the granulomas, if any, are very fibrous). {10958} tuberculosis, good caseous granuloma
* Future pathologists: Here is a reasonably complete catalogue of the granulomatous diseases.
Granulomas with suppuration (i.e., with pus in their centers; "stellate microabscesses") are typical of
those bacterial diseases with a propensity to involve lymph nodes. These are lymphogranuloma
venereum, cat scratch fever, brucellosis, plague, tularemia, glanders-melioidosis, listeria, campylobacter,
and
yersinia infection. In the central midwest, don't forget blastomycosis.
{23386} lymphogranuloma venereum
Granulomas with caseation are typical of certain fungal infections (histoplasmosis, blastomycosis,
and coccidioidomycosis, as above) and of mycobacterial ("fungus-like bacteria") infections
(basically TB; also remember BCG bacillus, leprosy, and "atypical mycobacteria").
Granulomas with foreign bodies: aspirated food, schistosome eggs, toxocara, silicone injections,
splinters, sutures, windshield fragments, chalazions, ruptured epidermoid cysts, sea urchin spines,
mucus plugs in cystic fibrosis,
nitrogen bubbles ("pneumatosis"; "tissue emphysema"),
amyloidomas, dead aspergillus fungi, dead filaria, ingrown hairs, talc in the lungs, metastatic
calcification bits, uric acid crystals (in longstanding gout, of course; these are "tophi"), sclerosing
lipogranuloma of the penis (J. Urol. 133: 1046, 1985, a fun article),
insect bites, "actinic
elastolytic granuloma of Mieschler" (a foreign body reaction to your
own elastic fibers), etc., etc.
Ruptured silicone breast implants produce aggregates of foamy macrophages (like macrophages
loaded with lipid or mucin) but not good granulomas (Am. J. Clin. Path. 107: 236, 1997).
Other solid granulomas invite subclassification as immunologic diseases:
Straightforward immune problems: The organic pneumoconioses, berylliosis, zirconium disease (the
infamous "armpit sarcoidosis", from zirconium-based deodorants), positive skin tests
More arcane immune problems: Wegener's granulomatosis (and its variants Churg-Strauss and
lethal midline granuloma)
Immunologic reactions to tumors: Lennert's lymphoma, seminoma (both are often rich in
granulomas); lymph nodes draining other cancers
Mysterious immune problems: sarcoidosis, Crohn's disease, primary biliary cirrhosis, bronchocentric
granulomatosis
Neutrophil deficiency syndromes: notably "chronic granulomatous disease"
Toxoplasmosis and Q-fever (curious little granulomas) and cutaneous leishmaniasis ("foamy
granulomas", present if immune response is good). Baboon amoebas (don't worry
about them just now: Lancet 362: 220, 2004), and CNS amoebas in the immunocompromised
HIV encephalitis presents groups of giant cells,
the result of macrophages recognizing HIV protein on
each others' surfaces
Scarring means laying-down of dense (type I) collagen in chronic inflammation and/or wound
healing (see below; brain makes its scars out of glial filaments instead). Usually, when there is
chronic inflammation of any time, some dense collagenous scar gets laid down.
Right now, transforming growth factor β
gets most of the credit (blame) for causing fibrosis in
chronic inflammation. Interleukin 1, from macrophages, is also a potent activator of fibroblasts.
This probably accounts for part of the scarring in chronic inflammatory diseases.
An ulcer (* "ulceration", for those who prefer nouns made from verbs made from nouns) forms when
necrosis has involved a body surface and a portion of it is sloughed. Further, there must be necrosis
of both the epithelium and at least some of the underlying connective tissue.
Note that any definition of an ulcer must exclude paper cuts (i.e., breaks in surfaces without
necrosis) and unroofed friction blisters (i.e., loss of epithelium without loss of connective tissue.)
Ulcers are discussed here by "Big Robbins" because they are always inflamed.
We've seen pictures of ulcers when we discussed necrosis. Please note that the familiar, banal
decubitus ulcer of pressure points results from ischemic necrosis. (Do you understand how?)
A little-known fact is that decubiti of the colonic and rectal mucosa from fecal impaction are
common, and can be the portal of entry for bacteria. These are called "stercoral" or "stercoraceous"
ulcers, and they can easily kill a person.
{10461} duodenal ulcer (stomach is at top)
A pseudomembrane results when the upper portion of a mucosal surface undergoes necrosis, freeing
fibrinogen from vessels that then clots along the surface. A pseudomembrane is actually a very
large, very shallow ulcer. The best pseudomembranes include secretory product from the underlying
glands as well.
{10529} pseudomembranous enterocolitis
NOTE: Very confusing to students is sloppy use
of the term "chronic inflammation" for scarring left over
from acute inflammation that resolved long ago. "Chronic pyelonephritis", "chronic pancreatitis",
and "chronic pericarditis" are generally misnomers.
Ignore old-fashioned discussions of "serous",
"fibrinous", "hemorrhagic", "suppurative" and "purulent" inflammation. Remember that really
severe inflammation will allow fibrinogen out of the vessels. Catarrh is an archaic word for an
exudate, or for heavy secretion from an inflamed mucous membrane.
* In the future, look for much more about mediators in inflammation produced by epithelium and
fibroblasts, especially as causes of "idiopathic" diseases in which chronic inflammation figures
prominently. REGENERATION
Inflammation is said to resolve when no structural cells have been lost after the inflammatory
process is complete and phagocytosis has cleaned up the area. When the tissue has been damaged
during the inflammatory process or in other ways, but the body itself is still alive, the tissue will
either regenerate or be repaired by fibrous tissue. If none of the latter is required, the word
"resolution" is also appropriate. If any repair by fibrous tissue occurs, there will be a scar.
(Depending on the site, scar tissue may be called "cicatrix", "fibrosis", "adhesions", "gliosis",
"fibroplasia", etc., etc.)
Labile cells ("continuous replicators") are constantly replenishing their neighbors that have died or
been shed. Examples include the epithelium of skin, mucous membranes, oviducts, ducts;
urothelium; endometrium; seminiferous tubules; bone marrow; lymphoid tissue.
Probably these cells would "like to" proliferate all the time, but are stopped by "contact inhibition"
by their neighbors. More about this arcane subject when we talk about cancer....
Epidermis can regenerate from the skin adnexal structures (hair follicles, sebaceous glands, sweat
glands), enabling full removal of epidermis as for a skin graft.
Stable cells ("discontinuous replicators") can proliferate rapidly in response to need, especially when
required to replace lost neighbors. These include all glandular parenchymal cells, as well as
fibroblasts, endothelial cells (cuboidal, and called "angioblasts", when they are healing), smooth
muscle cells, osteoblasts, and chondroblasts.
Cartilage and tendon heal very poorly, since nothing will restore their specialized structure. Smooth
muscle cells regenerate poorly. Otherwise, provided a scaffolding of fibrous tissue is available (i.e.,
the collagen framework in an area has not been totally wrecked), a few of these cells can regenerate
the organ.
The champion healer is the liver. For one thing, it's almost impossible to destroy its connective
tissue framework in the short-term.
Permanent cells ("non-replicators") cannot undergo mitosis or be replenished after birth. These cells
include glia, neurons, and cardiac (non-failing heart)
and (maybe) skeletal muscle cells. (Plasma cells and other
mature products of marrow are post-mitotic too, but can be replenished. Nerve cell processes have
some ability to regenerate, and there are reserve cells that can replace a lost portion of a skeletal
muscle fiber.)
* The regenerative ability of the myocardial cell: Lancet 363: 1306, 2004.
Maybe someday this will be clinically useful.
Obviously, cells will not regenerate if there is inadequate blood supply, inadequate nutrition, or
complete destruction of their connective tissue framework.
* Someone will tell you, "The more specialized the tissue, the less its powers of regeneration." This
isn't true. Liver regenerates, and belly button doesn't.
A few hours after injury, there is already evidence of connective tissue repair. Fibroblasts become
active and begin to proliferate, and buds ("angioblasts") sprout from the damaged capillaries. Of
course, the cells will show lots of euchromatin, large nucleoli, and abundant basophilic cytoplasm.
Typically, both kinds of cells invade the fibrin meshwork created during the injury and
inflammatory response.
The fibroblasts produce ground substance, fibronectin, and type III collagen;
later they will produce type I collagen for the mature scar.
The young vessels are leaky, so healing wounds are edematous both grossly and microscopically.
The fibroblasts lay down collagen and proteoglycans ("ground substance"), and some acquire
contractile elements as in smooth muscle ("myofibroblasts"). Of course, there are plenty of
macrophages (to keep the new tissue clean) and mast cells. The new tissue is called granulation
tissue ("immature scar", etc.), and the fibrin meshwork is said to be undergoing organization.
You've seen granulation tissue -- it was moist, red, jelly-like stuff under the scab that you picked off
too soon.
* You may run into granulation tissue that doesn't mature; depending on its location, you may call it
an "inflammatory pseudotumor", or whatever.
If everything goes well, eventually there is sufficient collagen to fill the gap (type I replaces
the type III originally laid down in the granulation tissue), most of the capillaries
are reabsorbed, the fibroblasts revert to a resting mode, and finally the myofibroblasts contract.
Especially where there has only been chronic inflammation,
you can also see dense collagen production, which of course also
counts as scar tissue. This is done by fibroblasts
on the instructions of macrophages.
{12707} granulation tissue
HEALING BY PRIMARY INTENTION
A well-approximated surgical wound is the ideal situation for wound healing. Since the edges are
close together and held tight by sutures and fibrin, and there is little necrosis and hopefully no
infection, the healing is by primary union or first intention.
Timetable for "the best possible wound" (i.e., a clean, protected one with edges apposed, in a well-nourished patient with
good blood vessels):
minutes: Fibrinogen from the severed vessels is activated via one or the other arms of the clotting cascade,
forms a meshwork, and stops the bleeding. The meshwork also contains platelets.
24 hours: Polys have entered the fibrin meshwork
Epithelial cells are regenerating from the edges of the wound surface, etc.
3 days:
The fibrin meshwork is extensively invaded by macrophages.
Granulation tissue is appearing at the edges of the incisions.
A thin layer of epithelial cells now covers the wound surface.
5 days:
Granulation tissue fills the entire wound, and there is abundant collagen.
2 weeks:
Fibroblasts continue to multiply, and collagen continues to accumulate.
4 weeks:
The overlying epidermis is now normal, though it will not re-grow adnexal structures.
Capillary involution and scar contraction is well underway, and the red scar is turning white.
The wound is still growing stronger, though it will never have the tensile strength of uninjured tissue
(sorry).
{08210} skin scar, nicely healed
HEALING BY SECONDARY INTENTION
Most wounds do not conform to the above ideal. There is a larger fibrin meshwork (a scab, rich in
red cells -- now brown because of methemoglobin), more inflammation, possibly infection, more
granulation tissue, and more spectacular wound contraction (up to 90-95% of the original surface
area.)
When epidermis grows underneath some of the fibrin meshwork, the edges of the scab loosen. When
re-epithelialization is complete, the scab falls off.
As surface epithelium grows into crevices (i.e., down suture tracks, etc.), it excites excessive
fibroblastic activity. This is why there's more scarring where the sutures were.
Scarring by secondary intention always produces some deformity.
The weave of collagen in the final scar (primary or secondary intention) is never the same as in the
surrounding connective tissue.
Sometimes the granulation tissue undergoes striking proliferation beyond the wound margins. This
is called exuberant granulations by physicians and "proud flesh" by the public. (You'll excise it.)
More intractable are keloids, (literally "crab claws")
disfiguring scars with excessive collagen production, seen primarily in
darkly-pigmented people.
Treating keloids usually involves re-excision and injection of the
surgical bed with glucocorticoid and/or administration of surface
radiation. Newer remedies that show promise are tamoxifen (changes the milieu
of fibroblast growth factors) and 5-fluorouracil.
{12805} "keloids", gross
Even worse than ugly surface scars are acquired deformities of the cardiac valves, and scars that
compress or plug the lumens of hollow organs.
If a scar is subjected to continual strain, the wound will stretch. Incisional hernias are the best
examples of this phenomenon.
Other mishaps may occur.
Pigment in a wound is likely to stay in the macrophages. Hemosiderin may persist for years in a
scar, especially if the person already has a high total-body iron burden.
Fragments of epidermis trapped in a healed wound may grow into spheres "with the skin-side inside"
-- the familiar "epidermal inclusion cysts" ("sebaceous cysts", etc.)
Attempts by severed sensory nerves to grow back into wounded tissue may produce painful
"traumatic neuromas".
NOTE: The wall of an abscess is, of course, granulation tissue. * You may hear the revolting word
"pyogenic membrane" applied to the wall of an abscess.
WHAT MAKES WOUND HEALING HAPPEN?
As for inflammation, growth factors for wound healing are continually being discovered. "Big
Robbins" lists the seven growth factors that seem to direct the production of granulation tissue.
You should recognize platelet-derived growth factor as a key to fibroblast activation and
fibrogenesis, and recognize the names of the others ("epidermal growth factor", "fibroblast growth
factor", "transforming growth factors α and β",
interleukin 1, and TNF/cachectin.)
Angiogenesis remains rather mysterious; a couple of factors are known (Science 268: 567, 1995).
Fibrin itself seems to attract inflammatory cells, fibroblasts, and angioblasts. Contact inhibition and
crowding seem to put the brakes on the process. Material in "Big Robbins" on cell-cell and cell-matrix interactions are still
experimental. Now is a good time to read
up on "integrins" in your biochemistry book; such medicines as
natalizumab (α4 integrin
antagonist that has been found to be useful in
Crohn's disease and multiple sclerosis) will probably come into
use soon.
FACTORS MODIFYING INFLAMMATION AND REPAIR
Despite conventional wisdom, age is not known to exert much effect on inflammation or wound
healing.
Adequate nutrition is needed for good wound healing. Protein is needed for collagen synthesis, and
vitamin C for hydroxylation of the proline and lysine in collagen. Several enzymes required for
wound healing are zinc-based. Some surgeons supplement some or all of these nutrients for their
post-operative patients.
Inadequate blood supply greatly interferes with both inflammation and healing.
Wound infection interferes with timely wound healing. Foreign bodies (dirt, sutures, others) in a
wound are a tremendous aid to bacteria in causing infections, as the bugs
can cling to the surfaces and thus escape phagocytosis.
We do not know exactly how glucocorticoids interfere with wound healing, but the effect is potent.
(For starters, they inhibit the migration of fibroblasts into fibrin meshworks.)
Future surgical clerks: Here are some names for surgical operations!
-tomy: The surgeon cut something.
-ectomy: The surgeon cut something out.
-ostomy: The surgeon cut something to make a mouth. If one organ is named, the mouth opened to the
outside of the patient. If two organs are named, the mouth connected two organs.
-plasty: The surgeon changed the shape of an organ.
-pexy: The surgeon moved the organ to the right place.
-rraphy: The surgeon sewed something up.
-desis: The surgeon made two things stick to one another.
RULES OF THUMB:
In infections by the common bacteria (staphylococci, streptococci, gram-negative rods or cocci), the
predominant cell in the inflammatory infiltrate is the neutrophil.
In viral infections and autoimmune diseases,
the predominant cell in the inflammatory infiltrate is the lymphocyte.
There might be some neutrophils early-on in the process.
Whooping cough produces a spectacular increase in circulating lymphocytes.
In the spirochetal diseases (syphilis and Lyme
disease), the predominant cell in the inflammatory infiltrate is the plasma cell
along with plasmacytoid lymphocytes.
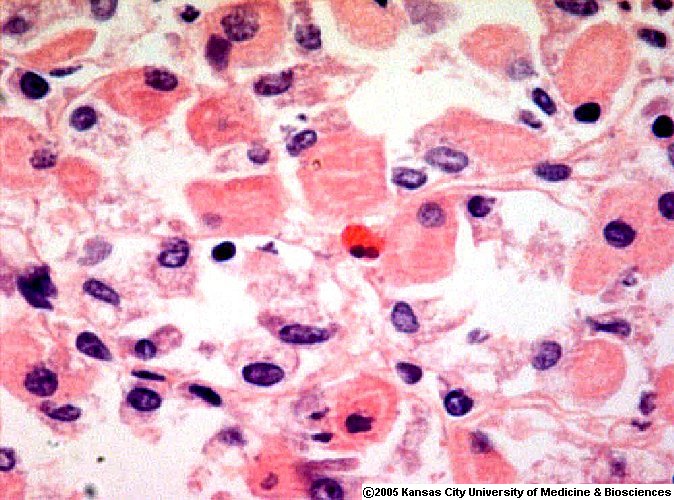
In typhoid fever, tuberculosis, and fungal infections (except candidiasis), the predominant cell in the
inflammatory infiltrate is the monocyte / macrophage / histiocyte / epithelioid cell.
* As above, in lymphogranuloma venereum, cat scratch fever, brucellosis, plague, tularemia,
glanders-melioidosis, and yersinia infection, there will be a plentiful mix of neutrophils and
epithelioid histiocytes.
In infections caused by metazoan parasites (i.e., worms),
and in Hodgkin's disease, and in most inflammations in the gut,
a predominant cell in the
inflammatory infiltrate is the eosinophil.
But depending on the agent and the host, there may not be any inflammatory reaction!
TYPES OF PAIN
If you have missed this so far in your medical education, learn it now.
In questioning people about their pain, you ask:
Aching pain: Probably periosteum, tooth, dura, or some circuit inside your own brain is involved
Burning pain: Either (1) the integrity of a mucosal surface has been breached, or (2) the nerve or its
immediate environment has been damaged (probably a depletion of substance P; "causalgia" from
nerve injury, thermal burns, sunburns, leprosy, epidermal necrolysis, capsaicin,
ergot; this is a "hot" topic
right now, and this responds to application of cold; see Lancet 345: 160, 1995.
Crampy pain (gas, labor, kidney stones): A hollow organ is being distended
Stabbing ("lancinating") (pleuritis, pericarditis, peritonitis): If you haven't really been stabbed, then
one of your serosal membranes is hurting.
Not really any of these: ischemia, common inflammation (everything from beesting to plague)
* If you want to get good at looking at pictures, and you have extra time, enjoy these pathology
pictures of inflamed tissue now:
{08121} polyp, inflammatory

* Of course, it was Virchow
who first demystified pus, showing that it was
white cells and necrosis.
{14704} normal neutrophil in a smear; finely
granular cytoplasm and segmented, dark nucleus
{10067} pus in an abscess, section; notice how neutrophils look different in sections and smears
{08979} histopathology of an acne pimple! Find two cross-sections of the keratin plug.
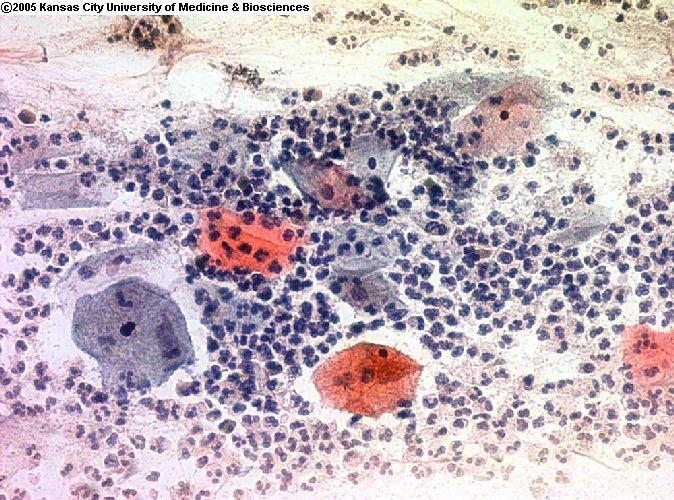 Neutrophils on
Neutrophils on
pap smear
Dave Barber MD, KCUMB
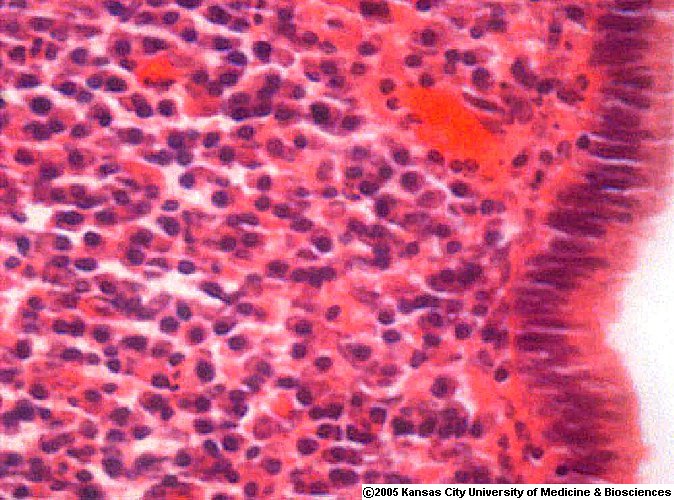
 Acute inflammation
Acute inflammation
Polys in gallbladder mucosa
WebPath Photo
{46310} acute inflammation from a bacterial infection of the kidney
{18719} fibrinous ("bread and butter", better "ketchup on bread") pericarditis
Their deficiency states are known. Obviously these patients mount a good increase in neutrophils
in response to infection, but the neutrophils don't enter the tissues very well.
Alcoholism, diabetes, and glucocorticoid therapy all reduce
the numbers of adhesion molecules. You'll be impressed with the difficulty
that such people have with fighting off bacteria.
(1) In viral and rickettsial
infections, the lymphocytes are the principal cell;
{13655} mature neutrophils (lots of segments;
can you see the granules?)
{16186} electron micrograph of neutrophil showing granules
{26189} immature neutrophil "bands" in the center
{13643} immature neutrophil "bands"; there is also
a lymphocyte
{09809} Pap smear, trichomonas vaginitis, showing neutrophils
{26442} monocyte in smear
C-reactive protein is a "marker for inflammation somewhere
in the body", but not much used except by researchers.
* An elevated level is supposed to be an independent
risk for coronary artery atherosclerosis (Circulation 100: 96, 1999).
The effect seems real and independent of other
factors. Your instructor believes that plaque grunge makes C-reactive
protein, and that this is the real explanation (rather than "atherosclerosis is
an inflammatory disease").
{10061} mostly lymphocytes;
{25397} autoimmune adrenalitis; low
power photo; many lymphocytes in the adrenal gland
{26430} small lymphocyte; notice that it is slightly
larger than the red cells
{26433} lymphocyte
{26436} lymphocytes, one resting, one a little bit turned-on (more cytoplasm,
more euchromatin)
{26412} plasma cell in a smear, top;
eccentrically-located clockface nucleus, abundant basophilic
cytoplasm, golgi pale spot
 Chronic inflammation
Chronic inflammation
Uterine cervix
ERF/KCUMB
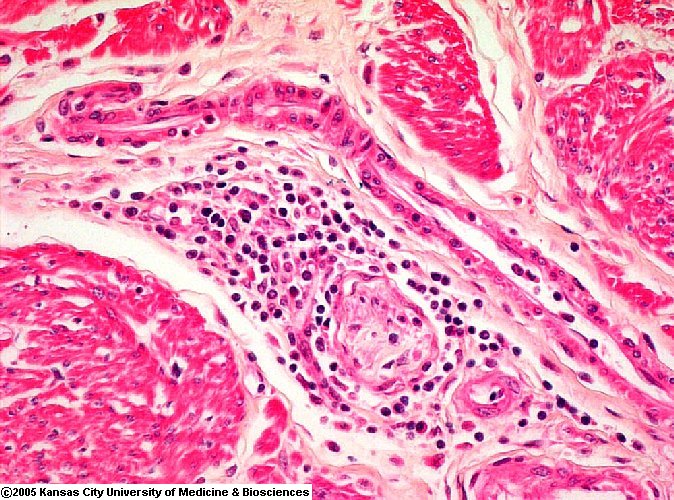 Chronic inflammatory cells
Chronic inflammatory cells
around a nerve twig
David Barber MD -- KCUMB
Mixed acute and chronic inflammation
Neutrophils and lymphocytes
WebPath Photo
 Eosinophils and lymphocytes
Eosinophils and lymphocytes
Two good eos in the center
ERF/KCUMB
 Eosinophil in stomach
Eosinophil in stomach
among parietal cells
ERF/KCUMB
Epithelioid cells of a granuloma
Purple rice krispies on a frayed pink tablecloth
WebPath Photo
Foreign body giant cell TB
Around a tiny vegetable fiber
WebPath Photo
 Granuloma Exhibit
Granuloma Exhibit
Yale Rosen MD
Nicest granulomas on the web
 Granuloma
Granuloma
Crohn's disease
ERF/KCUMB
{21428} granuloma with good asteroid body; this was a reaction to a jailhouse tattoo
 Tuberculosis
Tuberculosis
Granulomas and caseation -- trust me
WebPath Photo
Asteroid bodies
Lung pathology series; follow the arrows
Dr. Warnock's Collection
The newly-described entity "immune restoration syndrome" is seen in AIDS patients
who go on highly-active anti-retroviral therapy. Why might this produce granulomas?
{10964} tuberculosis, good caseous granuloma
{10106} sarcoid granuloma
{49350} silicone granuloma from ruptured breast implant
(microscopy would be needed for confirmation)
 TB granuloma
TB granuloma
Good caseous necrosis
WebPath Photo
If there is necrosis only of the epithelium, without any necrosis of the
underlying connective tissue, we call it an erosion.
Chronic Peptic Ulcer
Australian Pathology Museum
High-tech gross photos
 Inflamed Fibrin Meshwork
Inflamed Fibrin Meshwork
Ulcer crater
David Barber MD -- KCUMB
{10471} stomach ulcer (esophagus at right,
duodenum at left)
{53543} stomach ulcer (a section has already
been taken by the pathologist)
{10811} stomach ulcer, side view of a section through the crater;
see how the ulcer has penetrated through the muscularis propria and
only scar prevents perforation)
{11651} bad foot ulcer
{15560} bleeding stomach ulcer (arrow marks bleeding site)
{48177} diabetic ulcer
When you see a striking pseudomembrane, think of diphtheria (in the upper airway) or antibiotic-induced
pseudomembranous colitis (in the lower gut).
 Pseudomembranous colitis
Pseudomembranous colitis
Great photos
Pittsburgh Pathology Cases
 We rank cells according to their ability to regenerate:
We rank cells according to their ability to regenerate:
* The pop notion that normal chondrocytes never undergo cell division
is clearly false. Old folks' chondrocytes have much shorter telomeres
and other evidence of cell line senescence, and this probably has a lot to do with
"old-age arthritis" (J. Bone Joint Surg. 85-A (S2): 106, 2003).
* In animals models, neurons can reappear from
stem cell progenitors (even in response to SSRI's -- see
Science 301: 757, 2003).
REPAIR BY CONNECTIVE TISSUE
* They jest at scars that never felt a wound.
-- Shakespeare's Romeo
 Inflamed Fibrin Meshwork
Inflamed Fibrin Meshwork
Polys, red cells, dense and loose fibrin
David Barber MD -- KCUMB
{17606} granulation tissue in healing ulcer
{17607} granulation tissue in healing ulcer
{17608} granulation tissue
{17609} granulation tissue
{17610} granulation tissue in healing ulcer
{17611} granulation tissue in healing ulcer
When the scar contracts TOO well, as after a burn, messy surgery, or fibrosis-producing disease,
the result may be a crippling contarcture. You'll see plenty of these.
* Purists: Keloids send little processes into the surrounding
connective tissue, like the serrations on a crab's claw.
If these are absent, an exuberant scar is merely called
"hypertrophic". A keloid is likely to grow over time.
A hypertrophic scar is likely to regress over time.
Both can show glassy fibers.
{12807} "keloid", elbow
{24487} keloid, after a burn
{40368} "keloid", ear lobe
{25527} keloid, histology
{26432} keloid, histology
{26438} keloid, histology ("glassy fibers")
 Keloid
Keloid
Prize photograph
Institute of Medical Illustrators
Viral lung infection
Lymphocytes
WebPath Photo
* Almost everybody has experienced the "stitch", a brief,
sudden, stabbing pain that occurs with each of several
successive inspirations. This is probably due to a fold in the pleura.
(Relieve it with the deepest possible inspiration.)
{09322} polyp, inflammatory fibroid
{09806} inflammation, non-specific changes on a pap smear; look at nice neutrophils and the nuclei of the epithelial cells with somebig nucleoli
{09822} polyp, inflammatory polyp in stomach
{10058} inflammation, mixed acute and chronic
{10061} inflammation, chronic
{10106} inflammation, granulomatous
{10229} inflammation, granulomatous
{10529} inflammation, pseudomembranous colon
{10973} inflammation, chronic soft tissue
{12186} hypopigmentation, post-inflammatory
{12207} hyperpigmentation, post-inflammatory
{13153} inflammation, submandibular gland
{14350} dermatomyositis, severe inflammation
{14352} dermatomyositis, severe inflammation
{14432} polymyositis, acute inflammatory
{14433} polymyositis, acute inflammatory
{14702} polymorphonuclear leukocyte, normal
{14703} polymorphonuclear leukocyte, normal
{14704} polymorphonuclear leukocyte, normal
{14705} polymorphonuclear leukocyte, normal
{14706} polymorphonuclear leukocyte, normal
{14707} polymorphonuclear leukocyte, normal
{14734} polymorphonuclear leukocyte & lymphocyte
{14735} polymorphonuclear leukocyte & lymphocyte
{16061} chronic inflammation, liver
{16188} polymorphonuclear leukocyte
{16194} polymorphonuclear leukocyte
{16365} post inflammatory ossification
{16366} post inflammatory ossification
{16367} post inflammatory ossification
{16368} post inflammatory ossification
{16369} post inflammatory ossification
{16370} post inflammatory ossification
{16767} inflammation, glomerulus
{16771} neutrophil stuck to glomerular basement membrane
{17406} necrosis, fibrinoid inflammatory artery
{17612} inflammation, chronic acute skin (no normal tissue here)
{17613} inflammation, chronic
{17614} inflammation, chronic
{17615} inflammation, chronic
{17616} inflammation, chronic in skin
{17618} inflammation, chronic and acute
{17622} inflammation, lung
{17630} inflammation, chronic granulomatous lung
{20782} polymorphonuclear leukocyte, normal
{24601} carcinoma, inflammatory breast
{24652} inflammation, perivascular muscle
{24680} polyp, inflammatory colon
{25041} atypia, inflammatory
{25049} atypia, inflammatory
{25117} lymphogranuloma venereum
{25198} fibrous pseudotumor
{25776} single cell arrangement
{25869} inflammation, pap smear
{25897} inflammatory atypia - mild
{26001} lymphocyte
{26007} lymphocyte, chronic inflammation
{26107} inflammation, chronic
{26109} inflammation, acute and bacteria
{26187} promyelocyte and neutrophil segment
{26188} promyelocyte and neutrophil segment
{26189} neutrophil, band
{26190} neutrophil, band
{26191} neutrophil segment
{26192} neutrophil segment
{26193} neutrophil segment
{26194} neutrophil segment
{26201} neutrophil, band and metamyelocyte
{26202} neutrophil, band and metamyelocyte
{26211} myelocyte, neutrophil
{26212} myelocyte, neutrophil
{26214} neutrophil, band
{26215} neutrophil, band
{26230} polymorphonuclear leukocyte, normal
{29997} title slide
{30268} inflammation, brain
{30269} inflammation, brain
{32242} leishmaniasis in skin inflammation
{32287} brugia microfilaria with neutrophils
{34748} inflammation, vaginal smear
{38377} endarteritis, inflammatory
{39832} pelvic inflammatory disease
{39894} carcinoma, inflammatory
{40392} hydrocele; inflamed
{42013} carcinoma, inflammatory
{42015} carcinoma, inflammatory
{42017} carcinoma, inflammatory
{46186} polyarteritis
{46192} vasculitis
{46194} candida hyphae (silver)
{46195} candida hyphae (h&e)
{46199} toxoplasma
{46204} stenosis rheumatic mitral
{46213} pneumococcal septicemia
{46214} listeria
{46215} pyomyositis
{46218} tuberculoma
{46219} meningitis tuberculous
{46221} trichinosis
{46222} hepatitis herpes simplex
{46223} hepatitis herpes simplex
{46224} nocardia
{46225} coccidioidomycosis
{46226} histoplasma capsulatum
{46227} histoplasma capsulatum
{46228} histoplasma capsulatum
{46229} histoplasma duboisii
{46230} aspergillus fumigatus
{46233} candida albicans
{46234} cryptococcus
{46235} trichomonas mentagrophytes
{46236} aspergillus flavus
{46237} actinomyces israeli
{46238} nocardia
{46239} nocardia
{46240} microsporum audouini
{46241} leishmaniasis (cutaneous)
{46242} leishmaniasis (cutaneous)
{46243} leishmaniasis (kala azar)
{46247} malaria p. falciparum
{46248} malaria p. falciparum
{46249} malaria cerebral
{46251} stenosis rheumatic mitral
{46259} aspergillus septicemia
{46262} bronchiectasis and tuberculosis
{46263} asthma
{46268} Crohn's disease
{46289} herpes simplex
{46300} lupus band
{46301} dermatitis herpetiformis iga
{46305} rheumatic fever
{46310} pyelonephritis acute
{46311} pyelonephritis xanthrogranulomatous
{46317} Berger's disease (h&e)
{46318} Berger's disease (iga)
{46390} spondylitis ankylosing
{46391} rheumatoid arthritis synovium
{46392} rheumatoid arthritis
{46396} polyarteritis nodosa
{46441} Crohn's disease
{46443} amebiasis
{46466} carbon tetrachloride injury 24 hours
{46467} radiation injury
{46469} pneumonia cytomegalovirus
{46472} mast cell
{46473} mast cell degranulation
{46474} macrophage migration inhibition
{46475} Chagas' disease
{46476} Chagas' disease
{46477} Chagas' disease
{46478} cysticercus cellulosae
{46480} rheumatic valvulitis
{46481} rheumatic heart disease anitschkow myocyte
{46484} Crohn's disease
{46486} diarrhea (30 mins.)
{46491} treponema (Levaditi)
{46492} candida septicemia
{46493} echinococcus
{46495} trichuris
{46496} filaria
{46497} babesia
{46498} trichomonas vaginalis
{46505} tuberculosis
{46532} phlebitis pericentral
{46543}
hyaline droplets
{46548}
fibrin
{46551}
mast cell degranulating
{47613}
tooth pulp, inflamed
{47614}
tooth pulp, inflamed
{47621}
tooth pulp, inflamed
{47622}
tooth pulp, inflamed
{53544}
inflammation, necrotizing wall
{53545}
inflammation, necrotizing wall
{53546}
inflammation, chronic after inflammation
{05799}
eosinophilic granuloma multiple
{05800}
eosinophilic granuloma multiple
{05802}
eosinophilic granuloma, multiple
{05803}
eosinophilic granuloma, multiple
{05805}
eosinophilic granuloma, multiple
{05806}
eosinophilic granuloma, multiple
{05892}
very aggressive appearance
{05894}
granuloma, eosinophilic
{06190}
schistosomiasis egg shell in granuloma with giant cells
{07061}
trauma vascular obstruction
{07062}
trauma vascular obstruction
{07152}
trauma vascular obstruction
{09043}
eosinophilic granuloma, vulva
{09095}
eosinophilic granuloma
{09096}
eosinophilic granuloma
{09097}
eosinophilic granuloma
{09120}
granuloma
{09177}
eosinophilic granuloma, vulva
{09178}
eosinophilic granuloma, vulva
{09179}
eosinophilic granuloma, vulva
{09180}
eosinophilic granuloma, vulva
{09246}
thyroiditis, granulomatous
{09247}
thyroiditis, granulomatous
{09854}
Q fever hepatitis, ring granuloma
{10106}
inflammation, granulomatous
{10229}
inflammation, granulomatous
{10958}
granuloma, lymph node caseous
{10964}
granuloma, lymph node caseous
{10976}
granulomas, tonsil
{10979}
granulomas, tonsil
{10982}
granulomas, tonsil
{11423}
granuloma, lung fibrocalcific
{11541}
pyelonephritis, xanthogranulomatous
{11659}
granuloma, lung necrotizing
{11990}
Wegener's granulomatosis, necrotic nodule
{11991}
Wegener's granulomatosis, pulmonary
{12225}
granuloma, pyogenic
{12226}
granuloma annulare
{12356}
erosion, granuloma inguinale
{12783}
granuloma, pyogenic
{12784}
granuloma, pyogenic
{12786}
granuloma, pyogenic
{12787}
granuloma, pyogenic
{12789}
granuloma, pyogenic
{12790}
granuloma, pyogenic
{13053}
granuloma annulare
{13054}
granuloma annulare
{13056}
granuloma annulare
{13180}
granuloma, larynx
{13185}
granuloma, vocal cord
{13364}
histoplasmosis, lung; granuloma
{13365}
histoplasmosis, lung; granuloma
{13670}
granuloma, lymph node
{14427}
sarcoid, diffuse granulomatous myositis
{15376}
granuloma, lymph node
{15379}
granuloma with necrosis DF-2
{15671}
granuloma, eosinophilic
{15672}
granuloma, eosinophilic
{15746}
schistosoma eggs
{15757}
schistosoma
{17629}
inflammation, granulomatous lung
{17630}
inflammation, chronic granulomatous lung
{17631}
granuloma, lung
{19512}
colitis, granulomatous
{20125}
lipogranulomatosis, farber's
{20127}
lipogranulomatosis, farber's
{20206}
granulomas, spleen
{21285}
granuloma, peripheral giant cell
{21286}
granuloma, peripheral giant cell
{21294}
granuloma, peripheral giant cell
{21295}
granuloma, peripheral giant cell
{21296}
granuloma, peripheral giant cell
{21297}
granuloma, peripheral giant cell
{21298}
granuloma, peripheral giant cell
{21303}
granuloma, traumatic
{21367}
granuloma, central giant cell
{21497}
granuloma, central giant cell
{21531}
granuloma, peripheral giant cell
{21532}
granuloma, peripheral giant cell
{21533}
granuloma, peripheral giant cell
{21534}
granuloma, peripheral giant cell
{21535}
granuloma, peripheral giant cell
{21541}
granuloma, traumatic
{21542}
granuloma, traumatic
{21543}
granuloma, traumatic
{21545}
granuloma, traumatic
{21546}
granuloma, traumatic
{21584}
granuloma, pyogenic
{21585}
granuloma, pyogenic
{21586}
granuloma, pyogenic
{21587}
granuloma, pyogenic
{21602}
epulis, congenital=giant cell granuloma
{21603}
epulis, congenital=giant cell granuloma
{21604}
epulis, congenital=giant cell granuloma
{21605}
granuloma, peripheral giant cell
{21606}
granuloma, peripheral giant cell
{21607}
granuloma, peripheral giant cell
{21710}
granuloma, pyogenic
{21721}
granuloma, peripheral giant cell
{21777}
granuloma, peripheral giant cell
{21880}
pyogenic granuloma, conjunctiva
{21882}
pyogenic granuloma, conjunctiva
{21883}
pyogenic granuloma, conjunctiva
{23386}
lymphogranuloma venereum
{23422}
sarcoidosis, granulomas
{23425}
lymphogranuloma venereum
{23968}
prostatitis, granulomatous
{23999}
granuloma, post surgical
{24005}
granuloma, BCG
{24006}
granuloma, BCG
{24044}
pyelonephritis, xanthogranulomatous
{24045}
pyelonephritis, xanthogranulomatous
{24720}
thyroiditis, granulomatous
{24721}
thyroiditis, granulomatous
{24760}
granuloma, cholesterol tendon
{24852}
granulomatosis, Wegener's kidney
{24886}
xanthogranuloma, juvenile
{24918}
granuloma annulare
{25089}
granuloma inguinale
{25090}
granuloma inguinale, silver stain
{25117}
lymphogranuloma venereum
{25140}
epididymitis with sperm granulomas
{25141}
epididymitis with tubal rupture
{25142}
orchitis, granulomatous
{25143}
orchitis, granulomatous
{25196}
sperm granuloma
{25218}
prostatitis, granulomatous
{25220}
tuberculosis
{25340}
pyelonephritis, xanthogranulomatous
{27503}
berylliosis, granulomas
{27667}
coccidioides, granuloma
{27672}
coccidioides, granuloma
{29997}
title slide
{29998}
inflammatory granulomatous syndromes
{29999}
inflammatory granulomatous syndromes
{30000}
inflammatory granulomatous syndromes
{30001}
inflammatory granulomatous syndromes
{31978}
eosinophilic granuloma
{31996}
aspergillus granuloma, brain
{32215}
schistosoma mansoni egg granuloma
{32226}
pyogenic granuloma in skin
{32227}
schistosoma mansoni egg granuloma
{32251}
schistosoma egg granuloma
{32277}
schistosomal granuloma
{32311}
schistosoma japonicum granuloma fibrosis
{32321}
granuloma, noncaseating
{32324}
granuloma, noncaseating
{32346}
schistosoma japonicum granuloma, mouse
{34147}
granuloma, eosinophilic
{34150}
granuloma, eosinophilic
{34859}
eosinophilic granuloma
{35549}
beryllium, granuloma
{35552}
beryllium, granuloma
{36790}
granuloma, eosinophilic
{36793}
granuloma, eosinophilic
{37462}
granuloma, cryptococcus
{38881}
pyelonephritis, xanthogranulomatous
{39496}
granulomatosis, Wegener's
{39497}
granulomatosis, Wegener's
{39543}
granulomatosis, Wegener's
{39573}
pyelonephritis, xanthogranulomatous
{39574}
pyelonephritis, xanthogranulomatous
{39575}
pyelonephritis, xanthogranulomatous
{39879}
granuloma, fungal
{39880}
granuloma, fungal
{40073}
xanthogranuloma
{40120}
salpingitis, xanthogranulomatous
{40351}
granuloma
{40352}
granuloma
{40520}
granulomatosis, Wegener's
{40521}
granulomatosis, Wegener's
{40522}
granulomatosis, Wegener's
{40523}
granulomatosis, Wegener's
{40524}
granulomatosis, Wegener's
{40525}
granulomatosis, Wegener's
{40526}
granulomatosis, Wegener's
{40527}
granulomatosis, Wegener's
{40568}
granuloma, giant cell
{40569}
granuloma, giant cell
{40570}
granuloma, giant cell
{40571}
granuloma, giant cell
{40662}
granuloma, eosinophilic
{40663}
granuloma, eosinophilic
{40664}
granuloma, eosinophilic
{46311}
pyelonephritis xanthrogranulomatous
{49307}
pyelonephritis, xanthogranulomatous
{49350}
lipogranuloma from ruptured breast implant
{49459}
thyroiditis, granulomatous


| Visitors to www.pathguy.com reset Jan. 30, 2005: |
Ed says, "This world would be a sorry place if
people like me who call ourselves Christians
didn't try to act as good as
other
good people
."
Prayer Request
 Teaching Pathology
Teaching Pathology
PathMax -- Shawn E. Cowper MD's
pathology education links
Ed's Autopsy Page
Notes for Good Lecturers
Small Group Teaching
Socratic
Teaching
Preventing "F"'s
Classroom Control
"I Hate Histology!"
Ed's Physiology Challenge
Pathology Identification
Keys ("Kansas City Field Guide to Pathology")
Ed's Basic Science
Trivia Quiz -- have a chuckle!
Rudolf
Virchow on Pathology Education -- humor
Curriculum Position Paper -- humor
The Pathology Blues
 Ed's Pathology Review for USMLE I
Ed's Pathology Review for USMLE I
![]()
![]()
 | Pathological Chess |
 |
Taser Video 83.4 MB 7:26 min |

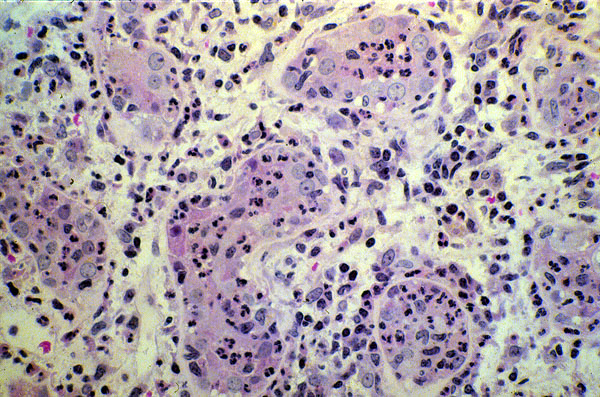 Acute pyelonephritis
Acute pyelonephritis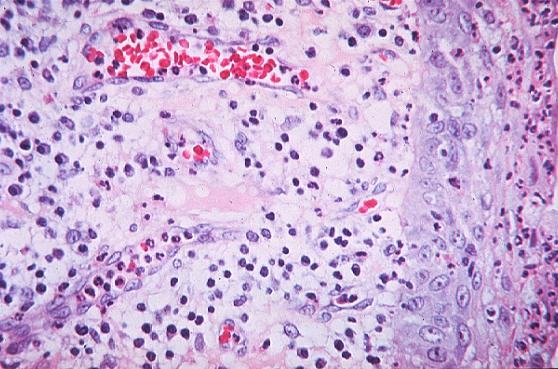 Inflammation
Inflammation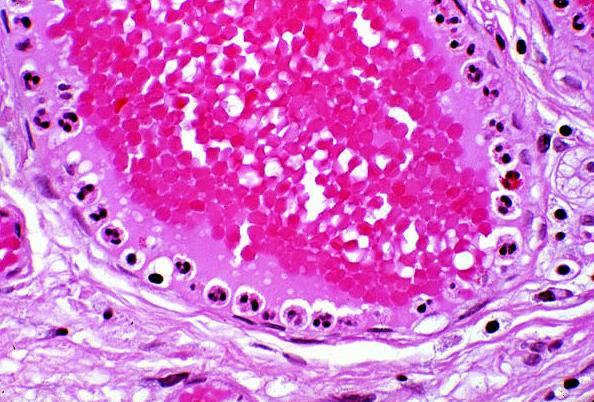 Polys marginating
Polys marginating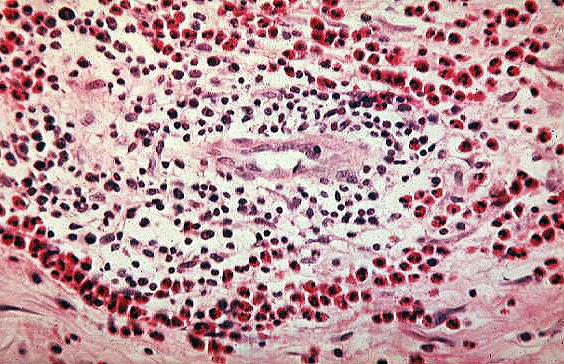 Eosinophils in tissue
Eosinophils in tissue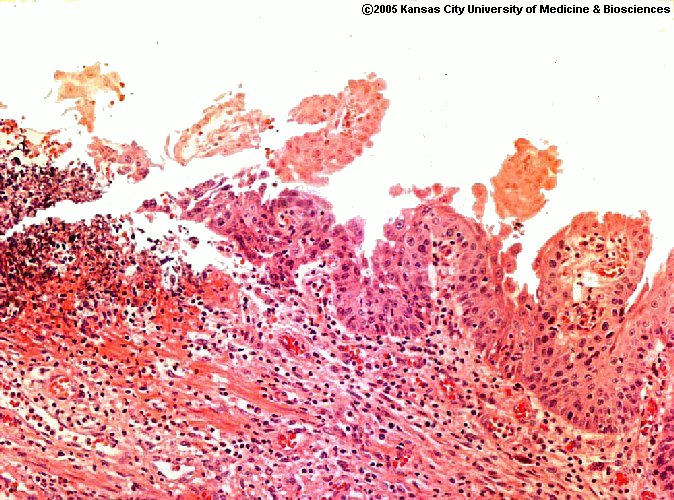 Esophageal erosion
Esophageal erosion Student Doc's Soccer Injury
Student Doc's Soccer Injury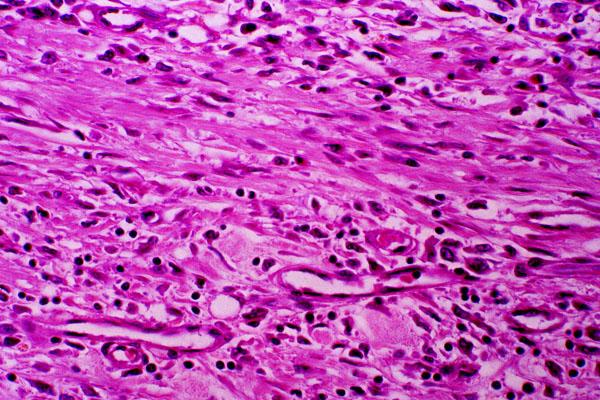 Granulation tissue
Granulation tissue