Ed Friedlander, M.D., Pathologist
scalpel_blade@yahoo.com



Cyberfriends: The help you're looking for is probably here.
Welcome to Ed's Pathology Notes, placed here originally for the convenience of medical students at my school. You need to check the accuracy of any information, from any source, against other credible sources. I cannot diagnose or treat over the web, I cannot comment on the health care you have already received, and these notes cannot substitute for your own doctor's care. I am good at helping people find resources and answers. If you need me, send me an E-mail at scalpel_blade@yahoo.com Your confidentiality is completely respected.
 DoctorGeorge.com is a larger, full-time service.
There is also a fee site at myphysicians.com,
and another at www.afraidtoask.com.
DoctorGeorge.com is a larger, full-time service.
There is also a fee site at myphysicians.com,
and another at www.afraidtoask.com.
Translate this page automatically
 |
With one of four large boxes of "Pathguy" replies. |
 I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
Numbers in {curly braces} are from the magnificent Slice of Life videodisk. No medical student should be without access to this wonderful resource. Someday you may be able to access these pictures directly from this page.
Also:
Medmark Pathology -- massive listing of pathology sites
Freely have you received, freely give. -- Matthew 10:8. My
site receives an enormous amount of traffic, and I'm
handling about 200 requests for information weekly, all
as a public service.
Pathology's modern founder,
Rudolf
Virchow M.D., left a legacy
of realism and social conscience for the discipline. I am
a mainstream Christian, a man of science, and a proponent of
common sense and common kindness. I am an outspoken enemy
of all the make-believe and bunk that interfere with
peoples' health, reasonable freedom, and happiness. I
talk and write straight, and without apology.
Throughout these notes, I am speaking only
for myself, and not for any employer, organization,
or associate.
Special thanks to my friend and colleague,
Charles Wheeler M.D.,
pathologist and former Kansas City mayor. Thanks also
to the real Patch
Adams M.D., who wrote me encouragement when we were both
beginning our unusual medical careers.
If you're a private individual who's
enjoyed this site, and want to say, "Thank you, Ed!", then
what I'd like best is a contribution to the Episcopalian home for
abandoned, neglected, and abused kids in Nevada:
My home page
Especially if you're looking for
information on a disease with a name
that you know, here are a couple of
great places for you to go right now
and use Medline, which will
allow you to find every relevant
current scientific publication.
You owe it to yourself to learn to
use this invaluable internet resource.
Not only will you find some information
immediately, but you'll have references
to journal articles that you can obtain
by interlibrary loan, plus the names of
the world's foremost experts and their
institutions.
Alternative (complementary) medicine has made real progress since my
generally-unfavorable 1983 review linked below. If you are
interested in complementary medicine, then I would urge you
to visit my new
Alternative Medicine page.
If you are looking for something on complementary
medicine, please go first to
the American
Association of Naturopathic Physicians.
And for your enjoyment... here are some of my old pathology
exams
for medical school undergraduates.
I cannot examine every claim that my correspondents
share with me. Sometimes the independent thinkers
prove to be correct, and paradigms shift as a result.
You also know that extraordinary claims require
extraordinary evidence. When a discovery proves to
square with the observable world, scientists make
reputations by confirming it, and corporations
are soon making profits from it. When a
decades-old claim by a "persecuted genius"
finds no acceptance from mainstream science,
it probably failed some basic experimental tests designed
to eliminate self-deception. If you ask me about
something like this, I will simply invite you to
do some tests yourself, perhaps as a high-school
science project. Who knows? Perhaps
it'll be you who makes the next great discovery!
Our world is full of people who have found peace, fulfillment, and friendship
by suspending their own reasoning and
simply accepting a single authority that seems wise and good.
I've learned that they leave the movements when, and only when, they
discover they have been maliciously deceived.
In the meantime, nothing that I can say or do will
convince such people that I am a decent human being. I no longer
answer my crank mail.
This site is my hobby, and I presently have no sponsor.
This page was last updated February 6, 2006.
During the ten years my site has been online, it's proved to be
one of the most popular of all internet sites for undergraduate
physician and allied-health education. It is so well-known
that I'm not worried about borrowers.
I never refuse requests from colleagues for permission to
adapt or duplicate it for their own courses... and many do.
So, fellow-teachers,
help yourselves. Don't sell it for a profit, don't use it for a bad purpose,
and at some time in your course, mention me as author and KCUMB as my institution. Drop me a note about
your successes. And special
thanks to everyone who's helped and encouraged me, and especially the
people at KCUMB
for making it possible, and my teaching assistants over the years.
Whatever you're looking for on the web, I hope you find it,
here or elsewhere. Health and friendship!
We have often seen in the breast a tumor exactly resembling the animal the crab. Just as the crab
has legs on both sides of his body, so in this disease the veins extending out from the unnatural
growth take the shape of a crab's legs. We have often cured this disease in its early stages, but after
it has reached a large size no one has cured it without operation. In all operations we attempt to
excise a pathological tumor in a circle in the region where it borders the healthy tissue.
LEARNING OBJECTIVES
Give short accounts of these non-neoplastic conditions:
Give accounts of these proliferative, benign, and "low-grade malignant" neoplastic
breast lesions, recognize obvious
examples microscopically, and tell the significance to the patient:
Recognize easy examples of ductal carcinoma in situ,
and distinguish the ones that are more likely to be aggressive.
Recognize non-infiltrating lobular carcinoma. Recognize Paget's
clinically and microscopically. Explain the significance of each.
Give an account of the risk factors, etiology, pathogenesis,
clinical findings, gross and microscopic pathology, metastatic patterns,
prognostic signs,
and lab workup (including markers) for each of the common types of
invasive breast cancer. Focus on the "why"'s when they are known.
Mention distinctive features of breast cancer in the male.
Read a breast biopsy with reasonable accuracy.
Accurately deal with patient questions about supposed health
hazards of breast implants.
Give a short account of how pop claims arise and how physicians should evaluate them.
QUIZBANK Breast (all)
REVIEW OF ORIGIN, ANATOMY, PHYSIOLOGY
{47710} {47732} {47725}
The anatomy and the physiology of the breast should be familiar to you.
* One does not have to be a breast-feeding militant to
take issue with Rubin & Farber's statement that "The breast has become
biologically superfluous in advanced societies."
The areolar tissue is pigmented, with smooth muscle and elastic
fibers. Montgomery's areolar
sebaceous glands (which prevent chapping) undergo hyperplasia during pregnancy; they
are the little bumps.
The breast is composed of a system of branching ducts draining
into
6-12 lactiferous ducts. The systems are extensively intertwined,
and I would urge you to ignore talk about "separate lobes".
Elastic fibers surround the lactiferous ducts and their branches.
The lactiferous duct widens to become the lactiferous sinus underneath the nipple.
Little groups of terminal ducts / acini are surrounded by a solid fibrous
stroma. The stroma between these units is fibrofatty.
As a woman gets older, there is usually more fat relative to stroma
in the breast. This
shows cancers (which are non-fatty) to advantage on mammography.
The duct system branches several times and ends in the collecting ducts.
Terminal ductules branch off the collecting duct. One collecting duct
and its terminal ductules, plus the accompanying stroma,
is called a "lobule".
You can recognize lobules in normal breast because
the stroma is looser and contains less fat and no elastin,
and the little ductules are clustered together.
During pregnancy, true secretory units sprout from each terminal duct,
coming to dominate the breast histology. After delivery, milk production
begins. You may see secretory units in a woman whose breasts
have become tender during the first few cycles on the oral contraceptive
pill, or "for no reason".
It's not clear to me that the male breast "is relatively
insensitive to hormonal
influences" (as Big Robbins tells us); men simply have little estrogen
and less progesterone on board. Hence the breast tissue does not
develop except under unusual circumstances.
Hormones to remember: During pregnancy, estrogen and progesterone prevent the milk from being
produced. When the pregnancy ends, lactation begins soon. Stimulation
of the nipple causes production of both prolactin (which keeps lactation going)
and oxytocin (which makes the milk come down).
At all levels of the duct-and-acinar system, there is a single
layer of myoepithelium. You can stain it for smooth-muscle-actin or S100 or high-MW keratin
or smooth-muscle myosin heavy-chain (probably best).
This contracts in response to oxytocin
to let the milk come down.
During the second half of the monthly cycle, progesterone causes some proliferation
of ducts and stroma in the lobules. When the cycle ends, these changes regress.
After menopause, the lobules may
vanish, leaving only the larger ducts.
Mother's hormones may produce some breast development in the
newborn baby girl, and there may even be a bit of secretion ("witch's milk").
You remember that some breast parenchyma extends toward the
axilla as the "tail of Spence". Generally, the upper outer quadrant of the breast is the most massive
anyway, which probably explains why most breast diseases are most common here.
{20793} normal breast
You should remember the duct cells, lobules, and myoepithelial cells.
You remember the anatomic "milk line" (check on most non-human female mammals).
Supernumerary nipples and supernumerary breasts (polythelia and polymastia) arise here, and are
very common. Accessory breasts may or may not have nipples, but undergo the same changes
during menstruation, pregnancy, lactation, and carcinogenesis as normal breast does.
DEVELOPMENTAL PROBLEMS
Inverted nipples are common, especially in larger breasts,
and may make nursing more difficult. If a previously-normal nipple
inverts, you have a problem, i.e., something has retracted underneath, and it's the stroma of a cancer
until proven otherwise.
Virginal hypertrophy: very large breast(s) developing around puberty. Really hyperplasia, of
course. The etiology is unknown, and occurrence is sporadic.
(Nowell's law at work, probably.)
{49360} giant fibroadenoma in a teen
Hypomastia: almost complete failure of breast development. (* Around half of these women have
mitral-valve prolapse. See NEJM 309: 1230, 1984.)
By contrast, very large breasts are likely to cause serious low-back problems.
{49359} hypoplasia of breast
INFLAMMATIONS: Not common.
Acute mastitis and breast abscess: Usually occurs during early lactation, less often in patients with
dermatitis. The bug is usually staph aureus (abscess-maker), less often streptococcus
(spreading cellulitis).
Fat necrosis: A solid mass, often in a fat breast, caused by a blow or other injury. Necrotic fat cells
surrounded by a mixed inflammatory infiltrate, later with calcification, foreign body reaction,
scarring. Before there was much notice paid to domestic
violence, the etiology was "mysterious".
Periductal mastitis ("recurrent subareolar abscess"): A hyperkeratinizing
squamous metaplasia going too far down a lactiferous duct. This gets inflamed
and needs to be cleaned up by a surgeon.
Almost all these people are smokers, and both men and women are affected.
Duct ectasia: An uncommon cause of a breast mass, usually in older women, usually tender and
with nipple retraction. Chronic inflammation and fibrosis around ducts are typical. The ducts are
loaded with a lipid-and-macrophage rich material. The cause is unknown
many of these women turn out to have pituitary prolactinomas.
*"Plasma cell mastitis", an old diagnosis,
is probably just duct ectasia with a lot of plasma cells. * Lymphocytic mastopathy is evidently an autoimmune disease.
It runs with Hashimoto's thyroiditis and type I diabetes. These lesions are patchy
but may produce masses.
* Granulomatous lobular mastitis is confined to the breast lobules.
All these women have been pregnant. Probably there is some autoimmune
reaction against the secretory units. Galactocele: One or more ducts became plugged during lactation.
Mondor's disease is thrombophlebitis of the breast, a minor mystery.
Rupture of an implant is commonplace, and in fact the fibrous capsules
that ordinarily form around implants helps contain this.
{49350} lipogranuloma from ruptured polyethylene breast implant
"FIBROCYSTIC CHANGE OF THE BREAST" (don't call it mammary dysplasia, chronic cystic
mastitis, etc.)
This is the commonest "disease" of breast (exactly how common is debatable).
It presents as a lump or lumps. Actually, it is always multifocal.
The cause, of course, is obscure. Unopposed estrogen is a known factor, and women on the
estrogen-progesterone balanced pills get less fibrocystic disease.
Despite much "pop" / "medical" wisdom, there's not much to suggest
that modifying a lady's diet will help her fibrocystic disease:
J. Am. Diet. Assoc. 100: 1368, 2000.
Three patterns occur separately or together:
1. fibrosis
2. cyst formation (>3 mm)
3. adenosis
Fibrosis: dense collagenization distorting and compressing the epithelial structures.
This is most common in upper outer quadrants, patients in 30's.
Your lecturer cannot agree with "Big Robbins's" claim that the fibrosis
results from ruptured cysts. If the cysts were filled with water, there
would be no reaction. If the cysts were filled with something else,
there would be a macrophage reaction, which you don't see in "breast fibrosis".
Cysts: dilated dusts containing cloudy serous fluid (sometimes bloody or infected)
All breasts during childbearing years contain microscopic cysts.
They are abnormal when they got
larger than 2 mm or so.
Grossly, the blue-dome cyst is very familiar. Epithelium may be flattened, cuboidal, columnar,
piled up, and/or show apocrine metaplasia. Surrounding stroma likely to be fibrous. Cysts likely
to be tender before menses and after drinking coffee.
Adenosis: {21062} fibrocystic changes, breast
PROLIFERATIVE BREAST DISEASE (review NEJM 353: 229, 2005)
2. Sclerosing adenosis
3. Small duct papillomas
Epithelial hyperplasia means more than the usual two layers of cells in
ducts and/or lobules. At
least one layer will be myoepithelial cells.
Cells are piled up and may even fill ducts and/or ductules.
Between the heaps of cells, you will see cracks and crevices, and at least
the bottom layer will be myoepithelium. Most often, there is a mixed population of cells.
If there is some anaplasia of architecture (i.e., swiss cheese)
or cells (ugly nuclei), but you can't quite diagnose ductal carcinoma in situ,
you may diagnose "atypical hyperplasia". The cells
do not fill the ducts or acini, as cells of an official "in-situ cancer" would.
Don't try to figure out exactly where
to draw the line between "atypical
hyperplasia" and "carcinoma-in-situ", because the line is obviously
just a cultural
construct with no biological meaning. "CIS" is only slightly
more likely to progress to invasive cancer and death than is "atypical
hyperplasia."
Here are some helpful indicators that you're looking
at "benign change" rather than "cancer":
Since "atypical epithelial hyperplasia" gives a woman
at least five times her baseline chance of getting breast cancer,
and since one woman in nine will get breast cancer in her lifetime,
you'll want to follow these women closely. Sclerosing adenosis: proliferation of small ductules and sometimes even acini in a fibrous stroma.
This
mimics cancer both clinically and microscopically. Usually it's
a tender lump in the upper outer
quadrant. Patients are usually around age 30-40.
Tipoffs that you are looking at sclerosing adenosis rather than cancer:
(1) There'll always be myoepithelium, for which you can stain
(smooth-muscle actin, S100, high MW keratin).
(2) The normal
lobular architecture is preserved, though lobules may be expanded.
This is a low-magnification diagnosis.
(3) Sclerosing adenosis can be hard, but it
never cuts "gritty" like many cancers. {25570} sclerosing adenosis
* One particularly treacherous
sclerosing adenosis variant is "microglandular adenosis",
round uniform glands everywhere, even in the fat, no myoepithelium,
but with no anaplasia
and no desmoplasia. Radial scar is a star-shaped fibrosing lesion that looks
like a typical crablike cancer on mammography but that proves utterly
benign on excisional biopsy and confers no increased
cancer risk. A larger version is called complex
sclerosing lesion. See Am. J. Surg. 180: 428, 2000.
Small duct papillomas seldom produce masses. These possess
fibrovascular cores, with epithelial hyperplasia-type lesions on the top.
Leave the diagnosis of actual malignancy in such lesions to us.
All of these have a multiplicative risk with familial history of breast
cancer, i.e., these benign lesions are probably are caused by mutations
of genes other than BRCA1, BRCA2, and p53.
FIBROADENOMA (pathology: Am. J. Clin. Path. 115: 736, 2001)
The most common benign breast tumor, occurs at any time during reproductive life, most often
under age 30.
It presents a small, sharply circumscribed, freely movable nodule within the breast substance.
A loose stroma surrounds ducts that are often crushed flat.
* Ignore the distinction between pericanalicular and intracanalicular fibroadenomas.
{08461} fibroadenoma, gross
Cystosarcoma phyllodes: a bad term for a "worrisome fibroadenoma" that exhibits metaplastic
and/or anaplastic stroma and supposedly rapid growth. A better term is phyllodes tumor.
If it metastasizes, it will be as a sarcoma. But most patients do not develop metastases.
Pathologists are now reporting these as "benign" or "malignant" (the latter can metastasize as the
corresponding sarcoma).
"Phyllodes" means "leaves", referring to the artichoke-like appearance of many
of these tumors.
It's interesting to speculate about how both epithelium and stroma overgrow in a fibroadenoma or a
phyllodes tumor. Since stromal mitoses are much more common adjacent to epithelium, the
epithelial cells are probably producing a factor that causes stromal overgrowth. In fully malignant
phyllodes tumor, the stroma becomes an autonomous sarcoma (Nowell's law again). See
Cancer 70: 2115, 1992; clinical review Cancer 77: 910, 1996.
LARGE DUCT PAPILLOMA This is a little (less than 1 cm) lesion in a major duct just below the nipple.
It produces bloody nipple discharge when bits twist and break off.
Occasionally it causes nipple retraction.
{20230} intraductal papilloma
One in 100 of these tumors is actually a papillary carcinoma. (This is a hard call. Do not expect your
pathologist to call these tumors benign or malignant on frozen section.)
Future radiologists: Visualize them using a galactogram, injecting dye into each of the
lactiferous sinuses (Am. J. Roent. 159: 487, 1992. )
INTRODUCING CARCINOMA OF THE BREAST ("breast cancer").
{00120} breast carcinoma, gross, skin dimpling
This is the commonest cancer in women (though no longer the #1 cancer killer), and still "the most
feared cancer" -- justifiably so!
There will be around 250,000 new cases of breast cancer this year
in the U.S., and 4,000 deaths. (Of these, 1500 new cases will be in men, and 400 of these men will die of it.)s
It is rare before age 25, and of course more common with increasing age.
Around 1 in 9 women will develop breast cancer during her life.
Breast cancer usually presents as a dominant, painless mass. Nowadays
it is often found on mammography long before symptoms appear. Remember
that 10% of breast cancers do not show up on mammography.
"Risk factors" (big review Lancet 346: 883, 1995):
Every ethnic group has a high incidence of breast cancer; American Indians have the least.
You'll go crazy trying to sort out all the studies, but the
key to protection is evidently the amount of time the woman has spent
lactating.
*A history of bilateral cancers and/or onset in a young women suggests a familial tendency.
Early-onset familial breast cancer is usually due
to germline mutations of BRCA1 or BRCA2, less often Cowden's
or Li-Fraumeni (p53).
Not surprisingly, BRCA1 tends to be lost in sporadic breast
cancers, though not by mutation (Nat. Genet. 21: 236, 1999); * "Big Robbins"
merely notes that BRCA1 mutations are uncommon in sporadic breast cancer.
*Breast-cancer gene screening was Mr. Rifkin the
anti-biotechnology lawyer's main target in 1996, attacking
companies who were devising these tests for profit:
Science 272: 1094, 1996. He was joined in this by Gloria Steinham
and Bella Abzug. Their major
argument became void when (in mid-1996, thanks Bill) it became
illegal for insurance companies to
consider genetic predisposition a "pre-existing condition" and denying coverage.
It seems to me that a woman should be able to make an informed decision about whether
she should consider the prophylactic surgery that could very likely save her life.
* Women are now coming in for prophylactic bilateral mastectomies
because they have the genes and/or a strong family history. This cuts the risk
by at least 90% -- but not entirely, since the breast is not a sharply-circumscribed
organ (NEJM 340: 77, 1999). These resected breasts are usually
normal on pathologic study: Arch. Path. Lab. Med. 124: 378, 2000.
A woman who chooses this option at age 30 adds 3-5 years
to her life expectancy (NEJM 336: 1465, 1997); what's more, patients seem to be
very happy about this (JAMA 284: 319, 2000).
* Ataxia-telangiectasia carriers may be at extra risk; this continues to be disputed
The "balanced" estrogen-progesterone pill for post-menopausal women
seems to increase the risk even more: JAMA 283: 534, 2000.
Estrogen replacement as a risk factor for breast cancer after menopause
remains controversial. Most past studies have indicated no link
(Cancer 95: 960, 2002
found a link for Hispanic women).
Especially see JAMA 268:
1900, 1992. The latter authors decided that probably women who get estrogen replacement go to
the doctor more and get early detection of their breast cancers (sound familiar?)
Even the recent article that caused the hoopla over estrogen replacement
(JAMA 288: 872, 2002) didn't show a believable link.
* Watch for raloxifene, a medicine that works as an estrogen
on bone, and an anti-estrogen on breast, as a handy drug for post-menopausal
women (JAMA 28: 2189, 1999).
*The conventional wisdom that estrogen replacement is absolutely
contra-indicated in women who have had breast cancer is now
being reconsidered: Geriatrics 57: 25, 2002.Am. J. Ob. Gyn. 187:
289, 2002.
* The "melatonin hypothesis", current popular, links low melatonin levels
to breast cancer; the evidence includes claims that nurses who work night shifts
have greater risk, and that blind women have only half the rate of breast cancer.
Normal breast epithelial cells are loaded with melatonin receptors (Am. J. Clin. Path. 118: 451, 2002).
I predicted in 2002 that "the melatonin hypothesis" was based on recall bias
and would soon be discredited, and now one major
study found no relationship (JNCI 96: 475, 2004).
NOT risk factors... * The pop claim that antiperspirants
cause breast cancer is simply a lie.
The oral contraceptive pill is not a risk factor (at least I'm satisfied; NEJM 346: 2025, 2002
supports much previous work).
There is still talk of high-fat, low-fiber diet being a risk factor; I saw the earlier studies and was
totally unimpressed. In a study in which the researchers controlled for other risk factors, all
correlation between diet and breast cancer vanished (JAMA 268: 2037, 1992);
another big negative study: JAMA 281: 914, 1999, more recently
Am. J. Med. 113(S9B): 63S, 2002.
* Pregnancy after treatment for breast cancer does not increase the risk
of a bad outcome (Lancet 350: 319, 1997).
* Residental magnetic fields (Am. J. Epidem. 155: 446, 2002).
*Some anti-abortion activists claim that having an abortion will increase the woman's later risk of
getting breast cancer. The Bush administration seems to have endorsed this claim
(Nat. Med. 10: 759, 2004),
but nevertheless it is probably not true.
Now is as good a time as any to bring up "statistical relationships" and the
problems they cause. For starters, there seems to be a massive reporting bias (i.e., women with
breast cancer confess to having had an abortion, healthy women deny it: Am. J. Epidem. 134: 1003,
1991). The Swedes keep records rather than relying on patient reports, and when these were
checked the effect disappeared (Br. Med. J. 299: 1430, 1989). A study from New York based only
on examination of reports of fetal deaths and breast cancer cases found a positive correlation; but
they did not take into account whether and when the women had term pregnancies. See also Int. J.
Cancer 48: 816, 1991. JAMA 275: 283, 1996 & 276: 31, 1996 indicated that there's small, if any,
increased risk from an elective abortion. NEJM 336: 81, 1997 found no overall risk.
Nor did Am. J. Pub. Health 89: 1244, 1999.
Neither did Br. J. Cancer 79: 1923, 1999.
Neither did Science 299: 1498, 2003.
Neither did Lancet 363: 1007, 2004 (I think this one should have closed the book).
Neither did the Scotch study (J. Epid. Comm. Health 59: 293, 2005).
A slight, probably bogus, protective effect from having had an abortion:
Int. J. Cancer 110: 443, 2004 (Boston).
No effect in African-Americans: Cancer Caus. Contr. 15: 104, 2004.
You had still better mention
this "controversy" in "informed consent" if you are going to do abortions, though
by now the claim (which enjoyed a vogue with tort lawyers) has run
afoul of "Daubert", the anti-junk-science law.
*In the early 1990's, Greenpeace launched a massive campaign, directed
at the public, claiming that
organic chlorine compounds in industrial pollution
are the great cause of breast cancer today.
Supposedly these are estrogens and also cause
increased oxidative damage to DNA; however women
with breast cancer don't have any more of oxidative damage to DNA, or of organochloride
compounds, than do controls
(Arch. Env. Contam. Tox. 41: 386, 2001; Env. Health Perspect. 109 (S1):
35, 2001).
Of course Greenpeace's rhetoric was typical of
junk-science-based disinformation campaigns
("Paradigm shift!" "Scientific-medical
establishment!").
The left breast is involved a few % more cases than the right. That's probably because the left
breast
is a few % bigger.
There are a host of tumor types that we'll cover now.
NONINVASIVE ("IN SITU") CARCINOMA
Ductal carcinoma in situ ("DCIS")
Of course, to confirm that the cancer is non-invasive, the savvy pathologist
can stain the myoepithelial cells.
Smooth-muscle myosin heavy chain is most popular today (SMMHC J. Clin. Path. 57: 625, 2004).
Please learn the Van Nuys grading-and-treatment scheme
for non-infiltrating ductal carcinoma: Lancet 345: 1154, 1995:
1: No necrosis (lumpectomy, skip the radiation)
2: Necrosis but no ugly nuclei (lumpectomy, maybe radiation)
3: Ugly nuclei (lumpectomy-radiation or mastectomy)
*Just to confuse you, here is the popular Scarff-Bloom-Richardson
for giving an architectural grade:
2: Can't decide
3: Comedocarcinoma
*And here's the latest synthesis:
Add 1 point if the tumor is 10 mm or more from the nearest margin,
add 2 if it is 1-9 mm, add 3 if it is <1 mm.
Add 1 if the tumor itself is <=15 mm across, add 2 if 16-40 mm,
add 3 if >41 mm.
Final scores of 3-4 have a 4% recurrence rate, 93% 8-year disease-free.
Final sores of 5-7 have 11% recurrence rate, 84% 8-year disease-free.
Final scores of 8-9 have 26% recurrence, 61% 8-year disease-free.
Low-grade ductal carcinoma, if left alone, turns invasive in maybe half
of patients, though often decades later. If an invasive cancer does
develop, usually it is at the site the the DCIS was (Cancer 103: 2481, 2005).
Comedocarcinoma (solid intraductal proliferation, central necrosis)
is the most common. Unlike the other "DCIS" lesions, the cells of
comedocarcinoma are usually quite anaplastic and vary widely in size.
It resembles blackheads on gross exam, and the necrotic cores
can be squeezed out. Often the necrotic cores calcify, making them easy to spot
on mammography.
Solid DCIS simply fills ducts. The cells are monomorphic
and monotonous; the nuclei may be big-ugly or small-tame.
Cribriform DCIS is swiss-cheese. Don't ask where "atypical intraductal
hyperplasia" ends and "cribriform DCIS" begins. Stupid lawsuits occur over this.
Papillary DCIS looks like the papillary lesions of proliferative
breast disease, with fibrovascular cores, but has a monomorphic cell population.
Micropapillary DCIS is little mounds of cells along the wall without fibrovascular cores.
If it turns invasive, it is highly aggressive (Am. J. Clin. Path. 121: 857, 2004;
Arch. Path. Lab. Med. 129: 1277, 2005).
"Paget's disease of the nipple": Intraepithelial growth of
large, pale, mostly-single cancer cells in the nipple. It looks inflamed. There is most often an
underlying duct carcinoma. Do not treat "eczema of the nipple" with cortisone without further
studies!
* Any DCIS extending in the ducts may produce "cancerization of lobules" (i.e., filling
the terminal ductules in a lobular unit). This probably doesn't mean anything
prognostically (Am. J. Clin. Path. 834: 1999).
{10931} Paget's disease of breast, gross
* Radiation added to simple excision cuts the rates of recurrence
(more DCIS and invasive cancer), but even without radiation, fewer than 20%
of women recur after excision (Lancet 355: 528, 2000).
While we're talking about radiation... if the margin of excision is 10 mm or more,
radiation clearly gave no benefit, 1-9 mm was a weak effect,
1 mm or less, radiation clearly helped prevent recurrence (NEJM 340: 1455, 1999).
* DCIS with microinvasion usually is comedocarcinoma with invasive
cancer confined to 1 mm away from the ducts. The prognosis is better
than if it were deeply invasive (Am. J. Surg. Path. 24: 422, 2000).
{12527} intraductal breast carcinoma, comedocarcinoma pattern
Non-infiltrating (in situ) lobular "carcinoma"
This is a distinctive proliferation of tame-looking cells,
slightly larger than normal, filling the ductules of one or more lobules.
The lobules are expanded but not distorted.
Often there are signet-ring cells.
It heralds (around 30% of the time)
infiltrating ductal or lobular carcinoma; however, the invasive
cancer is just as likely to be in the opposite breast.
"Lobular CIS" is usually
an incidental finding when tissue from the breast is excised and examined for some
other reason. As you'd guess, if you get a chance to examine both
breasts, it's usually bilateral.
{15525} lobular carcinoma in situ
INFILTRATING (INVASIVE) BREAST CARCINOMA
No Special Type (NST) ("usual type", "undifferentiated", etc.)
About 75% of infiltrating ductal carcinomas are of this type.
Most of these are stellate or micronodular, and quite hard, and these are called "scirrhous". Such
tumors present a chalky-white look flecked with yellow (elastin bands) on cut section.
Cutting the tumor produces the gritty
sensation of cutting an unripe pear. Don't be surprised by the presence
of elastin in these tumors; you know that healthy breast ducts are suspended by elastin
fibers.
Microscopically, "scirrhous" carcinomas with cells often arranged in nests or cords or
streams in a very
desmoplastic stroma. Although the books tell you that single-file "Indian file"
arrangement of cells is more typical of invasive lobular carcinoma, you can see
it often enough in a scirrhous cancer arising from ducts.
The cells usually do not look very malignant. Elastic fibers may be
prominent.
Medullary carcinoma
Big, bulky, and soft. Lymphocytes are plentiful among the tumor cells, perhaps
because the cells express HLA-DR strongly (nobody knows why). The prognosis is slightly
better than that of other types. (Do you think it's all those
lymphocytes fighting the cancer, or that this tumor is a distinct
disease? Maybe both.)
This type of cancer is much-overrepresented
among women with mutated BRCA1 syndrome (Lancet 349: 1505, 1997).
Mucinous (colloid, gelatinous) carcinoma
Clumps of cells in lakes of mucin. Grossly, the tumor is a gelatinous mass. Relatively favorable
prognosis.
* Adenoid cystic: Very low aggressiveness in the breast (Cancer 94:
219, 2002)
Papillary carcinoma
This is the one breast cancer that we think really
arises from the large ducts. Leave the distinction between benign
and malignant papillary lesions
to the pathologists.
{15488} carcinoma of breast, colloid type
Tubular carcinoma
Well-formed glands usually one cell-layer thick. Best prognosis for any breast carcinoma, very little
mortality. If there are no metastases to the regional lymph nodes, a cure is near-certain.
You can tell this from microglandular adenosis because there'll be
impressive desmoplasia and the glands will be angulated. Usually the tumor
is star-shaped grossly.
Metaplastic cancers (i.e., usually with cartilage): Nobody really
knows how this happens. Perhaps the cell of origin is myoepithelium.
Infiltrating lobular carcinoma (10% of infiltrating breast cancer.
Infiltrating lobular carcinoma is famous for its cells arranged
in Indian files. The cells tend to be very small and to lack
much anaplasia; they look like the cells of lobular carcinoma in situ
and often include signet-ring cells.
If you see them making circles around the ducts, the diagnosis is
a cinch, but an experienced pathologist can recognize these cells anywhere.
Such tumors are often multifocal within a breast, and are often bilateral.
Lobular carcinoma is infamous for spreading to the arachnoid and to bone.
{15484} carcinoma of breast, infiltrating lobular type
AFTER THE DIAGNOSIS OF BREAST CANCER IS MADE...
When examining these patients, look for:
** bad prognosis, of course
A majority of breast cancers arise in the outer quadrants, particularly the upper outer quadrant, and
the left breast is slightly more often affected than the right one (because it's
slightly larger naturally).
We used to teach that the single most important prognostic indicator in a case of breast cancer is the
size of the tumor at presentation. Now it's clear that the presence or absence of metastatic tumor in
the axillary lymph nodes is even more important (Cancer 70(6S): 1755, 1992).
Other favorable prognostic factors, in addition to those already cited, include:
The age-adjusted incidence of breast cancer among US women rose by 30%
during the 1980's. This is an artifact of finding them much, much earlier
(Soc. Sci. Med. 46: 907, 1998).
The newer studies mostly (not all) support breast cancer screening by mammogram
as a way of cutting mortality (though the impact is not huge): Lancet 353:
1903, 1999. The benefits drop to near-zero in the elderly (JAMA 282: 2156, 1999).
Fine-needle aspiration is becoming very popular, and panels of
molecular tests help with the prognostication (Am. J. Clin. Path. 113(5S1):
S49 & S84, 2001). These include DNA ploidy, proliferation rate,
HER-2/neu status
(FISH, immunohistochemistry; JAMA 291: 1972, 2004; Am. J. Clin. Path. 122: 110, 2004),
and p53 status.
Future clinicians: Here's a breakdown on these little lesions, which you'll localize by needle or wire
and excise (from Am. J. Surg. 164: 427, 1992, from Wash. U.; see also Br. J. Surg. 79: 1038, 1992)
80%...
benign
16 mm average size
NOTE: A great many genetic abnormalities have been found in breast cancer, but unlike many
cancers, there is no known invariable change. No claim relating prognosis to a particular genetic
lesion has stood up strikingly well, though checking for amplified c-erb-B2/HER-2/neu
is
now commonplace. Pathologists stain for the oncoprotein
(Am. J. Clin. Path. 113:251 & 669 & 675, 2000; assays
Arch. Path. Lab. Med. 126: 803, 2002); those with the amplification
may be treated with trastuzumab ("Herceptin"), a monoclonal antibody targeting
the protein.
Update Mayo Clin. Proc. 72:
54, 1997.
Here's a system that's becoming popular:
+1 if the cells are small, regular, and uniform
+1 if there are 0-9 mitotic figures per high power field
Scoring:
Unfavorable prognostic factors, in addition to those already cited, include:
One success story of the women's movement is the more rational, more thoughtful approach to the
therapy of breast cancer. Today's woman will be given an account of the risks of various
interventions, and be allowed to make her best choice. This is good. Rational management begins
with rational diagnosis.
Breast cancer is often, but not always, indolent; late recurrences (local,
metastatic) are
all too common.
{04607} metastatic breast carcinoma in brain, scan
You learn staging (which is not a "pathology" subject) and
therapies on rotations. They include:
NOTE: If a woman "wants to save her breast", and chooses radiation over surgery, she's risking
brachial plexus injury, with chronic severe pain and loss of the use of the arm. This was recently
brought to the public's attention by a women's pressure group, and rightly so. See Br. Med. J. 308:
188, 1994.
A variety of hormonal manipulations are available.
Tamoxifen, the anti-estrogen, is now standard for adjuvant therapy of
hormone-sensitive post-menopausal
breast cancer (Lancet 359: 2126, 2002). The use of tamoxifen
prophylaxis for women at high risk (i.e., lobular CIS, atypical hyperplasia,
strong family history)
is still under study, with both risks and benefits
rather small (Ann. Int. Med. 137: 59, 2002). The known hazards
include endometrial cancer, thromboemboli, exacerbation of endometriosis,
fatty liver, and
deceptive small blue "tamoxifen cells" on pap smear (Arch. Path. Lab. Med. 125:
1047, 2001).
The anti-progesterone agent RU486 / mifepristone has shown
good in-vitro activity
against many
breast cancer (J. Clin. End. Met. 75: 865, 1992; Mol. Endo. 13: 1657, 1999),
and shows some effect in patients with disseminated breast cancer
(J. Rep. Med. 43: 551, 1998),
but we await clinical studies (this is, after all, "the
controversial abortion pill"; common sense is finally winning
over politics and RU486 is finding occasional
use in advanced breast cancer: Fert. Ster. 68: 967, 1997).
Update on the politics: JNCI 92: 1970, 2000.
The late-1990's experiments with high-dose chemotherapy plus autologous
bone marrow transplantation for disseminated disease ("My HMO won't pay!")
ended up showing no advantage over conventional chemotherapy (NEJM 342: 1069, 2000).
Since protocols often depend on whether there are cancer cells in the lymph
nodes, pathologists now use keratin stains to show these up easily:
Am. J. Surg. Path. 23: 263, 1999; Lancet 354: 896, 1999.
{24707} post-mastectomy, post-radiation with lymphedema
Clinical course: The disease is likely to metastasize, but is often indolent, and late recurrences are
common.
The key to surviving breast cancer is early diagnosis.
* On rotations and afterwards, you'll learn a great deal more about
mammography and the follow-up of worrisome lesions.
To day, no one really knows what to do about very small lesions,
5 mm or less; some say they can safely be watched (Am. J. Surg. 190:
633, 2005).
DISEASES OF THE MALE BREAST
Gynecomastia
Proliferation of a man's ducts and stroma, unilateral or bilateral
It can be idiopathic (adolescents or older men), due to XXY, or due to hyperestrinism (tumors,
iatrogenic, female impersonators, guys using anabolic steroids to look more masculine, heh heh).
Other drugs to remember are digitalis and spironolactone; soy products contain
natural estrogens. Idiopathic gynecomastia puts a plain-vanilla
man at no greater
risk for cancer, but note that XXY's and female impersonators on estrogens
are at increased risk. The severity is widely variable. A man can be
cured by office surgery, if he wishes.
{49363} gynecomastia
Carcinoma of the male breast
Uncommon (100x less common than in women, 20x more common in XXY's than among other
men, and much more common in breast cancer families), but with only about 50% cure rate.
It is almost always an infiltrating ductal carcinoma, usually without much desmoplasia
{24603} carcinoma of breast, man
Other cancers
These can look totally benign clinically and microscopically, and
then metastasize. Many pathologists will tell you that all
hemangiomas of the breast should be considered malignant unless they are obviously
very sharply circumscribed, thoroughly benign-looking, and completely away from the lobules.
THE BREAST IMPLANT FIASCO: The U.S. public pays for willful ignorance of the fundamental
methods of science and rational decision-making, with women, as usual, the big losers (NEJM 326:
1696, 1992; NEJM 342: 781, 2000).
In April 1992, the FDA banned the use of silicone breast implants except in studies, even for women
with mastectomies (NEJM 326: 1713, 1992). In previous years, about 120,000 women per year got
breast implants for breast augmentation (i.e., "to look better"), and 30,000 got the implants for
reconstruction after mastectomy.
The "scientific rationale" was slim but not altogether lacking. We do know that silicone slowly
leaks out through the capsule of the implant. There was a series of four women with implants who
then got scleroderma (Ann. Int. Med. 111: 377, 1989). One other patient with a ruptured implant
got "scleroderma" and it resolved (!) when the implant was removed (Arch. Derm. 126: 1198, 1990).
Somebody was impressed enough to coin the term "human adjuvant disease", conjecturing that the gel was causing
people to get sensitized to their own proteins, and the rest is history.
Since the ban, a California study found anti-nuclear antibodies in 11 women with implants plus
scleroderma (most common), lupus, or some overlap syndrome; there was no typical serologic
picture, but the study related disease onset to traumatic rupture of the implants (Lancet 340: 1304,
1992). The most interesting work I've seen so far was 3 cases from South Carolina, in which silicon
was demonstrated at sites of connective tissue disease, and the illness remitted after removal of the
implants (Arch. Derm. 129: 63, 1993). A Danish mega-review found only 32 cases of all
connective tissue disease, mostly scleroderma (Kjoller et. al., 93134723, abstract), "much less than
you'd expect by chance" (gee whiz), but was impressed by anecdotes of disease clearing on removal of the
implants. A big review found no increase in connective tissue disease in implant recipients: NEJM
332: 1666, 1995; the only recent "study" that found a link took women's self-reports and made no
attempt to confirm them (i.e., if an implant recipient said she had lupus, then she had lupus).
Updates: NEJM 334: 1505 & 1513, 1996; Neurology 46: 308, 1996 ("neuromythology
of silicone breast implants"); Plast. Recon. Surg.
99: 1362, 1997; Br. Med. J. 316: 147, 1998 seems to have finished
the "connective tissue disease" claim off.
"Antipolymer antibody"'s existence remains
unsubstantiated by the general scientific community.
The link with fibromyalgia (which is a real disease / syndrome but one that a pathologist cannot
exhibit) remains a public concern and I think with some reason.
The FDA did a survey of recipients' health
and x-rayed to see if the silicone had leaked. When the obvious confounders
were controlled for, everything pretty much disappeared except for a link
between implant rupture and "fibromyalgia".
Nobody's reproduced this surprising finding yet,
previous studies were negative (J. Rheum. 27: 2237, 2000)
or extremely weak (the Wichita group suggested that psychological
factors contribute both to fibromyalgia and to getting implants),
and the folks in Denmark found that
whether or not the implants have ruptured seems to have no effect
on how Danish women say they feel (Plast. Rec. Surg. 111: 723, 2003).
Under a 1976 law, manufacturers had to prove their devices were "safe and effective". Of course,
that doesn't mean risk-free. The FDA merely had to decide that the benefits outweighed any
demonstrated risks. Unfortunately, because the benefits of breast augmentation are subjective, the
FDA acted as if there were no benefits (NEJM 326: 1695, 1992). Internal memos from
manufacturers of the implants painted a less-than-edifying portrait of corporate America.
"Consumer advocates" who have always tolerated alcohol and tobacco (including all those tobacco
advertisements directed at young girls) and who raised no fuss over tainted "health-food" tryptophan
presented anecdotes and scare-stories designed to terrify the two-million-plus women with implants.
Militant feminists were divided between "a woman's right to make decisions about her own body"
and the need to oppose the "sexist" pressures that makes some women feel they needed breast
augmentation in the first place. (It seems to your lecturer that a reasonable person can say
"no" to the
latter while still supporting the former.) The result was a media circus that led to the ban, as well
as around $4 billion dollars in liability payments; the whole thing may end up costing $40-$60
billion (Science 276: 1564, 1997). See also Cleveland Clinic J. Med. 59: 539, 1992; Plast. Rec.
Surg. 90: 1102, 1992; CMAJ 147: 772, 1127 & 1141, 1992; Arthr. Rheum. 39: 1615, 1996. It
was ironic, in mid-1994 in the wake of the (expected) studies showing no serious risk (NEJM
330: 1697, 1994 was best-known), to hear the same investigative
journalists turn wildly indignant against the
FDA's ban ("Government interference in our private lives!")
A psychologist explains how this sort of thing contributes to public
ill-health by making people somatize: Ann. Rheum. Dis. 60: 653, 2001.
We need a word to go with "iatrogenic disease" to describe people
who develop real (though subjective) symptoms because of pop claims
about things that are probably harmless
(other people's perfume, other people eating
peanuts on the airplane, etc.) The FDA decided in late 2003
not to allow the devices to be reintroduced. I've given up trying to make sense of this.
By the way: "Women who undergo breast augmentation with silicone implants have a lower risk of
breast cancer than the general population. This finding suggests that these women are drawn from a
population already at low risk and that the implants do not substantially increase the risk (NEJM
326: 1649, 1992)". Well, looking at the statistics again, there probably isn't any real effect one way
or the other (NEJM 332: 1535, 1995). For some reason that I cannot explain, nobody seems to have
looked at bust size as a natural risk factor for breast cancer.
*SLICE OF LIFE REVIEW
{11770} breast, normal
Ed says, "This world would be a sorry place if
people like me who call ourselves Christians
didn't try to act as good as
other
good people
."
Prayer Request
 I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
Pathology Education Instructional Resource -- U. of Alabama; includes a digital library
Houston Pathology -- loads of great pictures for student doctors
Pathopic -- Swiss site; great resource for the truly hard-core
Syracuse -- pathology cases
Walter Reed -- surgical cases
Alabama's Interactive Pathology Lab
"Companion to Big Robbins" -- very little here yet
Alberta
Pathology Images --hard-core!
Cornell
Image Collection -- great site
Bristol Biomedical
Image Archive
EMBBS Clinical
Photo Library
Chilean Image Bank -- General Pathology -- en Español
Chilean Image Bank -- Systemic Pathology -- en Español
Connecticut
Virtual Pathology Museum
Australian
Interactive Pathology Museum
Semmelweis U.,
Budapest -- enormous pathology photo collection
Iowa Skin
Pathology
Loyola
Dermatology
History of Medicine -- National Library of Medicine
KU
Pathology Home
Page -- friends of mine
The Medical Algorithms Project -- not so much pathology, but worth a visit
National Museum of Health & Medicine -- Armed Forces Institute of Pathology
Telmeds -- brilliant site by the medical students of Panama (Spanish language)
U of
Iowa Dermatology Images
U Wash
Cytogenetics Image Gallery
Urbana
Atlas of Pathology -- great site
Visible
Human Project at NLM
WebPath:
Internet Pathology
Laboratory -- great site My team:
My team:Ed Lulo's Pathology Gallery
Bryan Lee's Pathology Museum
Dino Laporte: Pathology Museum
Tom Demark: Pathology Museum
Dan Hammoudi's Site
Claude Roofian's Site
Pathology Handout -- Korean student-generated site; I am pleased to permit their use of my cartoons
Estimating the Time of Death -- computer program right on a webpage
Pathology Field Guide -- recognizing anatomic lesions, no pictures

St.
Jude's Ranch for Children
I've spent time there and they are good. Write "Thanks
Ed" on your check.
PO Box 60100
Boulder City, NV 89006--0100
More of my notes
My medical students
Clinical
Queries -- PubMed from the National Institutes of Health.
Take your questions here first.
HealthWorld
Yahoo! Medline lists other sites that may work well for you

We comply with the
HONcode standard for health trust worthy
information:
verify
here. 


![]()
-- Cornelius
Celsus, ancient Roman physician.
Review the normal anatomy and hormone effects.
Inverted nipples
Tell what we know, and don't know, about the causes of "fibrocystic change".
Describe the range of anatomic pathology, and distinguish it yourself from cancer
under the microscope.
"Virginal hypertrophy
Acute mastitis
Periductal mastitis
Duct ectasia
Galactocele
Fat necrosis
Gynecomastia
Benign hyperplasia
Atypical ductal hyperplasia
Atypical lobular hyperplasia
Sclerosing adenosis
Small duct papillomas
Fibroadenoma
Phyllodes tumor
Large duct papilloma
 Breast Exhibit
Breast Exhibit
Virtual Pathology Museum
University of Connecticut

Estrogen: Develops the big ducts
Progesterone: Develops the lobules and ductules ("acini")
Prolactin: Develops the secretory units and causes milk production
Oxytocin: Makes the myoepithelial cells contract and express milk
{11769} normal breast, histology
{11770} normal breast, histology
{10748} pregnant lady's breast
 Pregnant lady's breast
Pregnant lady's breast
WebPath Photo
{49361} supernumerary nipple
{12439} supernumerary nipple
* Probably the rarest breast disease with a name is
inflammatory gigantomastia, featuring enormous overgrowth of the breast
stroma and atrophy of the lobules, with lymhocytes around the ducts
and anti-nuclear antibodies (J. Clin. Endo. Metab. 90: 5287, 2005).
Obviously you'll want to rule out TB, sarcoidosis, and reaction to a ruptured
implant.
Benign Breast Lesions
www.breastdiseases.com
Physician guidelines area
This extremely common change means extra, crowded acini in some of the lobules. Often the lumens
are a bit distended ("blunt duct adenosis"), but they are not deformed, compressed
or distorted. Calcification is common.
{25567} fibrosis of breast
{25568} fibrosis of breast
{25569} cystic disease of breast
"Fibrocystic disease" probably doesn't put a woman at any extra risk
for anything. It's biopsied to rule out cancer.
Three entities have been removed from the "fibrocystic disease"
category
because they confer a significant cancer risk (i.e., mutations have begun
accumulating). They are:
1. Epithelial hyperplasia
Totally benign-looking hyperplasias
Atypical ductal hyperplasias
Atypical lobular hyperplasia
Epithelial hyperplasia is usually an incidental finding, and does not produce a mass.
{08942} fibroadenoma, histology
{08943} fibroadenoma, histology
{08944} fibroadenoma, histology
Fibroadenoma
WebPath Photo
Phyllodes tumor
WebPath Photo
Papilloma
WebPath Photo
 Breast Cancer
Breast Cancer
Australian Pathology Museum
High-tech gross photos
{00126} breast carcinoma, gross, recurrent at mastectomy site
{07561} breast carcinoma, gross
{10924} breast carcinoma, gross
{10928} breast carcinoma, gross
{12441} breast carcinoma, gross
{12533} breast carcinoma, infiltrating, gross
{49362} breast carcinoma
{49352} breast carcinoma
{24600} breast carcinoma
{10749} breast carcinoma
{00123} breast carcinoma, cytology
See also Lancet 360: 187, 2002. These analysis
conclude that the risk of breast cancer would be cut by 2/3 in the developed
world if women would just have as many babies and breastfeed for as long
as do the women in the poor nations.
Actually, "prevention of breast cancer", especially in patients at high
risk, is now fraught with medicolegal
issues (Postgrad. Med. 111:
83, Feb. 2002).
Much more dubious...
Cigaret smoking is not a risk factor for breast cancer, nor does it protect against it; a challenge to
this well-known observation bombed in 1996 (bad study JAMA 276: 1494, 1996,
trashed in Br.
Med. J. 313: 1226, 1996).
* In a review of Adventist diet studies (they eat little or no meat),
the folks at Harvard, not noted for political incorrectness,
pointed out that Adventist women have a disproportionately high rate of
breast and men of prostate cancer, and that vegetarianism seemed to be a risk
for breast cancer. Figure THAT one out. Am. J. Clin. Nutr. 78(S3):
539-S, 2003.
* Urban folklore has noticed
this and attributes the increase to more fondling by right-handed
partners.
If you're asked about this, it might be easiest to explain
that the left breast is normally bigger, and that there
is a much higher
incidence of breast cancer in nuns than
in past or present CSW's.
Ductal Carcinoma in Situ
www.breastdiseases.com
Physician guidelines area
Now that women go for mammography, we are finding a lot of these.
These lesions are non-invasive (yet), but can form masses by
filling ducts and/or lobules.
This is the most commonly-identified lesion on mammography.
These lesions are usually unilateral, they
often around for decades, and probably only a minority
ever invade.
Criteria for "ugly nuclei" are more than twice as wide
as a red cell, marked variation in size and shape,
coarse uneven chromatin, large nucleoli, more than two
nucleoli per nucleus, lots of mitotic figures.
1: Solid, cribriform, or micropapillary
Start with the Van Nuys number.
{24449} Paget's disease of breast
Paget's
WebPath Photo
Paget's
WebPath Photo
Paget's
PAS stain
WebPath Photo
Just what to do after an excisional biopsy reveals "ductal carcinoma in situ"
is still under study. On the one hand, it's more likely than not that the
woman will have no further problems following simple excision. On the other
hand, if cancer recurs and becomes invasive, it can kill her.
{12530} intraductal breast carcinoma, comedocarcinoma of breast pattern
{15498} intraductal breast carcinoma
Ductal carcinoma in situ
Photo and mini-review
Brown U.
Nowadays, women with breast cancer may be offered a contralateral prophylactic
mastectomy. This works to prevent breast cancer, and true to classic
teaching, invasive lobular carcinoma in the original breast is a strong
predictor of disease in the other (Cancer 101: 1977, 2004).
{15526} lobular carcinoma in situ
Infiltrating breast carcinoma
Photo and mini-review
Brown U.
Invasive Breast Carcinoma
www.breastdiseases.com
Physician guidelines area
Invasive ductal carcinoma:
The large majority of breast cancers are called "ductal",
even though we now know they really arise in the lobules.
Mucinous / colloid cancer
WebPath Photo
 Metaplastic breast cancer
Metaplastic breast cancer
Great photos
Pittsburgh Pathology Cases
{15485} carcinoma of breast, infiltrating lobular type
You will learn a great deal about the management of these patients
while you on rotations. The protocols will probably be different
by then.
Inflammatory carcinoma
Trust me
WebPath Photo
Inflammatory cancer
WebPath Photo
Inflammatory cancer
WebPath Photo
Today, the pathologist will examine the "sentinel lymph node", and probably
stain with cytokeratin to spot cancer cells not easy to see on H&E: Am. J.
Clin. Path. 117: 729, 2002. Rapid technique for immediate results during
surgery: Cancer 104: 14, 2005.
(
cyclin E, Ki67,
MIB-1 identify tumors that
are faster-growing and more likely to respond to chemotherapy;
"MIB-1 below 10% exclude from
chemotherapy"; methods
and cutoffs Cancer 94: 2151, 2002)
15%...
small invasive cancers
5%...
carcinoma in situ
+1 if 75+% of the tumor has cells making tubules
+2 if 10%-75% of the tumor has cells making tubules
+3 if less than 10% of the tumor has cells making tubules
+2 if the cells are big and/or vary some in size
+3 if the cells vary a lot in size
+2 if there are 10-19 mitotic figures per high power field
+3 if there are 20 or more mitotic figures per high power field3-5: Grade I
6-7: Grade II
8-9: Grade III
* Adjuvant chemotherapy following mastectomy for younger women in certain risk
categories seems to produce about 10% better survival at 10 years, but there are
quality-of-life issues as well: Lancet 352: 930, 1998.
* Most alarming, the guy who reported the big studies showing
an advantage refused to turn all of his materials over to an investigating
team, and the team concluded he had presented falsified data at two
international meetings (Lancet 355: 999, 2000).
{12442} reconstruction after mastectomy
* Comorbidity and compliance issues affect outcome. The British found
that their wealthier patients did better than their poorer patients despite
getting equal care (Br. Med. J. 320: 1442, 2000).
* Today, the greatest barrier to early diagnosis and treatment is
not poverty, but a level of ignorance that should not exist today.
Plenty of people believe that biopsying cancer makes it spread,
that the devil decides who gets cancer, and/or that chiropractors can
treat breast cancer effectively. These beliefs are most widespread
in a particular "culture" that has
a dramatically higher average stage at presentation
(JAMA 279: 1801, 1998.)
Adenoid cystic carcinoma
of the breast
Pittsburgh Illustrated Case
{12512} gynecomastia, histology
{49434} gynecomastia, 5 year old male, some kind of hormonal problem
Gynecomastia
WebPath Photo
The one entity worth mentioning here is the angiosarcoma,
cancer of the blood vessels. These occur in young women and/or after radiation, and
a majority are fatal (Cancer 104: 2682, 2005).
Silicone implant
WebPath Photo
Silicone implant
In place
WebPath Photo
Silicone leak
Granulomas
WebPath Photo
 * In Isaac Bashevis Singer's famous short story Gimpel the Fool,
one of the characters dies of cancer of the breast. The story deals with
a simple baker's struggle to be a good person in a world full of deceit.
Highly recommended.
* In Isaac Bashevis Singer's famous short story Gimpel the Fool,
one of the characters dies of cancer of the breast. The story deals with
a simple baker's struggle to be a good person in a world full of deceit.
Highly recommended.
{14992} mammary gland (prepubertal), normal
{14992} mammary gland (prepubertal), normal
{14993} mammary gland (prepubertal), normal
{14993} mammary gland (prepubertal), normal
{14994} mammary gland (secreting), normal
{14994} mammary gland (secreting), normal
{14995} mammary gland (secreting), normal
{14995} mammary gland (secreting), normal
{14996} mammary gland (ct stain), normal
{14996} mammary gland (ct stain), normal
{14997} mammary alveolus (active), normal
{14997} mammary alveolus (active), normal
{14998} mammary ducts (mature), normal
{14998} mammary ducts (mature), normal
{14999} mammary ducts (mature), normal
{14999} mammary ducts (mature), normal
{17489} breast, normal
{20293} breast, normal
{20690} mammary gland, normal
{20690} mammary gland, normal
{20691} mammary gland, gland epithelium
{20693} mammary gland, gland epithelium
{20694} mammary gland, gland epithelium
{20793} mammary gland
{20794} mammary gland
{20968} mammary gland
{20969} mammary gland, alveolus
{50571} breast, normal duct
{50572} breast, normal duct

Visitors to www.pathguy.com
reset Jan. 30, 2005: Teaching Pathology
Teaching Pathology
PathMax -- Shawn E. Cowper MD's
pathology education links
Ed's Autopsy Page
Notes for Good Lecturers
Small Group Teaching
Socratic
Teaching
Preventing "F"'s
Classroom Control
"I Hate Histology!"
Ed's Physiology Challenge
Pathology Identification
Keys ("Kansas City Field Guide to Pathology")
Ed's Basic Science
Trivia Quiz -- have a chuckle!
Rudolf
Virchow on Pathology Education -- humor
Curriculum Position Paper -- humor
The Pathology Blues
 Ed's Pathology Review for USMLE I
Ed's Pathology Review for USMLE I
![]()
![]()
Pathological Chess

Taser Video
83.4 MB
7:26 min

 Breast
Breast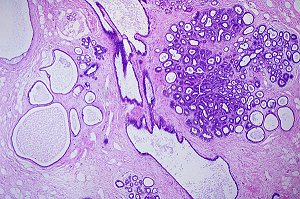 Fibrocystic disease of breast
Fibrocystic disease of breast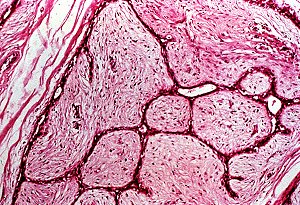 Fibroadenoma
Fibroadenoma Breast Cancer
Breast Cancer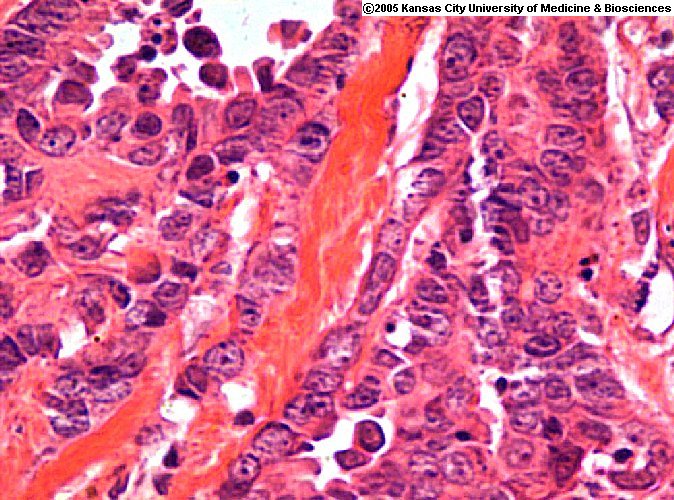 Indian Files
Indian Files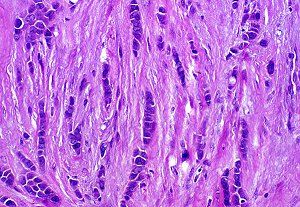 Breast cancer
Breast cancer