Ed Friedlander, M.D., Pathologist
scalpel_blade@yahoo.com



Cyberfriends: The help you're looking for is probably here.
Welcome to Ed's Pathology Notes, placed here originally for the convenience of medical students at my school. You need to check the accuracy of any information, from any source, against other credible sources. I cannot diagnose or treat over the web, I cannot comment on the health care you have already received, and these notes cannot substitute for your own doctor's care. I am good at helping people find resources and answers. If you need me, send me an E-mail at scalpel_blade@yahoo.com Your confidentiality is completely respected.
 DoctorGeorge.com is a larger, full-time service.
There is also a fee site at myphysicians.com,
and another at www.afraidtoask.com.
DoctorGeorge.com is a larger, full-time service.
There is also a fee site at myphysicians.com,
and another at www.afraidtoask.com.
Translate this page automatically
 |
With one of four large boxes of "Pathguy" replies. |
 I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
Numbers in {curly braces} are from the magnificent Slice of Life videodisk. No medical student should be without access to this wonderful resource. Someday you may be able to access these pictures directly from this page.
Also:
Medmark Pathology -- massive listing of pathology sites
Freely have you received, freely give. -- Matthew 10:8. My
site receives an enormous amount of traffic, and I'm
handling about 200 requests for information weekly, all
as a public service.
Pathology's modern founder,
Rudolf
Virchow M.D., left a legacy
of realism and social conscience for the discipline. I am
a mainstream Christian, a man of science, and a proponent of
common sense and common kindness. I am an outspoken enemy
of all the make-believe and bunk that interfere with
peoples' health, reasonable freedom, and happiness. I
talk and write straight, and without apology.
Throughout these notes, I am speaking only
for myself, and not for any employer, organization,
or associate.
Special thanks to my friend and colleague,
Charles Wheeler M.D.,
pathologist and former Kansas City mayor. Thanks also
to the real Patch
Adams M.D., who wrote me encouragement when we were both
beginning our unusual medical careers.
If you're a private individual who's
enjoyed this site, and want to say, "Thank you, Ed!", then
what I'd like best is a contribution to the Episcopalian home for
abandoned, neglected, and abused kids in Nevada:
My home page
Especially if you're looking for
information on a disease with a name
that you know, here are a couple of
great places for you to go right now
and use Medline, which will
allow you to find every relevant
current scientific publication.
You owe it to yourself to learn to
use this invaluable internet resource.
Not only will you find some information
immediately, but you'll have references
to journal articles that you can obtain
by interlibrary loan, plus the names of
the world's foremost experts and their
institutions.
Alternative (complementary) medicine has made real progress since my
generally-unfavorable 1983 review linked below. If you are
interested in complementary medicine, then I would urge you
to visit my new
Alternative Medicine page.
If you are looking for something on complementary
medicine, please go first to
the American
Association of Naturopathic Physicians.
And for your enjoyment... here are some of my old pathology
exams
for medical school undergraduates.
I cannot examine every claim that my correspondents
share with me. Sometimes the independent thinkers
prove to be correct, and paradigms shift as a result.
You also know that extraordinary claims require
extraordinary evidence. When a discovery proves to
square with the observable world, scientists make
reputations by confirming it, and corporations
are soon making profits from it. When a
decades-old claim by a "persecuted genius"
finds no acceptance from mainstream science,
it probably failed some basic experimental tests designed
to eliminate self-deception. If you ask me about
something like this, I will simply invite you to
do some tests yourself, perhaps as a high-school
science project. Who knows? Perhaps
it'll be you who makes the next great discovery!
Our world is full of people who have found peace, fulfillment, and friendship
by suspending their own reasoning and
simply accepting a single authority that seems wise and good.
I've learned that they leave the movements when, and only when, they
discover they have been maliciously deceived.
In the meantime, nothing that I can say or do will
convince such people that I am a decent human being. I no longer
answer my crank mail.
This site is my hobby, and I presently have no sponsor.
This page was last updated February 6, 2006.
During the ten years my site has been online, it's proved to be
one of the most popular of all internet sites for undergraduate
physician and allied-health education. It is so well-known
that I'm not worried about borrowers.
I never refuse requests from colleagues for permission to
adapt or duplicate it for their own courses... and many do.
So, fellow-teachers,
help yourselves. Don't sell it for a profit, don't use it for a bad purpose,
and at some time in your course, mention me as author and KCUMB as my institution. Drop me a note about
your successes. And special
thanks to everyone who's helped and encouraged me, and especially the
people at KCUMB
for making it possible, and my teaching assistants over the years.
Whatever you're looking for on the web, I hope you find it,
here or elsewhere. Health and friendship!
More of Ed's Notes:
 I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
Pathology Education Instructional Resource -- U. of Alabama; includes a digital library
Houston Pathology -- loads of great pictures for student doctors
Pathopic -- Swiss site; great resource for the truly hard-core
Syracuse -- pathology cases
Walter Reed -- surgical cases
Alabama's Interactive Pathology Lab
"Companion to Big Robbins" -- very little here yet
Alberta
Pathology Images --hard-core!
Cornell
Image Collection -- great site
Bristol Biomedical
Image Archive
EMBBS Clinical
Photo Library
Chilean Image Bank -- General Pathology -- en Español
Chilean Image Bank -- Systemic Pathology -- en Español
Connecticut
Virtual Pathology Museum
Australian
Interactive Pathology Museum
Semmelweis U.,
Budapest -- enormous pathology photo collection
Iowa Skin
Pathology
Loyola
Dermatology
History of Medicine -- National Library of Medicine
KU
Pathology Home
Page -- friends of mine
The Medical Algorithms Project -- not so much pathology, but worth a visit
National Museum of Health & Medicine -- Armed Forces Institute of Pathology
Telmeds -- brilliant site by the medical students of Panama (Spanish language)
U of
Iowa Dermatology Images
U Wash
Cytogenetics Image Gallery
Urbana
Atlas of Pathology -- great site
Visible
Human Project at NLM
WebPath:
Internet Pathology
Laboratory -- great site My team:
My team:Ed Lulo's Pathology Gallery
Bryan Lee's Pathology Museum
Dino Laporte: Pathology Museum
Tom Demark: Pathology Museum
Dan Hammoudi's Site
Claude Roofian's Site
Pathology Handout -- Korean student-generated site; I am pleased to permit their use of my cartoons
Estimating the Time of Death -- computer program right on a webpage
Pathology Field Guide -- recognizing anatomic lesions, no pictures

St.
Jude's Ranch for Children
I've spent time there and they are good. Write "Thanks
Ed" on your check.
PO Box 60100
Boulder City, NV 89006--0100
More of my notes
My medical students
Clinical
Queries -- PubMed from the National Institutes of Health.
Take your questions here first.
HealthWorld
Yahoo! Medline lists other sites that may work well for you

We comply with the
HONcode standard for health trust worthy
information:
verify
here. 


You should know this handout, which contains the essential content of the corresponding sections of a good pathology text, at the recall level. I am not kidding. My handouts are as clear as mud, and you owe it to yourself to use a real book for elucidation. The following structured objectives will help you as you master this material.
Explain the scope of pathology as a discipline. Recognize it as a physician's skill and activity as much as a body of knowledge. Explain how pathology integrates the study of disease at:
Recognize the major causes of failure in "Pathology" at the medical school level.
Briefly explain we say pathology is (or should be) a science.
Review how to distinguish science from cultural attitudes, junk science, aphorisms, pseudoscience, and politics. Give some examples from your own life-experience of ways in which politics adversely impacts on human health.
Briefly discuss the philosophic problems involved in defining "the cause of a particular disease".
 Define, correctly use, and recall (given the definition) the following ubiquitous pathology words:
Define, correctly use, and recall (given the definition) the following ubiquitous pathology words:
anatomic pathology
clinical pathology
diagnosis
diathesis
doctor
etiology
finding
forensic pathology
forme fruste
functional disease
general pathology
incidence
lesion
organic disease
pathogen
pathogenesis
pathognomonic
pathophysiology
prevalence
prognosis
risk
sign
symptom
syndrome
systemic pathology
Distinguish the different kinds of tissue samples that you will obtain for examination by pathologists.
Define hypoxia, and distinguish "ischemic", "hypoxic", "anemic" and "histotoxic" hypoxia, giving a full list of the causes of each. Describe the different effects of hypoxia on various tissues, and tell in considerable detail how we think hypoxia damages cells reversibly and irreversibly. Briefly cite other important things that damage cells.
Explain what free radicals are, sketch and name the important species, and explain in detail how and when they are generated, how they do damage, and how they are finally squelched. Mention the situations in which free radical injury is important clinically. Mention other chemical reactions that injure cells.
Define and correctly use "necrosis", and distinguish the various categories of necrosis (coagulation, liquefaction, enzymatic fat necrosis, caseous necrosis, apoptosis). Tell how you know a cell is dead. Explain why necrosis is not always visible when ischemia has caused sudden death. Explain how and when fat necrosis occurs, mention the settings for liquefaction necrosis, and list four infections characterized by caseous necrosis. Briefly describe the various forms of gangrene.
Describe the basic biology of lysosomes in health and disease. Mention other important ultrastructural features of cells that may be altered in disease. Give the sizes of cytoskeletal elements, including various types of intermediate filaments that distinguish different cells. Name the syndromes that result from their malfunction, and drugs that poison them.
Define, correctly use, and supply (given the definition) the following terms:
aplasia
atresia
autolysis
cell swelling
choristoma
cyst
cytolytic virus
cytopathic virus
diverticulum
ectopia
fatty change
fibrinoid necrosis
fistula
gangrene
hamartoma
heterolysis
heteroplasia
heterotopia
holo-
hypoplasia
inclusion body
karyolysis
karyorrhexis
local gigantism
occlusion
pseudodiverticulum
pus
putrefaction
pyknosis
sinus
spasm
stenosis
supernumerary
syn-
Give definitions and examples of each of the following, and recognize its presence in a description or photo as applicable:
Be sure you can recognize each of the following, grossly and/or microscopically, as applicable:
a turned-off cell
a turned-on cell
apoptosis
caseous necrosis
coagulation necrosis
contraction bands
enzymatic fat necrosis
fatty change
fibrinoid necrosis
karyolysis
karyorrhexis / nuclear dust
pus
pyknosis
viral inclusions
Have some sense of what various colors and consistencies will mean in gross specimens.
Ground rule: Here, and on all of my handouts, an asterisk (*) indicates a word, sentence, paragraph, or block of text is non-testable. Paragraphs positioned in outline form underneath a starred paragraph are, of course, not testable either, but {pictures} are. However, don't be surprised if you need some of this information for USMLE/COMLEX, roundsmanship, or even "real life". -- ERF
"Ed's notes" are sequenced after "Big Robbins" and are intended as lecture-helpers for my own students. Other students seem to like them, and they can be especially useful to users of the superb Slice of Life collection.
Nobody's lecture notes are substitutes for reading a good, solid textbook like "Big Robbins", "Rubin & Farber", "Chandrasoma", or others. And of course, nobody's lecture notes are a complete, authoritative guide to clinical practice, or (heaven forbid) your own physician's advice to you. Be wise, and use these notes appropriately.
Don't take life too serious. It ain't nohow permanent.
-- Walt Kelley, "Pogo"
Medicine, to produce health, must study disease, and music, to produce harmony, must study discord.
-- Plutarch
Oh, death has ten thousand several doors
For men to take their exits....
-- John Webster, The Duchess of Malfi (17th century)
Our lives are filled with joys and strife,
And what is death but part of life?
Will come the day that we must die,
And leave behind those learning why.
-- "The Pathology Blues" (Class of '98)
To fear death is nothing other than to think onesself wise when one is not. For it is to think one knows what one does not know. No man knows whether death may not even turn out to be the greatest of blessings for a human being; and yet people fear it as if they knew for certain that it is the greatest of evils.
It is the unknown we feaer when we look upon death and darkness, nothing more.
-- Socrates
-- Albus Dumbledore
We are accustomed to speak of "disease entities" as though they had an independent, individual existence and could be recognized as friends -- or better, perhaps, as enemies. This is obviously one of those abstractions that do violence to the reality of the concrete situation, for there is no disease apart from the patient. The disease is the change produced in the patient by a pathological process. Diagnosis involves the observation of the patient as he is, and also a reconstruction in imagination of the patient as he was, before he was afflicted. The disease is the difference between these two pictures. But this, also, is an abstraction.
-- Thomas Addis, M.D.
Don't get diseases in the first place, schmo.
-- Don Matthews
Director of Campaigns for People for the Ethical Treatment of Animals
responding to a question about animal research for treating disease; USA Today, July 27, 1994
If the patient has all of the risks laid out, as well as all of the benefits, very well-controlled studies have shown the patient tends to choose low-tech, low-cost treatments and is satisfied with the result, no matter what it is, because he chose it.
--C. Everett Koop, M.D.,
Chronicle of Higher Education,
July 1, 1992
Knowledge makes you vain, education makes you humble.
-- Hans G. Creutzfeldt, M.D.
Education is hanging around until you've caught on.
-- Robert Frost
A man who dares to waste one hour of time has not discovered the value of life.
-- Charles Darwin
American Osteopathic College of Pathologists, Inc.
12368 NW 13th Court Pembroke Pines Florida 33026
Phone 305-432-9640 Free student memberships available

QUIZBANK
General aspects of disease (all)
Degeneration and necrosis #'s 1-54, 66-68, 71
Disturbances of cell growth #'s 22-30
|
|
 LEARN FIRST
LEARN FIRST
Necrosis is the anatomic changes that result from abnormal cell death of cells within a living creature. The first light-microscopic proof that a cell is dead is shriveling and fragmentation of the nucleus.
Most necrosis results from loss of blood supply to part of the body. Hypoxia is the inability to carry out oxidative phosphorylation.
Coagulation necrosis retains the outlines of the cells. Liquefaction necrosis is usual following total loss of blood to the brain, or when neutrophils digest tissue as in most bacterial infections. Caseous necrosis is crumbling of tissue, and is most familiar in tuberculosis. Enzymatic fat necrosis results from the action of pancreatic lipase on belly fat. Apoptosis is enactment of a program for single-cell death, often on the instructions of a developmental program or T-killer cell, or in the setting of otherwise-sublethal cell injury, i.e., the body is removing unwanted cells.
Hypertrophy means cells growing bigger. Hyperplasia means cells growing more numerous. Atrophy means shrinkage of an organ. Metaplasia is transformation of one type of tissue into another normal type, because genes have been turned-on physiologically and/or mutated.
Anaplasia is bizarre cells. It means the genome has been destabilized. Dysplasia is anaplasia confined to an epithelium, i.e., precancer. These definitions and understandings will become critical when we discuss neoplasia -- formation of new, worthless organs.
INTRODUCTION
Bene ascolta chi la nota.
("He listens well who takes notes.")
-- Dante Inf. 15:99
My task, as your principal instructor in pathology, will be to teach you (1) the common ways the body fails, (2) the common ways the body responds to injury, (3) the common diseases, and (4) how to reason about disease.
Understanding is the key. To succeed in this course, you must try to understand (when applicable) instead of just memorizing. The worst advice someone can give you is: "There's no time in medical school to understand principles, you must simply memorize".
This is not impossible. Most of us probably know more rock-and-roll lyrics than there are words in "Big Robbins". We learned the lyrics easily because we knew the tunes. The key concepts in pathology will be the tunes that enable us to learn the "little details" that we need for patient care.
You can learn because, and only because, you are able to say as you go along, "This makes sense."
THINK. Your licensure exam is intended to test you ability to think, as well as your knowledge base. Master the key concepts early. Preview the material for each lecture beforehand. After you hear a lecture or read a paragraph in a book, try to rephrase it (whisper, write) in your own words. Review the material in the evening following the lecture, while it is still fresh; this will save you time. Talk with your friends, and explain what you're learning to each other. And look at pictures early.
This seems to take more time. But it will save you time, even in the short run, because it is much more efficient. It's like running your motor with your car in gear, rather than in neutral.
My promise to you is that, if you spend an hour in one of my lectures, you'll get more out of it than if you'd spent the hour with your book. You'll see pictures, hear anecdotes, watch me make sketches, and walk away with an overview onto which you can place your after-hours learning. What I will not do is read you my notes paragraph-by-paragraph. If this kind of "disorganized" lecture isn't to your taste, you're free to sit toward the back of the classroom and read to yourself instead, or read the newspaper, or whatever.
{19409} slice of life hooked up to a computer
In the past, students who have had difficulty with pathology have often had one or more of the following identifiable problems.
Cramming is the worst thing you can do, because the minute you get into it, you forget it.
-- Joe Montana
Further, you can't learn day-to-day unless you get enough sleep most nights.
There's a little bit written on pathology education, but not much (Hum. Path. 29: 750, 1998). If a medical school department responsible for the introductory pathology course "doesn't teach for the boards", perhaps the focus is on memorizing clinical protocols (Calgary: Acad. Med. 70: 186, 1993), or on current research, or the teaching is simply poor.
If public speaking is a problem for you, there's some great practical advice in Am. J. Nurs. 94(3): 64, Mar. 1994. advice on dealing with your fear in Nursing 21(8): 108, Aug. 1991, and bibliotherapy in J. Nerv. Ment. Dis. 178: 172, 1990, and Am. J. Psych. 151: 408, 1994. Fear of public speaking is extremely common and causes a lot of unhappiness: Arch. Gen. Psych. 53: 169, 1996. Even the surgeons, not noted for soft-heartedness, are screening their new students for public speaking phobia before they encounter disaster (Am. J. Surg. 176: 41, 1998). I'm no psychiatrist, but paxil, propranolol and monoamine-oxidase inhibitors are less likely to help you in the long run than simply confronting your fear. Come in prepared. If you need, I'll even coach you some, and unlikely as it seems now, I'm nicer than the types you'll meet when you present next year in "Morning Report".
In a study of year-one medical students (Acad. Med. 65: 586, 1990), the strongest quality-of-life predictor was strong social ties. You must work on keeping your social network in shape. If you are having difficulty, or don't know how, get good advice.
For one subgroup of students "at special risk", a no-nonsense trio of teachers found that the key is attitude: "injustice collecting / entitlement" fails, while "shut up, take-charge, work hard" succeeds ("locus of control" is what they call it; Acad. Med. 68(3), Webb letter). Surprised, America?
In any case, on the morning of the exam, if you are fairly certain you are going to fail (i.e., you haven't made it through the book or your notes), let the me know ahead of time. I'll worry less.
Can you love anyone without making him work hard? Can you do your best for anyone without educating him?
-- Confucius (Analects XIV.7)
Please feel free to interrupt lectures with questions. There are very few "stupid questions", only questioners who are foolish enough to remain lost. Don't take us too far afield during lecture, but otherwise, ask. However, please don't ask, "Is X associated with Y?" That's telling me you're cramming for a poorly-written multiple choice test, rather than trying to understand. Anyway, I use lots of synonyms on exams, so word-associations won't help much. You may ask, "What's the real relationship between X and Y?" That tells me you want to understand.
 This pathologist would define health (after Freud) as the full physical and mental capacity to
work, play, and love others, and disease (again after Freud) as internal problems that cause
pain and/or interfere with a person's ability to work, play, and/or love others. I consider
health to be a primary good, and will repeatedly say so. You may prefer a different definition, or
not want to bother with a definition.
This pathologist would define health (after Freud) as the full physical and mental capacity to
work, play, and love others, and disease (again after Freud) as internal problems that cause
pain and/or interfere with a person's ability to work, play, and/or love others. I consider
health to be a primary good, and will repeatedly say so. You may prefer a different definition, or
not want to bother with a definition.
Note that this definition applies to disease in animals also (and perhaps even in plants). Many, if not most, of the diseases we'll discuss also occur in animals, and probably predate the human race.
Don't call changes that are not really health problems "diseases". Because of people losing their insurance, we now sign out biopsies showing "fibrocystic disease" of the breast as "fibrocystic change" instead.
Not everything we'll describe in this course is a disease. The big heart of an aerobic athlete is something a pathologist can describe, but is desirable, and no kind of a health problem. In the 1970's, the American Psychiatric Association had the good sense to remove homosexuality from the list of "diseases". Some "diseases" (i.e., sickle cell trait, hemochromatosis gene) are mixed blessings, other "diseases" (Gilbert's, XYY, thal minima) are basically lab curiosities, milder versions of Thomsen's "myotonia congenita" merely gives you big muscles without working out, a man may either love or hate his big-brown-hairy androgen-hyperresponsive Becker's nevus, some cultures did or do go gah-gah over left-handedness or thal-minor, and every skin pathology book has a description of freckles.
 |
Top row: Achondroplasia (considered desirable in some cultures),
baldness-hirsutism (considered attractive or unattractive),
Becker's nevus, cross-dressing (stigma, unwanted compulsion, and/or
source of enjoyment), deafness (many deaf resent being called
handicapped, especially where sign language is widely spoken; this is
intensely politicized right now as some "multiculturalists" /
"advocates for the deaf"
try to prevent young children from obtaining cochlear implants),
Ehlers-Danlos (the unusual joint structure may confer superior musical
ability, as with Paganini), homosexuality (once a "disease",
now mainstream) Bottom row: Gilbert's disease (an abnormal lab finding with no health consequences), hemochromatosis (fatal if neglected, but offers advantages), left-handedness (carries a tremendous stigma in some cultures, where the left-handed go to great lengths to conceal their "disease"), myotonia congenita, serial killer ("They look just like everybody else" -- Wednesday Addams), dissatisfied straight who'd like to be "bi" -- some adults are now asking psychiatrists for help with this (J. Homo. 15: 7, 1988), XYY "stereotype of the karyotype". |
Blake's "visions" and "voices" strongly suggest schizophrenia, and sometimes they terrified and baffled him. His contemporaries considered that Blake's "genius" and his "madness" (both of which were obvious) must be part of the same process. But even today, I don't think any reasonable person would consider Blake "diseased" or "disabled". |
 |
A disease process is one of the generic mechanisms common to many diseases, i.e., inflammation, mutation, multiplication of infectious organisms, edema, thrombosis, and so forth. Alternatively, it can mean "pathogenesis". There is little reason to use the term "disease process".
Pathophysiology literally means "how physiology is altered by disease". If you know physiology, you can easily tell what is going to happen when you understand the pathogenesis of a disease. As a result, the term has a special meaning in medical education -- a course in disease that de-emphasizes pictures, taught by physicians who are not pathologists or surgeons. Usually it is run by internists.
Over 20 years as a medical school teacher has taught me that the common request, "Teach us more pathophysiology!" really means "Teach us physiology." I'm always honored, and we can always review normal "fiz" in lab.
At allied health schools, "pathophysiology" is the term for the course on disease, almost always directed by non-physicians.
In trivial-untreatable non-disease, the mainstay of therapy is education coupled with a sense of humor. A bodybuilder friend went from hating to loving his Becker's nevus upon receiving my advice: "Tell people that's where a bear licked you". A man with morphea is "Linoleum Man"; a man with treated hemochromatosis sports an "Iron Man" shirt; a man with multiple small lipomas "was conceived during a campfire-marshmallow-toast"; "My birthmark is an erogenous zone"; "Vitiligo? You have to pay extra for a two-tone chassis"; etc., etc.
Science and opinion. The first produces knowledge. The second produces ignorance.
-- Hippocrates, Laws of Healing
Public health, i.e., studying what influences, and how we might better influence, the health of our communities, is a proper part of a meaningful pathology course. I will be blunt. And you should be upset.
If I simply say, "Iodine deficiency causes goiter and lots of people are sick from this", it makes the world's poor folk sound foolish or indifferent. They aren't.
If I blame the goiter-belts' corrupt, moronic and tyrannical politicians, I am only telling the truth. There are not two sides to this business.
And the existence of widespread, crippling iodine, iron, and vitamin deficiencies in today's world offends me much more than the truth should offend you, Doctor.
Poverty, as used by social scientists, means a total income less than three times the cost of a varied, nutritious diet. Absolute poverty means total income less than the cost of a diet that will enable a person to work at maximum efficiency. Presently, one person in seven lives in absolute poverty.
"The developing world" is a euphemism for the poor nations. The causes of world hunger are complex, but it seems both cruel and patronizing to say "the developing world" when some (not all) of these countries are actually deteriorating. I prefer not to use the term, though again, this may "offend" someone.
One objective of this course is to help you understand popular and media claims about health and disease. Now's a good time to offer some more definitions. You'll want to know these for talking with your friends (and adversaries!) These are mine, but they work:
Science: Trying to learn about the world systematically, taking elaborate precautions against deception (especially self-deception). Advancing knowledge by testing hypotheses and developing theories, grounded in looking at the world as it really is.
Nature: The world of physics, chemistry, molecules, botany, zoology, astronomy, geology, human biology and pathobiology, the brain and its hard-wiring, the experiences and desires common to all human beings. Studied by the natural ("hard") sciences and general psychology.
Theory: An idea about the world that has consistently enabled people to make successful predictions. The round earth, the periodic table, the structure of the atom, the circulation of the blood, the earth orbiting the sun, plate tectonics, the genetic code, the expanding universe, Darwin's common descent of living things. Newton's and Maxwell's physics was true until Einstein's relativity and Planck's quantum theory added greater predictive power, and there have been further improvements.
Propagated error: Ill-grounded speculation or erroneous data that gets passed from author to author until it is ultimately corrected (and it will be). For several years after the first human karyotype, biology textbooks copied an original miscount and described 48 human chromosomes. Recently-corrected errors (each of which I called as such, years before their official correction) include the mechanism of action of selenium dandruff shampoo, herpes 8 cell proliferation being cancer ("Kaposi's sarcoma"), the rarity of primary progressive tuberculosis, and the 1960's and 1970's baloney about "sudden infant death syndrome". In my opinion, errors still in propagation include splinter hemorrhages as a sign of endocarditis, and the initial passage through the lungs of the deep cutaneous yeast infections. I will protect you from exam questions about these.
Pseudoscience: Using the language and authority of science, without using its methods. Astrology, Freudian psychoanalysis, Marxism, medical quackery, creation-science (in contrast to the religious-ethical doctrine of creation), hypnotic memory-enhancement, "dianetics", facilitated communication for autism (i.e., using autistic kids like ouija-boards), anti-immunization activism, anti-fluoridation activism, "contemporary gender theory", crackpot racial stuff, many others. Pseudoscience is about politics and big money. Dealing with pseudoscientists is distasteful and can be dangerous. Because their target audience wants to feel intellectually and morally superior and will not examine the subject fairly, pseudoscientists launch vicious personal attacks at anyone who tries to argue with them. Point out obvious untruths, and the discussion immediately turns into "Okay, we lied. You're still the bad guy. Now let's hear you explain this one...."
Junk science is one step above pseudoscience. It's a term, mostly used by lawyers, for poor natural-science (old studies, bad studies, discredited studies; also statistics and tables out of context as in pseudoscience) used in arguments directed at the public or in court. Real work is cited accurately, but very selectively and misleadingly. Much of this is obviously intentional by agitprop writers. Today's grown-ups are well-aware of this, and generally (and rightly) dismiss "new information about health risks" and "warnings of impending environmental catastrophes" as junk science.
Sub-science: My term for disciplines that try to study areas of major human concern but in which the methods of science (measurement, experiments) are difficult to apply. Emotion and ideology come to dominate the practitioners, and since the sub-sciences have an enormous influence on politics, this is bad.
Aphorisms are prominent in the sub-sciences and pseudosciences. These are statements that one wouldn't think are true, but that distill the passionately-held personal impressions that people decide are true BEFORE the usual methods of science have been applied. Aphorists usually claim that those who do not agree with them are wicked.
Even Virchow's dictum that "cancer cannot arise in an epithelium" (!!) remains a monument to the human capacity for self-deception. (Virchow did not consider those who disagreed with this aphorism to be wicked. But his mistake did lead to disaster.)
Of course I find that this psychological mechanism explains many other instances of intolerance too. You need to decide for yourself.
Why do smart people persist in believing stupid things? They seek out confirmation and support for their emotionally-held beliefs, and supplying these is an industry (Sci. Am. 287(3): 35, Sept. 2002).
Literary "theory" is a special case; the current ideology is "il n'y a rien hors la texte", which is obviously not true, and what's happening right now to college English departments is lamentable. Today's "postmodernism" fad, especially as represented in the works of Michel Foucault ("the era's greatest intellectual"), appears to me to rest upon confusing sub-science (and the harm it does) and real science (and the real knowledge it produces). I have never met or seen anything by a postmodernist or "social constructionist" who actually seemed to know any science.
Culture: Behaviors and attitudes that are not hard-wired into human beings, but are passed along from generation to generation to enable us to live together in relative peace, health, security, and satisfaction, instead of merely living the way that animals live. Studied by the other "soft" sciences and especially the sub-sciences.
The culture war: Probably as ancient as our species, the three-way struggle for control of human culture by the Left, the Right, and the naïve naturalists. The usual tactic is to present whoever doesn't want what you want as an unreasonable extremist of one of the other two categories.
Ideology: Any stupid-unreasonable-unscientific idea that some people believe passionately. In our world, the ideologies do enormous harm and little good. Followers of ideologies are ideologues. (You may prefer "suckers", "ditto-heads", "dupes", or any of the other synonyms.) Leaders of ideological movements get money and/or political power. Followers find companionship and feel intellectually and morally superior, and without having to be kind or decent to those around them. Typically ideologues mean well, and they leave the movement when, and only when, they find out they've been deceived intentionally. In my experience, every human being with a mental age of 12 or higher is interested either in science, or in one of the ideologies. I strongly recommend science, not ideology, to people with the responsibility of looking after other people's health and guiding public opinion. You can talk to me about it if you want.
Tolerating a diversity of opinions is fine. Giving respect to obvious lies is profoundly immoral. If you don't know this, you don't belong in medical school.
Politics: How people work with and against each other to distribute limited opportunities and resources. Especially in health care and education nowadays, every dollar that a special interest group demands is a dollar taken from somebody else. The fact that everybody prefers to ignore this basic truth explains many of the characteristics of public debate.
Right-wing (conservative) politics: Honest, thinking conservatives focus on how wealth and opportunities are created and defended, rather than how they are distributed. Distinguish good, decent conservatives from right-wing ideologues (traditional anti-science-religionists, majority-culture racists-sexists-hatemongers, the anti-contraception crowd, the folks responsible for apartheid, today's pseudo-Christian and pseudo-Islamic terrorists, etc.) Each of these ideologies is a public health problem.
Right-wing ideologues, being unreasonable and having their facts wrong, claim moral superiority and attack science and reason; almost without exception, they claim to be motivated by religious zeal. Right-wing ideologues portray honest, reasonable people as diabolic.
Good, decent conservatives look to science as the means to a higher standard of living, plus personal and national security. Think about it.
Left-wing (liberal) politics: Honest, thinking liberals focus on getting wealth and opportunities redistributed by the government, rather than creating or defending them. Distinguish good, decent liberals from left-wing ideologues (anti-science nature-mystics, minority-group racists-sexists-hatemongers, the "entitlement-rights-victims-political-correctness" crowd, the drug crowd, the animal-liberation folks, the magic-thinking brand of environmentalism, the folks responsible for communism, etc.) Each of these ideologies is a public health problem.
Good, decent liberals look to science as the means of ensuring a safe, clean environment, and the way to counter the ignorance and lies that form the underpinnings of prejudice and actual injustice. Think about it.
Left-wing ideologues, being unreasonable and having their facts wrong, claim moral superiority and attack science and reason; this is almost always in the name of the poor, the oppressed, the women, the minorities, and the alienated. Left-wing ideologues portray honest, reasonable people as wicked oppressors of the helpless downtrodden.
Today's postmodernists take early-1900's psychiatry at its least scientific (which really WAS institutionalized pseudo-knowledge that often wrongly stigmatized and oppressed people) as the prototype of medicine. It seems to me that these people are wrong to apply their analysis of stupid sub-science to genuine science and human reason.
Left-wing ideologues, who pretend to be "scientific", typically use the word theory when they mean "ideology". For the failure of "gender theory" to predict findings about sexual violence, see Violence & Victims 9: 95, 1994, Int. J. Law & Psych. 14: 47, 1991, the only two empirical studies on medline. The term "gender theory", once widely-used, has now vanished from the medical literature. The other favorite militant-Left term, "critique", is more of an admission that we're doing propaganda, not science.
Religion: Whatever people think deals with matters of ultimate concern. Various religions have varying contributions from science, ideology, secular philosophy, and revelation (whatever the latter is). Some definitions of religion would require some belief in the supernatural (i.e., causes outside the familiar subject-matter of science); other definitions would not.
Naïve naturalism (scientific reductionism): Two reasonable terms for the attitude (common but by no means the norm among scientists or those who admire science) that the extraordinary success of the natural sciences in adding to human knowledge and power means that human ideas about "the transcendent", "God", and so forth must be untrue.
Especially at high levels, scientists do tend to be much less likely to profess orthodox religion (i.e., to pray expecting results, and to believe in an afterlife): Sci. Am. 281(3): 88, Sept. 1999.
"The naturalistic fallacy", sometimes put forward by (and more often falsely attributed to) science-oriented people is this: "Because something happens this way in nature, therefore it should happen this way in human society."
Ethics: Trying to understand what we mean when we say "right" and "wrong", and why. Its real purpose in a pluralistic society like ours is to influence politics (i.e., trying to influence who gets what limited resources and opportunities, through selective moral indignation). Private work in ethics, i.e., the hospital ethics committee, usually focuses on finding precedents and common-sense for defending yourself when you're trying to do the right thing and/or the expedient thing and protect yourself in the process. By contrast, public discussions of "ethics" are often (not always) as one-sided and unreasonable as those from the most intolerant and dogmatic religionists. As you already know, ideologues always present themselves as highly moral, and their opponents (scientific thinkers, ideologues of other camps) as evil, venal, and immoral. Science acting alone cannot tell you what's right or wrong, but the best way I know to end up making a bad decision is to pretend that the world is something that it isn't, i.e., to ignore scientific knowledge. And it's been my experience that this is exactly where most (not all) public discussions of "ethics" are conducted -- in an atmosphere of make-believe and mud-slinging.
Great villains believe they're right.
-- Jean-Claude Van Damme, KC Star 12-23-95
Never underestimate the power of very stupid people in large groups.
-- Author unknown
When all think alike, then no one is thinking.
-- Author Unknown
The best lack all conviction, while the worst
Are full of passionate intensity.
-- Yeats
We thought, because we had power, we had wisdom.
-- Stephen Vincent Benet, "Litany for Dictatorships" (1935)
Mundus Vult Decipi.
The world wants to be deceived.
-- Latin Proverb (Martin Luther?)
It isn't what we don't know that gives us trouble, it's what we know that ain't so.
-- Will Rogers
Against stupidity, the gods themselves struggle in vain.
-- Schiller, "Maid of Orleans"
Believing is easier than thinking. Hence so many more believers than thinkers.
-- Bruce Calvert, mathematician
Opinions founded on prejudice are always sustained with the greatest violence.
-- Hebrew Proverb
A person about to speak the truth should keep one foot in the stirrup.
-- Mongolian Saying
Hoax: Deliberately falsified evidence, usually concerning something of grave importance, almost always targeting left-wingers or right-wingers. Important hoaxes in recent times include Carlos Castañeda's non-existent Yaqui sorcerers (he could not produce his field notes, acquaintances say he spent his time in the library reading books on shamanism, real Yaqui experts say they're obviously fake, and real Indians were outraged), the Paluxy River footprints "that proved humans lived at the same time with dinosaurs" (the creationists who carved the best ones confessed long ago, and this kind of fabrication is typical of classic "creation science"...), the Calavaras skull (a human skull supposedly found in very old strata; the "scientific source" for this often-cited "evidence for creation" is an old tabloid newspaper), the "Amityville Horror" fabrication (when the book wouldn't sell as horror-fiction, the author repackaged it as fact), Ferdinand Marcos's "gentle Tasaday tribe" (slum-dwellers transported to the jungle, talking their version of pig-Latin; the perpetrators targeted left-wingers who wanted to believe that a community could survive "in peace and harmony with nature" and without knowing how to fight, and the real anthropologists knew right away that it was a fraud because there was no "kitchen midden", i.e., no garbage dump), everything about Laetrile (right-wingers getting rich off other right-wingers), the popular books supposedly written by former members of powerful satanic cults ("Satan Seller" by Mike Warnke, "Michelle Remembers" by Michelle Smith, others; I'm pleased to note that these people were all exposed as fakes by their fellow-Evangelicals), Immanuel Velikovsky (didn't take college physics, and it shows), the Bermuda Triangle (Lawrence David Kusche took a year out of his life to examine the actual records of the supposed mysterious disappearances, and of course the accounts in the big-money books were massively falsified), and T. Lobsang Rampa's entire body of writings (when "the high Tibetan lama" turned out to be a Mr. Cyril Hoskins, the son of an English plumber, he claimed a "soul transplant" but could not read or speak a word of Tibetan). I would have liked to believe that Alex Haley had indeed miraculously traced his "roots" to Gambia, but the court proceedings brought out the sad truth about his elaborate, utterly cynical racial hoax. Sun films' documentary on the discovery of Noah's Ark (shown on TV in 1993) was the end-result of a skeptic's successful effort to demonstrate the lack of scientific standards at the most influential creationist organization; the "wood from the ark" was store-bought lumber steeped and boiled in teriyaki sauce, and a sniff would have been enough to reveal the hoax (let alone some honest tests on the wood). The famous "multiple-personality disorder" patient "Sibyl" was shown in 1998 to have been induced under hypnosis after a psychologist reviewed audiotapes between the therapist and the book author. The book helped cause the disastrous "repressed memories" fiasco of the 1980's to mid-1990's, which ended with tens of thousands of ruined families and huge successful legal judgments against therapists who had induced false memories. Fox TV's 2001 piece on the moon landings being faked was itself a masterpiece of bunko artistry (how it was done: Sci. Am. June 2001). "Historical revisionism" (holocaust-denial), crackpot biology (left-wing, right-wing), and most of the Kennedy assassination conspiracy theories are built on lesser hoaxes (along with fallacies and personality smears, of course). Scientists are much harder to fool, and in spite of what you've been told, most didn't make much of "Piltdown man" even decades ago. As physicians, you need to be able to recognize hoaxes, preferably before they are exposed. Your patients will ask you about them.
The impact of disease on humankind is tremendous. The subject is never "just academic". Each of us will have some first-hand experience with the content of a "pathology" course.
The citizens of today's western democracies are the healthiest humans who have ever lived. This is due almost entirely to the knowledge, technology, and improved standard of living produced by the much-maligned "dominant culture" characterized (at its best) by an emphasis on science, personal liberty, democratic government, free enterprise, and the work ethic. Contrary to what you may have been told (by "liberals", "greens", or "conservatives"; some of the latter still lie about the "healthy Hunza people of the far Himalayas"), we are far healthier than "indigenous peoples", past or present (pull up "indigenous people / tribes / tribal" on the medline if you don't believe me).
In the 1990's, we heard a tremendous amount about "cultural relativism" and "multiculturalism." Your lecturer (who gives his race as "human" and thinks everybody should do the same) appreciates multiculturalism, or what is left of it, so long as its proponents are understanders, peacemakers and enrichers (like in their rhetoric).
Multiculturalists begin by observing how human attitudes and behaviors differ from culture to culture. Ideological multiculturalism jumps to the conclusion that all of our beliefs and behaviors are culturally determined. This is contrary to common sense, common experience, and a large body of empirical evidence from field anthropologists about what all human cultures have in common. (The benign ones include trying to appease divine beings, having fashions in hair styles, having group sing-alongs, and seeking privacy for toilet functions.) And despite your lecturer's admiration for humankind in all our rich diversity((he hopes you will reject the a priori claim that "You should not judge another's cultural practice or belief about the world." (Nowadays, new moral imperatives are a dime a dozen, and they can't all be right.) You may find this articulated on college campuses, though not much in the hard sciences. I have noticed that since 9/11/01, the movement off-campus seems to have ended.
Today, the word "multicultural" in an article by and for physicians is usually is a euphemism for "multiracial" / "multiethnic", while the word "multiculturalism" has nearly vanished. Martin Luther King's dream was of a colorblind America, and today most people who are really trying to reduce racial prejudice try to de-emphasize categories and focus on what we all have in common (J. Pers. Soc. Psych. 78: 635, 2000).
As a physician, you'll do well to learn something about the idiosyncracies of ethnic groups, especially those that may impact on how you communicate with each other and whether they comply with your instructions. Presumably you're already a good enough listener and human being to respect what people tell you they want. Even the sociologists and anthropologists (the disciplines most famous for radical multiculturalism) now tell physicians, "Engaging with other cultures does not imply that all cultural norms should be accepted uncritically, as there may not always be room for compromise" (no kidding; Med. J. Aust. 176: 174, 2002). When Yale (not exactly a bastion of social conservatism) teaches multiculturalism to its medical students, they just hear about what communications styles and techniques might work best, and about possible attitudes toward disease that might help or hinder therapy (Acad. Med. 72: 428, 1997). Despite laments that most medical schools do not have "separate courses addressing cultural issues" (Acad. Med. 75: 451, 2000), I would not want to see a medical school teacher stand up and say "You need to know that ____ people believe ____, ____, ____, and ____, and they do ____, ____, ____, and ____, so as a doctor you must ____, _____, ____, and ____ with them."
Actually looking at the influence of "culture" on health and disease does not always show humankind at its best. ____ men object vehemently to their wives doing breast self-exam. If a man of the _____ culture fails economically, his family discards him. ____ intravenous drug-users generally refuse to use condoms. In the country of ____, the active partner in a homosexual relationship is perfectly acceptable, while the passive partner is a social outcast. In modern industrial nation of ____, there has never been an organ transplant surgery simply because people don't care about people they don't know. "In [the country of] ___, young people who suspect they may be infected with HIV will avoid a definite diagnosis while at the same time seek to spread the infection as widely as possible." And so on. See JAMA 285: 1075, 2001; Med. Anthro. 17: 363, 1997; many others. And if "all cultures are of equal value" or "you cannot judge another culture", how can we talk about our own civilization having made moral progress over the years, say by banning slavery or by giving women the vote?
One more note for health-care providers interested in the "multiculturalism" business: Don't fall into the trap of telling someone else, "You are of thus-and-such culture, therefore you are/want/believe thus-and-so." You will end up looking as foolish as the physician who was forced to disclaim, "All persons must be treated as individuals first, not as stereotyped members of a cultural group" (West. J. Med. 158: 201, 1993 for the not-at-all-funny story). I note with pleasure that even the ideologically-minded nurses are now repudiating ideological multiculturalism in favor of truth and common sense (Nurs. Inquiry 3: 3, 1996; J. Adv. Nurs. 23: 564, 1996; J. Prof. Nurs. 12: 159, 1996; the latter prefers "a transcultural ethics grounded in moderate realism"). Most recently, medical students overwhelmingly reject the sort of "cultural sensitivity training" that plays politics and/or pigeonholes people (article contains euphemisms: Acad. Med. 78: 1191, 2003).
The improvement of medicine will eventually prolong human life, but the improvement of social conditions can achieve this result more rapidly and more successfully.
-- Virchow
Following Rudolf Virchow's lead, your lecturer believes that good health is a fundamental value basic to all of humankind, and therefore hopes you will reject supposed "cultural values" that will predictably lead to impaired function / poor health (my list, closely modelled on Dr. Virchow's work):
These world-level political-social problems are the over-riding causes of both ill-health and general misery on our planet. No "culture" (or any other group) has a monopoly on good or evil; but the next time someone tells you that "All cultures are of equal value", compare the number of people trying to enter, and trying to escape from, the U.S., Canada, and Western Europe. Then be grateful.
To clarify: I know no secular meaning for the word "value" except as a statement of what real-life people want. "Multiculturalism" or no, "values clarification" or no, really get to know your neighbor "across cultural lines" and you'll almost always meet someone who wants the same things you do. These begin with good health, economic opportunity, personal self-determination, and respect. Etiquette and buzz-words differ among ethnic groups, and a good physician learns to avoid misunderstandings.
Your lecturer first placed these thoughts online in 1994. They are echoed especially in Ruth Macklin's "Against Relativism: Cultural Diversity and the Search for Ethical Universals in Medicine". Prof. Macklin comes up with pretty much the same ideas as your instructor: humaneness (i.e., being healthy rather than in pain) and humanity (i.e., having others allow you to choose your own path). See also Health Care Analysis 8: 321, 2000.
Pathology is often called "the science of disease", and this is a fair definition. By custom, nosology
means the actual semi-science of naming diseases (for example, in coding diagnoses for paperwork).
However, there are only a handful of underlying mechanisms of disease. The body responds to life's
hazards in stereotyped ways. These are the subject matter of general pathology (i.e., the stuff up
through "Neoplasia/Infections/Immunopathology"). You'll need to remember them well; they are
the template onto which you will place your knowledge of disease.
In contrast to general pathology, systemic pathology concerns itself with specific diseases that
involve the various organ systems. You can use your general pathology knowledge to predict the
contents of a chapter in systemic pathology. Anatomic pathology is the business of making
diagnoses by examining tissues, while clinical pathology is concerned with the rest of the things
done by the clinical lab, i.e., blood banking, clinical hematology, clinical chemistry, and clinical
microbiology. Forensic pathology is a subspecialty under anatomic
pathology, dealing with medicolegal issues.
A biopsy is tissue removed from a person during life and
that
will be sent to the pathologist for diagnosis. A rotten tooth or an ingrown
toenail will not be sent for diagnosis; most other tissues, including resections
where the diagnosis is already made, will be sent and hence are biopsies.
Open biopsy means an incision was made to obtain a larger mass
of tissue.
Excisional biopsy means the mass or entire organ was removed for
diagnosis and perhaps cure as well.
Autopsy ("necropsy") is the opposite of "biopsy". The pathologist examines
part or all of a dead body.
* Future pathologists (and future users of pathologist services):
These are the most common "problem" biopsies as judged by litigation! Am. J. Surg.
Path. 18: 821, 1994
If you've been brought up on "pop" ideas about health and disease, you'll be surprised by how little
you hear in this course about imbalances, buildup of poisons, poor circulation, or vital forces.
This
is the emphasis of folklore, not today's science. But you may find these folk-terms helpful in
explaining things to patients from various backgrounds.
Symptoms are, of course, the patient's subjective observations, while signs are evidence of disease
discovered by the physician. Unless otherwise qualified, "signs" are abnormalities on physical
exam, and findings are physical, lab or x-ray results. Lesions are fundamental pathologic changes
(usually anatomic derangements, though they may be molecular) that the pathologist can exhibit.
A syndrome is a cluster of related
symptoms and/or signs not necessarily due to the same causes in different
patients, but typically due to a single cause in any individual patient.
Your understanding of basic anatomy, biochemistry, and physiology can help
you understand the various syndromes.
A diathesis is a condition that interferes with normal response to minor hazards of daily
living. (The usual use of this odd word is "bleeding diathesis", i.e., the patients are fine until they
need to clot their blood.)
The etiology of a disease is its "cause", and "Big Robbins" begins with an important point: it is
simplistic to think of an individual disease having a single "cause". For example, you could
consider the "cause of fatal measles in poor countries" to be the measles virus, the malnutrition
that makes the infection more severe, the poverty and crowding in which the infection flourishes,
or the local laws that forbid immunization.
Intrinsic etiology means the genetic component of any disease.
Although the human genome is now sequenced, it
is not always clear how a particular mutation leads to a particular disease.
Extrinsic etiology is everything else -- bugs, physical injury,
poisons, bad nutrition, lots more
* Actually, can you think of anything with a single cause? The Buddha, attending an autopsy,
reportedly philosophized, "He died because he was born." If you are interested in quackery, you
will hear the following fallacy: "Since some people carry staphylococci or pneumococci without
becoming sick, microorganisms do not really cause any disease, and immunizations and antibiotics
are useless." A lie -- how would you answer it?
The closest we come to "single etiologies" is the one-gene disorders
and the extreme virulent infections (rabies, ebola, influenza).
In court, I am likely to be asked, "To a reasonable medical certainty, did the patient's exposure to
substance A cause disease B?" The requirement is "more likely than not", and the best way to
demonstrate it is that people exposed to substance A have more than twice the risk than do
unexposed people of getting disease B. Of course, you've got to control for everything else,
including other variables, selection bias, and recall bias.
Good luck. Note in particular that, as of right now, breast implants have
not met this test for any known disease.
The pathogenesis of a disease is the sequence of events at the organ, cellular, ultrastructural, and
molecular levels, by which the disease develops. The story -- from etiology to symptoms and signs --
is always complicated.
By convention, a pathogen is a micro-organism that causes disease.
Morphology / morphologic changes / morphologic derangements is
whatever the pathologist can exhibit grossly or under the microscope.
Pathognomonic is a big word that means that a particular abnormality is found only in one
condition. ("Hearing the fetal heart tone is pathognomonic of pregnancy." "Finding a Reinke
crystalloid in a primary benign testicular tumor is pathognomonic of Leydig cell adenoma.")
By contrast, a forme fruste of a disease is a very mild variant, that may teach us about the more
serious malady.
Organic disease has a clear anatomic and/or chemical lesion, while functional disease has not (yet?)
yielded its deep secrets and is assumed to result from subtle nervous system abnormalities and/or
mild mechanical problems. Pathologists seldom talk about "the functional diseases", i.e., don't
expect us to talk about migraine or low back pain with the same zeal as we discuss sickle cell
anemia.
The incidence of a disease is the number of new cases per unit time (usually given as "new cases per
100,000 people per year"). The prevalence of a disease tells how many people are affected at any
one time (typically, "cases per 100,000 people"). Obviously, prevalence equals incidence times average duration.
The risk of a disease is how much your unusual situation
(typically some kind of exposure to an uncommon hazard) increases your chance of
getting the disease compared with everybody else. "Relative risk"
has nothing to do with whether something is common or rare,
mild or severe.
The diagnosis is the name given to the particular disease, once it is identified. The prognosis of a
disease is the expected outcome for a particular case. "Good prognosis" suggests that recovery is
likely; "poor prognosis" suggests permanent disability or death. The prognosis is likely to be
influenced by the diagnosis, the age and general health of the patient, and the available treatments.
This unit deals with ways in which cells are injured, how they look, and how they adapt to different
conditions. We will deal with the interesting accumulations and deposits seen in and among cells in
a later lecture. If you want to understand disease (and that's why we'll call you "doctor"), this unit is
absolutely essential.
WHAT HURTS CELLS?
Necrosis is the death of cells prior to the death of the organism, and its visible (grossly and/or
microscopically) evidence.
* The law of nature is "adapt or die",
but we can only offer qualified support to "Big Robbins"'s idea that "adaptation, reversible injury, and
cell death should be considered states along a continuum of progressive encroachment on the cell's
normal function and structure." Once accepted, this idea would place sports training on a
continuum with flesh wounds.
* In classical pathology, we pay little attention to such adaptive (or maladaptive) phenomena as "up-regulation of surface
receptors". Traditionally, we have left the study of
these things to physiologists and pharmacologists. Remember that such cell adaptations are invisible
by light microscopy.
Hypoxia, or loss of the ability to carry on sufficient aerobic oxidative respiration, is the most
common cause of cell injury and death. It is still the prototype.
The causes of hypoxia:
Ischemia ("ischemic hypoxia"; "stagnant hypoxia"): Loss of arterial blood flow (* literally, "holding
back the blood")
Local causes
Systemic causes
Hypoxemia: Too little available oxygen in the blood
Oxygen problems ("hypoxic hypoxia")
Hemoglobin problems ("anemic hypoxia")
Failure of the cytochromes ("histotoxic hypoxia")
Cyanide poisoning
Dinitrophenol poisoning
Other curious poisons
{07447} carbon monoxide suicide; notice cherry-red color;
the blackening of the lips is drying, and the epidermis has
slipped off the chin; both indicate a post-mortem interval of a few days.
* NOTE: The best definitions of "hypoxia" (literally, "low oxygen") are broad enough to include all
causes of inadequate oxidative phosphorylation, as above. Yeah, some textbooks limit "hypoxia" to
"too little oxygen in the tissues", and I won't count this wrong, as long as you say "tissues" and not
just "blood" (that's hypoxemia). Gee whiz.
Of course, increased metabolic demands (exercise, fever) will exacerbate any of these problems. It
is rare, however, for anything more than temporary organ failure to result.
Despite the great importance of hypoxic injury, it is not self-evident why cells should actually die
just because they cannot carry on aerobic respiration. See below.
Neurons undergo frank necrosis after being deprived of oxygen for 3-5 minutes at normal
temperature (and clinically, brain damage follows much shorter intervals).
Heart muscle cells can last maybe 30-60 minutes.
Liver cells and renal tubular cells can last for 1-2 hours without oxygen before they are irreversibly
damaged (and of course, they're easier to replace.)
A leg can last for many hours.
Poor nutrition affects cells as it does people. Different cells react differently to starvation conditions.
Lack of glucose, for example, produces the same brain damage as does hypoxia. Other cells simply
waste away and die.
Infectious agents injure cells in a variety of ways. We'll study these under "Infectious Disease".
Certain clostridia, for example, produce phospholipase enzymes that break down cell membranes
and enable the bacteria to flourish briefly in dead tissue. Viruses and some rickettsiae explode cells
when they multiply. Other kinds of harm are far more subtle.
Immune injury (i.e., antibody or T-cell mediated) is of five enumerated types, which you'll learn
soon. Curiously, "Big Robbins" does not list damage to the body's own "innocent bystanders", which
routinely occurs in serious inflammation, even when lymphocyte-mediated immunity is not
involved. Much more about this later.
Chemical agents (noxious stuff, or even "too much of a good thing" like water or salts) and physical
agents including fire, freezing, electricity, barotrauma, and ionizing radiation (JAMA 266: 698,
1991), are less subtle causes of cell injury.
{01909} radiation necrosis of the brain (Think:
this must be toxic/metabolic rather than traumatic or vascular,
since you can see that
it limits itself to one particular tissue type, the white matter)
Glutamate excitotoxicity is a newly-examined cause of the death of individual neurons, in the
"neurodegenerative diseases". Stay tuned; there's even a drug (riluzole) to slow it down (NEJM
330: 585, 1994).
For some reason, "Big Robbins" also lists genetic errors as causes of cell injury, rather than the
results of injury to nucleic acids. Frequently, though, a cell that cannot metabolize something will
accumulate preposterous amounts of the substance and eventually may die from it.
Obviously, cell systems for maintaining membranes, metabolism, enzyme synthesis, and gene
preservation are inter-linked, and whatever affects one will affect the other. And of course, different
cells (types, sick or healthy) will respond differently to adversity. Damage that is obvious
microscopically is well-advanced.
In hypoxic injury, the sequence of cell injury and death is still yielding up its secrets.
The first change, of course, is loss of ATP production by mitochondria. Cellular ATP content drops
rapidly and work stops. (For example, a heart muscle fiber stops beating in 60 seconds after
cessation of blood flow).
The lethal chain of events probably begins with the switch to anaerobic metabolism. The increased
amount of AMP (from un-recycled ATP) stimulates anaerobic glycolysis (* AMP activates
phosphofructokinase -- what's the teleology?), glycogen is depleted, lactic acid (the end-product of
glycolysis) and phosphorus (from the ATP and other energy-rich phosphates) accumulates, and cell
pH drops precipitously, denaturing the proteins.
* Bio-philosophers: We could probably have avoided this process had we been designed to simply
shut our cells down when the oxygen supply becomes low. However, this would have made it
impossible to rescue ourselves from critical situations.
When the cell goes anaerobic, for some reason the cell membrane loses the ability to keep sodium
and water from diffusing in. Probably there is some hydrolysis of macromolecules right away, and
this increases the osmotic pull. Acute cellular swelling ("cellular edema") occurs. Much of this
fluid is in the endoplasmic reticulum, and this is seen as dilatation on electron microscopy. At the
same time, the sodium pumps fail for lack of ATP. Sodium enters the cell and potassium leaves.
Enzymes begin to leak from the cytoplasm into the bloodstream (see below).
All these changes have taken place in your skeletal muscles when you have exercised near your
limit.
Experimentalists: This is the stage at which trypan blue starts to enter "newly dead" cells.
* I hope the fad word "oncosis", mentioned in Robbins, never catches on as a
term for acute cell swelling.
* Fun to know: Among the most-conserved proteins over evolution are the "heat shock proteins",
which refold denatured proteins and get rid of those that cannot be salvaged. The prototypes are
ubiquitin and the chaperonins (the Hsp family). Whenever a cell is damaged, levels of these proteins
increase strikingly. Right now the whole family is "proteins in search of a disease"; there are some
interesting links.
Next, ribosomes start coming detached from the rough endoplasmic reticulum. "Big Robbins"'s
observation that "polysomes dissociate into monosomes" is just another way of saying that RNA
translation stops. Microvilli (if any) flatten, blebs form on the cell surface, and the membranes of
disrupted organelles form laminated ("myelin-like", alternating
layers of water and lipid) figures in the injured cytoplasm.
{17369} laminated "myelin figures" in cell injury; electron micrograph ("mb"="myelin bodies") (NOTE:
despite what anyone else may tell you, these do not
prove that the cell is injured irreversibly)
At this stage, chromatin clumping and nucleolar scrambling are visible by electron microscopy, but
not really by light microscopy.
Up through this point, all the changes are reversible if oxidative phosphorylation is restored. The
hallmark of early irreversible hypoxic injury is "calcification of the mitochondria".
The
mitochondria become permeable to calcium
("the mitochondrial permeability transition, other
stuff gets in and out as well)
, which precipitates with the local phosphates (ADP &
ATP, remember?) as an insoluble "amorphous density". This shuts them down permanently.
{17366} calcium precipitate within mitochondria
If you're interested in mechanisms of cell injury, pay attention to calcium as the likely mediator of
irreversibility.
More generally, hypoxic injury (with the drop in pH
and perhaps other reasons)
allows "escape of sequestered calcium into
the cytosol" (and surely also across the cell membrane from outside). Calcium is currently blamed
for activating endogenous phospholipases
(which damage membranes) and activating proteases
(notably the "calpains", which wreck the cytoskeleton and which can be inhibited; Proc. Nat.
Acad. Sci. 88: 7233, 1991) which damage diverse elements of the cytoskeleton. Remember you
also need ATP to continue the synthesis of membrane phospholipids; swelling of the cell might rip
the cytoskeleton off the membranes, damaging them; etc., etc.
Rigor mortis, following death, results when
ATP is depleted and (I suspect)
enough calcium has diffused into the damaged cells to
make the sarcomeres clamp shut for the last time. (Remember that it's entry of calcium that makes
sarcomeres contract in life.)
Around this time, the lysosomes also rupture and begin digesting the cell (with their DNAases,
RNAases, proteases, phosphatases, sulfatases, glucosidases, and cathepsins, enumerated in "Big
Robbins"). Obviously, once the genes have been sliced to bits, the damage is irreversible.
{17368} break in cell membrane, irreversible injury
Nuclear changes are the light microscopist's hallmark for irreversible injury. Pyknosis is a
shriveling and darkening of the nucleus attributed to very low pH. (RULE: If the nucleus is smaller
and darker than a resting lymphocyte's, or is small and dark and shows no euchromatin-heterochromatin textures, that cell is
very dead.) Later stages include karyorrhexis, or fragmentation
of the shriveled nucleus (into "nuclear dust"), and karyolysis, which simply means that nothing of
the nucleus is visible any longer, except perhaps a purple haze. {17374} nuclear pyknosis (arrows); be sure you can tell
a pyknotic nucleus from a live lymphocyte nucleus
Currently, there is considerable interest in free radicals (especially toxic oxygen radicals; see below)
as mediators of reperfusion injury, i.e., additional harmful things that occur only when blood flow is
restored to a damaged organ. Further, when blood flow is restored to damaged cells, the newly-available calcium
will pour
through the damaged cell membranes
and into the mitochondria, killing the cells even faster. And
later, the neutrophils, which fight disease using free radicals, accumulate at sites of tissue injury. Of
course, if blood flow is not restored, the tissues will die anyway.
Finally, once cell membranes are badly broken down, certain lipids act as detergents, further
disrupting the devastated cell.
NOTE: According to "Big Robbins", enzymes leak from the cell only when irreversible injury has
occurred. This is clearly wrong; mild reversible injury is quite sufficient to cause enzyme leakage.
These are the "liver enzymes", "cardiac enzymes", etc., that your lab measures to let you determine
the presence and extent of injury in the clinical setting. (Skeletal muscle enzymes rise after a
workout, and liver enzymes after a beer party, but in neither case is there microscopic
or clinical evidence of
cell death.)
FREE RADICALS
A common "final pathway" in a variety of forms of cell injury, including injury brought about by
inflammatory cells, is generation of free radicals, i.e., molecular species with a single unpaired
electron available in an outer orbital. Single free radicals initiate chain reactions that destroy
large numbers of organic molecules.
Notable results of free-radical generation:
1. Oxidation of unsaturated fatty acids in membranes ("lipid peroxidation", etc.) * Basic biologists:
These are the same reactions that make unsaturated fats turn rancid.
2. Cross-linking of sulfhydryl groups of proteins.
3. Genetic mutations.
Free radicals may be generated in the following ways:
1. By absorbing radiant energy (UV, x-rays; striking water, these generate a hydrogen atom and a
hydroxyl radical; when hydrogen peroxide contacts ferrous iron, it is cleaved into two hydroxyl
radicals (* the Fenton reaction).
2. As part of normal metabolism (for example, xanthine oxidase and the P450 systems generate
superoxide; our white cells use free radicals to attack and kill invaders)
3. As part of the metabolism of drugs and poisons (the most famous being CCl3.-, from carbon
tetrachloride; even O2 in high concentrations generates enough free radicals to gravely injure the
lungs).
The most important free radicals are probably those derived from oxygen, i.e., superoxide (O.-2) and
hydroxyl radical (OH.); hydrogen peroxide, though not a free radical, is two hydroxyl radicals
joined.
Lately we've also come to recognize the importance of nitric oxide in tissues;
despite its popularity with viagra users, it's a free radical
and generates even meaner free radicals (peroxinitrite, ONOO.).
We have only a limited ability to dispose of free radicals.
Certain molecules ("antioxidants") scavenge free radicals. Worth remembering are vitamin E,
sulfhydryl compounds ("Big Robbins" list cysteine and glutathione, as well as the drug
penicillamine), ascorbic acid (vitamin C; Ann. Int. Med. 114: 909, 1991), melatonin (Science News
114: 109, 1993) and the metalloproteins ceruloplasmin and transferrin. All except the drugs are
"endogenous antioxidants".
Superoxide is ordinarily detoxified by superoxide dismutase into H2O2. (* This protein is currently
sold as youth preservative pills. What's the fallacy?)
Catalase (in our peroxisomes, remember?) helps us by turning H2O2 into oxygen and water.
Glutathione peroxidase (a selenium-based enzyme -- * ask several health food store proprietors
whether selenium is "very good for you" or "very bad for you") greatly speeds the consumption of
free radicals by cross-linking sulfhydryl groups.
Whether or not you believe that free radicals explain aging, there is no doubt that they are
responsible for many of the genetic mutations that cause cancer and birth defects.
For your future reference: When a free radical chain reaction scrambles two C=C double bonds on
adjacent unsaturated membrane lipids, the resulting cross-linked mess is biologically inert and will
stay around forever, eventually being incorporated into the wear-and-tear pigment "lipofuscin".
This pigment also contains other un-digestible remnants. More about this later.
* Malondialdehyde in the urine is a traditional research measure of the extent of current whole-body
free radical production. People have been offering this as a marker for "oxidative tissue
damage" for the past 30 years without its becoming much accepted; part of the problem
is that it's also a normal by-product of prostaglandin metabolism.
CHEMICAL INJURY
Biological molecules react like any other chemicals. Acids and alkalies hydrolyze membranes, and
horrible poisons like mercuric ion tie up sulfhydryl groups and ruin the cell. Formalin /
formaldehyde crosslink amino groups on proteins and nucleic acids.
Other classic poisons affect the more vulnerable parts of the cells,
depending on the poison and dose, there may or
may not be necrosis:
Current thinking is that most simple nonmetallic
poisons that cause actual cell necrosis require activation to form
free radicals. For example, carbon tetrachloride (old-fashioned cleaning fluid) is turned into CCl3.-
radical in the smooth endoplasmic reticulum of the liver. Not surprisingly, the liver is damaged first,
as described in detail in "Big Robbins".
{07020} carbon tetrachloride toxicity to liver,
gross (widespread cell death shows as yellow, in the centers of the lobules)
Chemical injury fades into other types of biological injury in certain protease venoms (pit viper
poison, necrosis following a brown recluse spider bite).
{10658} snake and snake-bit foot
VIRUS-INDUCED CELL INJURY
Cytolytic viruses destroy cells, while cytopathic viruses alter their morphology without causing
necrosis. Viruses may also be produced by cells without any morphologic changes.
Viruses may kill a cell by scrambling the genes it needs to maintain its structure, or by multiplying
so fast that the cell explodes. Obviously, it is not really in the virus's interest to kill its host organism.
Cold viruses may scramble cilia, and pox viruses scramble cellular vimentin. Most interesting are
the "giant cells" that result when several virus-infected cells fuse. Viral inclusion bodies are
crystalloids of viruses in the nucleus and/or cytoplasm.
Further, the body's T-cells often attack cells that harbor viruses.
For example, the cell damage in hepatitis B is
brought about by T-cells, not viruses.
LIGHT MICROSCOPY OF CELL INJURY
The electron microscopic appearances of hurt cells described in "Big Robbins" reiterate the
mechanisms of cell injury. We rarely use electron microscopy in diagnostic pathology, but we often
examine cells.
Reversible cell injury has two morphologic hallmarks -- cell swelling and fatty change.
Cell swelling ("cloudy swelling"; the extreme forms are called "vacuolar degeneration" or "hydropic
change") is the visible change resulting from water being pulled by osmosis through damaged cell
membranes.
It is subtle, it does not alter cell shape much, and we will not expect students to diagnose
it. "Big
Robbins" notes that organs with extensive hydropic swelling will be heavy.
Good places to look for "cell swelling" include the renal tubules of patients on diuretics, and the
subendocardial myocardium of patients who died after hypotension of at least a few hours duration.
(Why?) The epidermal "balloon cells" of acute contact dermatitis are another good illustration.
Future pathologists: You'll use stains to distinguish "hydropic change" and glycogen accumulation
in heart and kidney.
{19358} hydropic change in epidermis in acute contact dermatitis
(perhaps poison ivy)
Fatty change occurs when cells that ordinarily take up a lot of lipid (heart, liver) cannot process it.
More about this later.
{08357} fatty liver, gross (yellow, felt greasy; you
would want to see the histology to make sure of the diagnosis)
Necrosis is the gross and light-microscopic appearances that indicate cell death. "Big Robbins"
gives two similar definitions back-to-back. (Purists will note that
"necrosis" actually occurs only after death. Every cell on a microscopic slide is
dead, but that only the necrotic ones were assuredly dead when the fixative froze their appearances
in time.)
How do you tell a cell is dead? For a moment, ignore the various types of longstanding necrosis.
(1) As it is dying, the cell cytoplasm becomes hypereosinophilic (loss of ribosomes, more exposed
arginine and lysine units binding eosin).
(2) If the cell was burning glycogen in life (heart, maybe liver), the glycogen is gone. This makes the
cell smaller, more homogeneous, and more pink-staining.
(3) Nuclear pyknosis, karyorrhexis, and karyolysis are the easiest ways to tell that cells are dead.
Later on, the cytoplasm starts looking "moth-eaten" as lysosomal enzymes digest the cell. By this
time, we stop talking about "dead cells" and start talking about "debris".
Words: Autolysis is the dead cell being self-digested by its lysosomal enzymes, while heterolysis is
the cell being digested by the body's living white cells. After death of the person, all the tissues
autolyze, and the skilled pathologist must distinguish these changes from necrosis during life.
(When there's antemortem necrosis, there's generally some vital reaction among the surviving cells,
i.e., inflammation, congestion, a recognizable pattern of infarction at the organ level, a thrombus,
etc., etc. More about this later.) Putrefaction is the lysis of dead tissue (part of a live body, or a
dead body) by bacterial enzymes, producing nasty smells. The champions are clostridia from the
bowel.
{07195} putrefied corpse from the woods
Types of necrosis is a topic that generates tremendous confusion among students. These patterns
are not hard-and-fast.
Coagulation necrosis: Death of groups of cells (most often from loss of blood supply), with
persistence of their shapes for at least a few days.
Grossly, the dead area is likely to be soft and pale. After a while, it is likely to shrink (catabolism)
and turn yellow (its lipids are freed up to form little micelles, trapping the tryptophan metabolites
that impart the yellow color to normal body fat).
You'll see coagulation necrosis when it is the
result of proteins being denatured (i.e.,
ischemia, extensive free radical injury).
Think of frying eggwhite.
The microscopy is distinctive. After loss of their nuclei, the cytoplasm of the cells remains intact for
days. The "tombstones" reveal the structure of the living tissue. If the patient lives, the edges of the
necrotic area become inflamed, and eventually the dead cells will be removed by white cells and
their noxious proteases. RULE: Unless otherwise specified in this section, the death of a group of
cells will result in coagulation necrosis.
Depending on circumstances, necrotic tissue may be walled off by scar tissue, totally converted to
scar tissue, get destroyed (producing a cavity or cyst), get infected (producing an abscess or "wet
gangrene"), or calcify. Of course, if the supporting tissue framework does not die, and the dead cells
are of a type capable of regeneration, you may have complete healing. You'll learn about all these
processes in the next few days.
Remember: True coagulation necrosis involves groups of cells, and is almost always accompanied,
after a day or so, by acute inflammation (next unit!)
Apoptosis ("shrinkage necrosis", "single-cell coagulation necrosis",
"natural death in contrast to necrosis")
is a distinct reaction pattern that represents
programmed single-cell suicide. Cells actually expend energy
in order to die.
(Reviews Science 292: 865, 2001; Science 293: 1784, 2001).
Everything about apoptosis:
JAMA. 279(4):300, 1998; Am. J. Med. 107: 489, 1999.
In apoptosis, the cell membrane does not rupture, the cell contents are not released into the
extracellular space, and inflammation does not occur.
Apoptosis is "the physiologic way for a cell to die", seen in a variety of circumstances.
Despite some writers' efforts to distinguish it from other kinds of necrosis,
it is often seen along with them when there is disease.
The basic biology of apoptosis is the same regardless of the circumstances:
1. The process often starts when a surface suicide receptor is stimulated (fas/Apo1 product, "the
death trigger", etc.; Nature 367: 317, 1994; J. Imm. 151: 621, 1993)
2. The common point-of-no-return seems to be leakage of cytochrome C from
the damaged mitochondria (Am. J. Med. Sci. 318: 15, 1999, lots more)
3. Endonucleases slice the genome between each pair
of nucleosomes (Am. J. Path. 136:
593, 1990) -- experimentalists see DNA ladders on agarose gel electrophoresis;
* One of the endonucleases comes from damaged mitochondria: Nature 412: 90 & 95, 2001.
4. A transglutaminase crosslinks glutamine and lysine units by their side-nitrogen atoms (this may
cause the edges of the cells to bleb and fragment);
5. A caspase degrades the cytoskeleton.
Cells connected to their neighbors (i.e., epithelial cells) detach cleanly as they die. The most famous
of these is the "Councilman body" ("acidophil body")
of viral liver disease. Apoptotic cells may be phagocytized by
their neighbors. Unlike coagulation necrosis and the other types of necrosis, there is never any
rupture of the cell membrane, the surrounding cells are alive,
and there is never any inflammation.
{05961} apoptotic hepatocyte ("Councilman body") in hepatitis B
(shrivelled, hypereosinophilic, separated from its neighbors)
* We now have special research techniques to show up, definitively, which cells are apoptotic in a
section. Most popular with the researchers
is "terminal deoxyribonucleotidyl transferased mediated
nick end labelling" (TUNEL). For the working pathologist,
there are immunostains, perhaps the best being an antibody
against cleaved caspase 3. Update Histopathology 44:
9, 2004.
Apoptotic nuclear pyknosis, karyorrhexis, and karyolysis look, morphologically, like what you see
in other necrosis. The difference is that apoptosis features individual cells dying off, and a lack of
inflammation.
A big topic right now is the triggering of apoptosis. Worth knowing:
The bcl-2 gene product inhibits apoptosis by coating
the mitochondria and not letting the cytochrome C out.
Mutant expressions
(as in
some cancers) prevent cells from dying when they should.
The fas ligand, when stimulated, triggers apoptosis.
When tumor necrosis factor (TNF) binds to its receptor (TNF ligand;
Nat. Med. 5: 157, 1999),
it stimulates apoptosis.
CTL-lymphocytes (killer "T"'s) trigger the fas ligand,
and also use perforin to pierce the cell membrane and
inject their granules, where granzyme B
activates the caspase.
The p53 gene product instructs damaged cells to undergo apoptosis.
This is the most common gene known to be
lost in aggressive cancers.
Other variants on coagulation necrosis:
One variant of coagulation necrosis is the contraction bands seen in dying heart muscle. These are
strips of cytoplasmic hypereosinophilia perpendicular to the long axis of the fiber (not to be confused
with cross-striations). They are typically the first light-microscopic indication of heart cell death,
and represent areas in which sarcomeres have clamped shut. (Some experimentalists attribute their
appearance to "reperfusion injury", with calcium entering the damaged cells. This seems very
reasonable.)
{06642} contraction band necrosis in heart
Coagulation necrosis of skeletal muscle fibers (or something very similar) is sometimes called
Zenker's hyaline change. Segments of individual fibers shrink and become hypereosinophilic.
Liquefactive necrosis (* "colliquative necrosis" in Europe): The result of hydrolysis. When the cells
die, they are rapidly destroyed by lysosomal enzymes, either their own or those from neutrophilic
leukocytes (i.e., bacterial infections), or clostridia or snake poison.
Acid and lye burns represent the extreme of liquefaction.
Also, if both neurons and glia are killed, dead brain liquefies rapidly.
Liquefactive necrosis that is caused by neurophilic leukocytes is called pus. The term may also
be used for an effusion that is full of dead neutrophils.
NOTE: The truism that "brain liquefies" is a common source of misunderstanding. Brain deprived
of its oxygen for a few moments will suffer neuronal damage but not necrosis. Brain deprived of
blood flow for a few moments longer will lose neuronal structure but not glia, and remain solid. The
same is true of diseases in which neurons die off one at a time (i.e., Alzheimer's disease causes the
brain to shrivel but not to liquefy). Only if the glia are killed does the brain melt away, and then
only after several days.
{17399} old liquefactive necrosis, brain, gross
NOTE: Menstruation actually involves liquefaction of the endometrium. Nobody talks about the
term in this way.
(Enzymatic) fat necrosis: When pancreatic enzymes are released into the body's tissues, they digest
them wholesale. Lipase releases free fatty acids (saponification)
from the local
lipids (membranes, depot triglyceride). This
complexes with calcium ions to form salts (calcium stearate, etc.) that are notoriously insoluble --
ask a plumber, or anyone who's had a bathtub ring or grunge after washing dishes in hard water.
Years later, survivors still have soap deposits in their insides.
Hematoxylin stains calcium very blue, and fat necrosis appears as blue cell ghosts on H&E stains.
The pattern is sufficiently distinctive from classic "coagulation" and "liquefaction" to merit a term of
its own.
{17404} enzymatic fat necrosis, gross; patches of white
calcium stearate
Non-enzymatic "fat necrosis" can also follow physical
injury (remember a blow to the breast) or hypoxic injury to
a newborn (you'll see this under the skin), and freed fats
can calcify.
Caseous necrosis (same root as "cheese" and "casein"): All of the cells
in an area die, the tissue architecture is obliterated,
and they turn into a crumbly ("friable"), readily-aerosolized powder.
This is characteristic of a poorly-understood subtype of immune injury, and generally it is seen in
certain granulomatous diseases, notably tuberculosis and certain fungal infections
(coccidioidomycosis, blastomycosis, and histoplasmosis -- you'll learn these later).
The cells appear to be undergoing mass apoptosis (Eur. J. Immunol.
27: 3182, 1997; Infect. Immun. 65: 298, 1997; J. Path. 191: 417, 2002; -- I predicted
this in 1986).
In the past few years, there have been some experimental work suggesting that the
macrophage-derived protein tumor-necrosis factor alpha ("cachectin") is the principal toxin that
causes cells to undergo caseous necrosis, especially in the presence of certain components of
mycobacterial cell walls (Immunology 77: 505, 1992; J. Immunol. 145: 149, 1990). We might
reasonably think that some substance from the micro-organisms potentiates
the effect of alpha-TNF on its apoptosis trigger. Experimental confirmation is
eagerly awaited.
But despite "Big Robbins", don't expect there
will always be a nice granuloma walling off the caseous debris -- especially TB in the
AIDS-and-homelessness era!
{08187} renal TB, good caseous necrosis (right side, left is normal)
Gangrene ("gangrenous necrosis") is not a separate kind of necrosis at all, but a term for necrosis
that is advanced and visible grossly. If there's mostly coagulation necrosis, (i.e., the typical
blackening, desiccating foot that dried up before the bacteria
could overgrow), we call it dry gangrene. If there's mostly liquefactive necrosis (i.e., the
typical foul-smelling, oozing foot infected with several different kinds of bacteria), or if it's in a wet
body cavity, we call it wet gangrene.
{17392} dry gangrene
Bacterial gangrene
occurs when the primary problem is infection by one or two strains of bacteria,
and widespread tissue necrosis occurs in short order. Examples:
Clostridial gangrene (including "gas gangrene"), a dread complication of dirty, blood-deprived
wounds. The clostridia digest tissue enzymatically and rapidly, often transforming it into a bubbly
soup, usually too fast for inflammation to develop. Minutes count.
Synergistic gangrene after surgery, a mixed infection with staphylococci and streptococci
Ulcerative gingivitis ("trench mouth"), caused by overgrowth of anaerobes in the mouths of stressed
people with dubious oral hygiene.
Noma, necrosis of the lower face and/or female genitalia, seen only in people who are
immunocompromised (usually from malnutrition).
* Fournier's gangrene, bacterial gangrene of the scrotum (the dreaded "black sack disease" -- no joke)
Cavitation results from removal of necrotic material (i.e., draining a huge abscess, coughing up
caseous debris in tuberculosis, physiologic removal of debris in a cerebral infarct, etc.)
Fibrinoid necrosis is a time-honored term for damage to the walls of arteries that allows plasma
proteins to seep into, and precipitate in, the media (some pathologists call this "insudation"). This is
a particularly unwholesome situation. You'll learn the common causes (notably malignant
hypertension and type III immune injury) later. It's hard to be sure that anything here is really dead,
but at least the intima must have been damaged.
{01917} fibrinoid necrosis, blood vessel, following radiation (fibrinoid is pink)
* Gummatous necrosis is, for our purposes, coagulation necrosis seen in granulomas in syphilis. I've
seen this only in study-sets.
* Necrobiosis is a curious term for necrosis of fibroblasts within
still-intact dense fibrous tissue. It's
characteristic of two lesions -- necrobiosis lipoidica and granuloma annulare.
NOTE: If a person dies of acute coronary insufficiency (i.e., a sudden drop in blood supply to the
heart triggered a fatal rhythm disturbance or pump failure), no necrosis will be found in the
myocardium at autopsy. This generates much confusion among non-pathologists.
But already it is time to depart, for me to die, for you to go on living; which of us takes the better
course, is concealed from anyone except God. -- Socrates To die will be an awfully big adventure!
Let us so live that when we come to die even the undertaker
will be sorry.
I am going to the great Perhaps.
-- Rabelais, last words
ALTERATIONS WITHIN IN THE LIVING CELL
Lysosomes: For some reason, "Big Robbins" reviews the basic cell biology of lysosomes here. It's
common (especially in full-type phagocytes) to see a bacterium or bit of debris within a
phagolysosome ("heterophagocytosis"). You may also see an organelle being digested within a
phagolysosome ("autophagocytosis"). A residual body is a phagolysosome filled with already-digested debris, and
in lysosomal storage diseases, they fill with metabolites that patients cannot
break down.
* Chloroquine raises the pH in lysosomes and renders
their enzymes less active.
Proliferation of smooth endoplasmic reticulum: Overgrowth of the drug-metabolizing equipment of
drug-exposed liver cells. (We prefer the term "proliferation" for this process, rather than
"hypertrophy" or "hyperplasia".) We can tell by the cell's light microscopic appearance, but we
won't ask you to do this.
Mitochondrial alterations are cited by "Big Robbins". Giant mitochondria are seen in alcoholic
(and
other) liver disease, odd mitochondria are hallmarks of certain muscle diseases, and occasionally
weird ones are seen in cancer.
More familiar is the process of "getting in shape" by physical conditioning. This process probably
involves increasing the numbers (or at least the efficiency)
of mitochondria in affected muscles. Conversely, in cells that are
wasting away ("atrophying", see below), mitochondria are few.
Certain cells become literally stuffed with mitochondria. In health, these include the apocrine sweat
glands of the armpits, and the "oxyphil" cells of the parathyroid glands. In disease, such cells are
generically called Hürthle cells or oncocytes (the latter, which means "swollen cells", is a terribly
confusing word.)
Cytoskeleton problems are currently under much study. For your reference:
Microtubules...
20-25 nm (* the vinca drugs used for chemotherapy bind these,
thus preventing mitosis from being completed)
Myosin...
15 nm (in muscle) or 8 nm (non-muscle)
Intermediate filaments...
10 nm
Actin...
6- 8 nm (* experimentalists: prevent these from forming
using cytochalasin B)
Chediak-Higashi syndrome is a genetic white cell disease in which microtubule protein fails to
polymerize. This isn't the whole story, since the major problem that these people have is failure of
lysosomes to fuse with phagocytic vacuoles.
Colchicine disrupts microtubules, while cytochalasin B disrupts microfilaments.
Defects in the dynein arms of the microtubules within cilia cause infertility in both sexes, problems
keeping the airways clean, and sometimes problems in getting the embryo's guts into the right places.
More on these ("Kartagener's syndrome" and others) later.
The intermediate filaments are supposed to keep organelles in their positions. They include keratin
(for epithelium; there are several subtypes), neurofilaments, glial filaments, vimentin (for
mesenchyme), and desmin (for muscle). Mallory's hyaline in the boozer's liver is scrambled
prekeratin, while neurofibrillary tangles in the brains of Alzheimer's patients and boxers are
composed of tau protein, a microtubule-associated protein.
* More than you ever wanted to know about the intermediate filaments, including mutations that
cause some of the hereditary skin diseases collectively called epidermolysis bullosa: Science 25:
799, 1992.
Even the cell membrane has its own underlying skeleton, including the protein spectrin, which when
deficient prevents the erythrocytes from assuming the forms of biconcave disks. (The patients have
hereditary spherocytosis, a fairly common disease. More about this later.)
DEVELOPMENTAL ABNORMALITIES: This covers a host of anatomic lesions in which "things
grew wrong". This is a terminology section.
Aplasia is the complete failure of an organ to form. (By a time-honored misuse, wipe-out of once-healthy bone marrow
is called "aplastic anemia").
{15939} kidneys never formed ("renal aplasia / agenesis"; organ block of newborn child; the kidneys
should be next to the small intestine)
Atresia is the complete failure of the lumen, or a portion of the length of the lumen, to form where it
should in a hollow organ..
Stenosis is a non-neoplastic narrowing of a lumen; it may be a birth defect, or acquired.
Not birth defects, but you need to know: Occlusion is the complete obstruction of a lumen that was
once open. Spasm is the narrowing or occlusion of a lumen due to inappropriate contraction of
smooth muscle, or the inappropriate contraction of skeletal muscle anywhere.
Hypoplasia is the failure of an organ to grow to normal size. (By another time-honored misuse,
bone marrow with too-few cells is called "hypoplastic", even if it was once normal). "Atrophy"
would be a better term.
{15632} hypoplasia of the nails (minor birth anomaly)
Local gigantism is just as it sounds (Dolly Parton, "Elephant Man", Nixon's masseters -- noted
syndrome, see J. Oral. Max. Surg. 52: 1199, 1994 -- others that you know).
Malformation: Something was shaped wrong since before birth.
Deformation: Something used to be well-formed, but its shape was permanently altered, other than
by being cut apart.
You are welcome to call both malformations and deformations "deformities".
Syn- and holo- are prefixes that indicate failure to separate ("syndactyly" is fused fingers;
"holoprosencephaly" is a brain without divided hemispheres). Failure to fuse has no special word
root, but is also important ("hypospadias" is failure of a male's urethra to fuse; "harelip" you know).
Supernumerary organs often recall those of other animals (very common are supernumerary nipples
-- who's got one? -- and the less-visible accessory spleens), or might-have-beens in the history of life
(polydactyly, i.e., six fingers on a hand, six toes on a foot).
Ectopia / heterotopia is a well-formed bit of organ in the wrong place. If it's tiny and trivial, it's a
heteroplasia (for example, the common sebaceous glands on the buccal mucosa, called "Fordyce
granules"). If it's big enough to interest a surgeon, it's called a choristoma.
Hamartomas ("ectopias") are the right components of an organ in the wrong arrangement. The best-known hamartomas are
the vascular and pigmented birthmarks, and most "benign tumors of blood
vessels" are really hamartomas.
Like "real tumors", hamartomas can be clonal, indicating origin from a single mutated cell post-lyonization: Am. J. Path.
148: 1089, 1996. If you do not remember what lyonization is, you had
better review.
{05756} cartilage hamartoma, lung (trust me; your
lung is supposed to contain cartilage, in its bronchial walls,
but not a cartilage golfball like this)
Cysts are abnormal, closed, fluid-filled structures. Most definitions also stipulate that they be lined
by epithelium (I'd consider those that don't to be wrong). Many (but by no means all) cysts are
developmental defects, left over from embryogenesis.
* In due time, you'll learn about "retention cysts" (resulting from plugged ducts), "implantation
cysts" (after a bit of epidermis grows within the dermis following trauma), "hydatid cysts" (brood
cavities for tapeworms), "hyperplastic cysts" (i.e., part of the common, banal "fibrocystic disease of
the breasts"), cysts that form within tumors, "pseudocysts" (large cavities lined by partially-digested
fat cells), and "cystic changes" resulting from liquefaction necrosis in brain, mesenchymal tumors, or
elsewhere.
{25559} mucous cyst, within the lip
Fistulas are abnormal openings between body surfaces. Sinuses, when abnormal, are pathological
openings from a fluid-containing cavity
onto surfaces. If they're present for more than a very short time, each will epithelialize (of
course, why?) Either may sometimes represent a developmental defect.
{49228} anal fistula
A diverticulum is an outpouching of the entire wall of a tubular organ. This is most often a birth
defect or the result of something pulling on the side of the tube for a long time.
A pseudodiverticulum is an outpouching of the mucosa through a weakness in the wall of a tubular
organ. This is most often the result of too-high pressure for too long in the lumen.
ATROPHY: "Shrinkage in the size of the cell by loss of cell substance" ("Big Robbins"), without
the cell actually dying. When many cells each become smaller, the organ itself become smaller.
Defined this way, atrophy is very reversible.
Examples of real atrophy are:
Wasting of skeletal muscle on disuse (casted extremity, couch potato); wasting of a bed-ridden
patient's myocardium
{14424} atrophy of type II fibers in a couch potato
Loss of innervation of skeletal muscle (polio, nerve damage, nerve disease)
* The molecular biology, which of course involves inhibition of RNA transcription, is just now being
worked out (Proc. Nat. Acad. Sci. 91: 3647, 1994).
Diminished blood supply (various organs -- this includes "pressure atrophy") or inadequate nutrition
(various organs).
Loss of endocrine stimulation. This is very important; most organs that depend for their function on
endocrine stimulation (adrenals, testes, a man's skeletal muscles) will diminish in size if the
stimulating hormone is no longer available.
{17447} atrophy of thyroid (left; right side is normal thyroid at much lower magnification)
"Aging" is cited by "Big Robbins", though I am not impressed that geriatric cases have appreciably
smaller cells when all other things are equal. Cell loss is probably most of the story. Purists use the
term "involution" for decrease in cell or organ size as a result of the aging process (i.e., "the thymus
undergoes involution later in childhood").
Atrophic cells have fewer organelles and do not function as well as their normal counterparts. As
cells atrophy, their lysosomes consume their organelles. Again, some of the debris is non-digestible
and ends up as lipofuscin -- contributing to "brown atrophy".
Especially when the cause of atrophy is inadequate blood supply or nutrition, the atrophic cells may
go on to die and be replaced by scar tissue and/or fat. Probably in all the cases listed above except
for skeletal muscle, there is loss of individual cells.
{10247} atrophy of a kidney supplied by a narrowed artery ("ischemic atrophy")
Looser usage allows the word "atrophy" to be used for widespread loss of cells (usually by
apoptosis, if you catch them dying at all), without shrinkage of survivors. This misnomer has been
hallowed by long tradition when applied to the brains of heavy drinkers, Alzheimer's disease, and the
elderly.
{10847} brain "atrophy" (wide sulci, narrow gyri)
Another classic misuse is "atrophy of the testes" seen in dudes on anabolic steroids, which suppress
LH production by the adenohypophysis. So they lose their germinal epithelium (which accounts
for most of the mass of a man's testis.) Or following torsion or mumps. Wait until the male
contraceptive pill becomes available....
{10898} "Testicular atrophy", gross, with a normal for comparison
Bone marrow becomes less cellular in old age and in some illnesses.
{39457} bone marrow "atrophy"; only 20% of the marrow is hematopoietic cells, 80% is fat
And we routinely talk about "atrophy of the caudate nucleus in Huntington's chorea", "atrophy of
the exocrine pancreas when the duct is obstructed", etc., etc., etc., when we really mean loss of cells
instead.
{15426} atrophy of the gastric fundus mucosa in an elderly patient; smooth, shiny (i.e., thin
epithelium), no rugae
Now is as good a time as any to introduce cachexia, catabolism of body tissues, mediated by the
cytokines (substances by which white blood cells talk to one another and to the surrounding tissues).
You have probably already seen a cachectic cancer or AIDS patient, the most familiar situations.
The muscles of the body, and some other important tissues, are destroyed and energy liberated while
the fat is not burned. Widespread apoptosis may be taking place as well, especially in AIDS.
You can distinguish cachexia from marasmus (total-calorie malnutrition) because of selective loss of
muscle rather than fat. You can tell it from kwashiorkor (protein malnutrition, not exactly rare,
either) by the absence of fatty change in the liver. More about this later.
Cancer and AIDS patients are also likely to have poor appetites and to be low on fat as well; adults
may weigh as little as 60 lb. when they finally die, and death itself may be due to loss of the muscle
strength necessary to cough or even breathe.
HYPERTROPHY: Increase in the sizes of cells, and hence the size of the organ.
There are only a few examples:
Hypertrophy of the muscles of a strength athlete
{18668} "built up"; hypertrophied muscles
* Hypertrophy of the muscles of a person with a birth defect causing increased muscle tone
("myotonia congenita", not very serious)
Hypertrophy of the overworked heart of an aerobic athlete, hypertension victim, or victim of aortic
valve stenosis or other cardiac structural defect.
* Abnormal hypertrophy is critical to the development of common
congestive heart failure. Different genes are activated, and these may
become targets for therapy (Nat. Med. 11? 877, 2005.)
* Hypertrophy of the muscles of a person or animal deficient
in myostatin, a protein responsible for the atrophy of unused muscle
{03347} cardiac hypertrophy (either side, normal in center; the giveaway is the giant nuclei)
Hypertrophy of heart or skeletal muscle fibers, when their neighbors have been lost to disease.
Not surprisingly, there are genes, at least in cattle (J. Animal Sci. 76: 468, 1998)
and mice (Nature 387: 83, 1997, growth factor alleles),
to have more or less hypertrophied muscles; these are now being
discovered in humans to explain the
natural differences in muscularity. (* Angiotensin-converting enzyme: J. Clin.
Endo. Metab. 86: 2200, 2001).
* Certain angiogensin converting enzyme alleles
promote both muscularity (good) and early
hypertension (bad). Stay tuned.
Hypertrophy of portions of the heart in people who have inherited an abnormal beta-myosin gene
("Reggie Lewis's disease", much more on this later.)
Hypertrophy of the smooth muscle cells of the uterus in pregnancy (also undergo hyperplasia, see
below)
Most endocrine organs, when stimulated for a long time, show some cellular hypertrophy.
Hyperplasia is the predominant change.
* Hypertrophy of astrocytes when the brain is damaged.
* Hypertrophy of the good liver cells while the liver is repairing itself.
* Hypertrophy of liver cells bearing increased smooth endoplasmic reticulum, i.e., in response to medications
that stimulate the P450 system.
* Nobody says this, but the fat cells in an overweight person are technically hypertrophic (unless you
define hypertrophy to be increase in cell size due to more functional units.)
It's no surprise that cells undergoing hypertrophy have "increased protein synthesis", increased
numbers of organelles, etc. We have almost no understanding of the mechanisms of hypertrophy, or
its limits.
Hypertrophic cells, especially in the heart and endocrine glands, tend to become hyperploid. Cardiac
muscle cells, normally tetraploid (did you know that?) become octaploid or 16-ploid. Endocrine cell
nuclei become very large, etc., etc.
* "Big Robbins" makes the artificial distinction between "pathologic" and "physiologic" hypertrophy
(which is surprising for a text which considers healthy and bad adaptations to be on a "continuum").
We discourage the use of "hypertrophy" as a generic term for any increase in size of an organ, in the
absence of significant increase in cell size ("benign prostatic hypertrophy"; skin calluses as
"hypertrophy", etc.)
"When
an organ by increasing the number of its cells" -- R&F. This may be physiologic
(ignore "Big Robbins's distinction of "compensatory" and "hormonal" --
in health, it's probably all hormonally mediated), or pathologic
(i.e., the result of genetic mutations or environmental changes).
Examples:
The female breast at puberty -- under the influence of estrogens -- and during pregnancy and
lactation (additional hormones). (NOTE: The breast also undergoes hypertrophy.)
{49360} idiopathic "hypertrophy" of one breast. Actually, this is probably the result of an embryonic mutation, hence best considered a neoplasm.
The endometrial glands and stroma during the menstrual cycle
The male breast in cirrhosis or estrogen therapy, or in some boys at puberty ("gynecomastia") -- all
reflect estrogens
Lymph nodes in response to infection
The callused skin of a laborer's hand (in addition to more keratin, the epidermis itself thickens)
Smooth muscle cells in the pregnant uterus (also undergo hypertrophy)
Adrenal cortex in response to extra ACTH ("stress", ACTH-producing tumor, defective cortisol
synthesis)
{09217} adrenal cortex ("stressed"; compare a normal, otherwise this is hard to appreciate)
Renal tubules in the remaining kidney following removal of the other -- mechanism unknown
Bone marrow normoblasts ("erythroblasts", "baby reds") following hemorrhage -- under the
influence of erythropoietin
Bone marrow myelocytes in response to infection -- under the influence of colony-stimulating factors
Leydig cells in the testes of men with Klinefelter's syndrome or elderly men -- they don't produce
much androgen, so high gonadotropin levels drive them to multiply.
{24694} testis with Leydig cell hyperplasia (the cells between the tubules with the abundant
eosinophilic cytoplasm; this shows lots too many of them)
Thyroid cells under the influence of hTSH ("epidemic goiter", due to iodine deficiency),
autoimmune stimulation of hTSH receptors ("Graves' disease"), or unknown factors ("idiopathic
goiter")
Thyroid cells in response to type V immune injury with stimulation of hTSH receptors ("Grave's
disease")
Parathyroid cells in renal failure
{49450} parathyroid gland hyperplasia (they're big, trust me)
Bladder epithelial cells in bladder infections -- mechanism unknown
Endometrial cells in illness -- under the influence of unknown factors ("hyperplasia of the
endometrium", an important cause of irregular bleeding)
{49376} endometrial hyperplasia (uterus has been opened anteriorly;
the hyperplastic endometrium appears as a blob)
The prostate in old men -- under the influence of unknown factors (or perhaps genetic
programming).
{10743} prostatic hyperplasia (paper clip demonstrates urethral stenosis)
{24827} sebaceous gland hyperplasia
* Epidermis overlying certain curious dermal lesions (blastomycosis, granular cell tumor) -- this
"pseudoepitheliomatous hyperplasia" looks grossly and microscopically like cancer.
Various tissues under the influence of drugs
* The islets is Langerhans after gastric bypass surgery for
weight reduction. Figure THAT one out! NEJM 353: 249, 2005.
{25557} hyperplasia of gingival tissue in a patient receiving phenytoin ("Dilantin") therapy (this is often misnamed "hypertrophy")
Contrary to what you have been told, the heart muscle cells undergo hyperplasia rather than
hypertrophy in the remodelling, failing hearts of the elderly: J. Am. Coll. Card. 24: 140, 1994;
and after myocardial infarction. Update Lancet 363: 1306, 2004.
Also contrary to what you've been told, there is some cell division in the skeletal muscles of
bodybuilders that remains when the gymrat lays off but enables more rapid gains on resumption of
exercise ("Muscles have a memory"). It is much less important than the hypertrophy.
Various tissues where a gene has mutated and given the cell a growth advantage over its neighbors,
but in which the cells still appear more or less normal (for example, pancreas Cancer 92: 1807, 2001 &
Am. J. Path. 144: 889,
1994; lung J. Clin. Path. 54: 257, 2001 &
Virch. Archiv. 424: 129, 1994; bladder 89:
514, 2000; parathyroid Am. J. Path. 147: 1600, 1995).
NOTE: Significant hyperplasia usually doesn't happen in neurons, cardiac/skeletal muscle (except
as noted above), or cartilage; because these cells are usually incapable of division.
* When the hyperplasia is useful, textbooks call it "physiologic", and make the distinction between
"hormonal" (part of growing up) and "compensatory" (in response to injury). When the hyperplasia
isn't useful, the books call it "pathologic". These distinctions are artificial and not necessary to an
understanding of the processes. Probably the physiologic hyperplasias don't result from mutations.
Notice that most hyperplasias seem to result from hormonal stimulation. As a rule, when the
hormone is removed, the hyperplasia quickly reverses.
Of course, hyperplasia resulting from genetic mutations conferring a growth advantage will not
reverse, and are a step in the development of cancer.
METAPLASIA: "(Adaptive) substitution of one type of adult or fully differentiated cell for another
type of adult (or fully differentiated) cell" -- Baby Robbins. "A reversible change in which one adult
cell type replaced by another adult cell type." -- Big Robbins. "Conversion of a differentiated cell
type into another" -- R&F.
Examples:
Replacement of airway pseudostratified mucin-producing ciliated columnar epithelium by stratified
squamous epithelium (cigaret smokers -- "to protect our delicate tissues from the harsh effects of
smoke").
Your lecturer remains skeptical about the "protective effect" of this metaplasia, since you seldom
see it fully expressed in casual sections of smokers' lungs, though it's the norm next to squamous-cell lung cancers. Actually,
it's most likely
due to mutations. More about this later.
Transformation of the gallbladder or urinary bladder epithelium to stratified squamous epithelium
in the presence of foreign bodies (stones, schistosome eggs)
Replacement of airway pseudostratified mucin-producing ciliated columnar epithelium by an
epithelium consisting almost entirely of goblet cells (cigaret smokers and asthmatics)
Replacement of the columnar mucoid epithelium of the endocervix by stratified squamous
epithelium in women infected with wart virus
Replacement of most columnar and transitional epithelium by stratified squamous epithelium, and
replacement of corneal epithelium by heavily-keratinized epithelium (vitamin A deficiency)
Replacement of fibrous tissue by calcified bone (many scars, which in the real world may be
considered "normal")
Replacement of laryngeal, tracheal, and costal cartilages by bone (old age)
Replacement of normal gastric epithelium with intestinal epithelium in stomach disease
("intestinalization")
{15432} stomach mucosa with intestinal metaplasia (right;
there's a bit of dysplasia/anaplasia as well); normal at left
Replacement of transitional bladder epithelium by mucin-producing epithelium ("cystitis
glandularis", a misnomer since there's no inflammation)
Replacement of flat simple squamous epithelium by cuboidal epithelium (damaged alveoli, hurt
mesothelial surfaces). This is temporary and is a stage in repair -- you can call it "metaplasia" if you
want.
Development of bone, often complete with hematopoietic marrow, within a blind, shrunken eye.
* Development of bone in the corpus cavernosum following papaverine treatment of impotence (J.
Urol. 142: 1323, 1989)
Replacement of columnar epithelium by squamous epithelium in the prostate, under the influence of
exogenous estrogens (administered for the treatment of prostate cancer) or adjacent to an infarct.
Replacement of squamous epithelium by columnar (gastric-type) epithelium in "Barrett's"
esophagus, caused by reflux-and-repair in the presence of some genetic mutations that give
a growth advantage to stomach-type cells
{19453} columnar metaplasia ("Barrett's" change) of esophageal mucosa (note the goblet cells)
Just how "adaptive" these changes are seems extremely dubious, but all are metaplasia.
Some epithelial metaplasias are reversible if there is an
identifiable stimulus that can be removed (which is rare).
Mesenchymal metaplasias (despite "Big
Robbins") are probably not reversible. Ignore anything that anybody may tell you
about "metaplasia by definition is reversible".
As with hyperplasias, certain metaplasias (notably, most Barrett's esophagus and many gastric
intestinalization cases) result from mutated genes that have given a clone of cells a growth
advantage over their neighbors. Of course, these are irreversible.
DYSPLASIA ("atypia", "atypical hyperplasia", "pre-cancer", etc.): "Bad growth".
By convention today,
used today, this implies a very abnormal epithelium
with "loss of uniformity of the individual cells, as well as a loss
of their architectural orientation". This includes "atypical hyperplasia" and "atypical metaplasia"
as well as the unfortunately-named newer term "intra-epithelial neoplasia".
Unqualified, "hyperplasia" and "metaplasia" imply the tissue cells look normal. In dysplasia, they
look distinctly abnormal, and the changes resemble those seen in cancer cells. These
weird changes are called ANAPLASIA. Look for:
Cells of varying sizes and shapes, lying topsy-turvy (i.e., the cells have forgotten how to be good
neighbors)
Less of the familiar differentiating features appropriate for the organ (i.e., the cells are forgetting
what to do)
Large, dark-staining nuclei with irregular surfaces (i.e., there's too many chromosomes, and the
nucleus doesn't know how to pack them all)
Increased nuclear-cytoplasmic ratio ( N/C ratio; i.e., there's a surplus of chromosomes and/or
they've forgotten to make enough cytoplasm)
Frequent mitotic figures (but no really weird ones) -- often away from the basement membrane (i.e.,
at least some of the normal controls on cell division are suspended)
It might be reasonable to consider that "metaplasia involves the cytoplasm; dysplasia requires
abnormal nuclei". The changes listed above are collectively called anaplasia ("grow-down", "funny-looking cells").
The abnormal nuclei are the easiest way for the beginning to recognize anaplasia.
We'll see them again, much more vicious, in the discussion of full-blown cancer.
* Virchow coined the terms "hypertrophy" and "hyperplasia". He called metaplasia "histological
substitution", and called anaplasia / dysplasia "pathological substitution", and of course
related the latter to cancer.
All dysplasias result from genetic changes that give cells a substantial growth advantage. The
changes cited above are the result of these changes.
Ongoing injury (cigaret smoking, ulcerative colitis, reflex of acid into the esophagus) promotes the
dysplastic process by causing increased cell division for repair. So the bad
genes have a chance to propagate.
Examples:
A pre-cancerous Pap smear (dysplasia at the squamo-columnar junction of the cervix,
with HPV infection an important part of the process)
{11490} dysplasia in the endocervix (upside-down; note N/C ratio, hyperchromatic cells, mitotic
figures off the basement membrane)
Ugly cells in the metaplastic bronchial epithelium next to (or a year prior to) an invasive lung cancer
Chaos in the colonic epithelium in a long-term sufferer from ulcerative colitis
Chaos in a "benign colonic tumor" that was removed for fear it would become malignant
{11484} dysplasia in a colon polyp (note N/C ratio, crowding, loss of mucin production)
Chaos in the mucosa of the stomach in a patient at risk for stomach cancer
{15441} dysplasia in gastric mucosa (note N/C ratio, cells lying topsy-turvy)
Chaos in the urothelium in a patient with a frank bladder cancer elsewhere
{25297} urothelial dysplasia / maybe even carcinoma in situ (note N/C ratio, very large and
hyperchromatic nuclei, topsy-turvy arrangement)
Red or white spots in the mouth of a tobacco-chewer -- when biopsied, the pathologist says
"pre-cancerous"
Weird cells adjacent to an invasive prostate cancer: Hum. Path. 22: 644, 1991.
While dysplasia is supposedly "reversible", it is common for cancers to arise here. The borderland
between dysplasia and cancer is carcinoma in situ (better, "intraepithelial carcinoma"). Much more
about this later.
{08911} carcinoma in situ of the endocervix, replacing epithelium and growing into a fold
* Ignore anything you may read in older textbooks about "teleology of dysplasia"; the process is
NEVER useful.
IMPORTANT NOTE: It is now abundantly clear that atrophy, hypertrophy, hyperplasia, and
metaplasia are all mediated, at least in part, by the same growth-and-differentiation genes ("proto-oncogenes") that function
abnormally in dysplasia and cancer. By now, there are a tremendous number
of examples, and I can share only a few.
* Healthy Harvey-ras mediates at least some of the hypertrophy of
cardiac muscle in response to
epinephrine and work (J. Clin. Invest. 89: 939, 1992); the gene product may work in part by turning
on the fos gene (J. Biol. Chem. 268: 2244, 1993). Activated ras alone produces prostatic
hyperplasia, at least in models (Cell 70: 153, 1992). Mutated Kirsten-ras begins to appear in
dysplastic colon epithelium in ulcerative colitis (Gastroent. 102: 1983, 1992), and premalignant
hyperplasia of the pancreas (J. Path. 186: 247, 1998). ras is among the
most-mutated genes in full-blown cancer, and some types of cancer always feature a mutation here.
*
A heavily worked skeletal muscle fiber expresses a tremendous amount of
myc product within a few hours (Biochem. J. 281: 1433, 1992), as an early step in the process of
undergoing hypertrophy.
* In squamous metaplasia adjoining squamous cell carcinoma of the bronchus, the over-expression of
myc and p53 match the cancer (Lab. Invest. 68: 26, 1993).
Much, much more about this soon. When a mass has formed, i.e.,
when bizarre cells have figured out a way to
grow their own
blood supply, we talk about a new growth, i.e., NEOPLASIA.
Anaplasia is ugly cells, whether confined to an epithelium (dysplasia) or invading (cancer / malignant neoplasia).
Dysplasia is pre-cancer. Dysplasia is anaplasia confined to an epithelium
and not yet invading. It is not yet really neoplasia.
If a neoplasm exhibits anaplasia, it is malignant (i.e., it is cancer), it will
invade, and it will spread.
If a neoplasm does not exhibit anaplasia, it is benign,
and will compress surrounding structures but will
not invade of spread.
Well, usually. Stay tuned.
LOOKING AT ORGANS: You learn by doing.
-- Goethe Consistency
Soft:
Like your earlobe. Think of fat, lung, edematous loose connective tissue, pus, tumor with scanty
stroma ("small blue cell" tumors, sarcomas)
Firm:
Like your strongest, leanest muscle when you flex it. Most pathology specimens are mostly firm.
Hard:
Like your knuckle. Think of bone, other calcified tissue, over-fixed dense connective tissue.
Remember the normal consistencies of organs, and that fixed organs are harder than unfixed ones.
Color
Red...
Fresh blood or fresh myoglobin
Red-orange... Bilirubin; hemosiderin (sometimes)
Orange... Carotene
Yellow... Lipid (adipose tissue; adrenal cortex; most necrosis); elastic fibers (vessels; yellow ligaments)
Green... Biliverdin (formalin fixation reduces bilirubin to biliverdin)
Blue... Something non-white seen through a reflective surface (blood in your veins through your skin;
carbon pigment under the pleura; blue iris; cornea in type I osteogenesis imperfecta).
Purple... ???
White... Tumor; granuloma; collagen (fibrous tissue; scar; etc.); calcium flecks
Gray... Lung alveolar tissue with some carbon
Brown... Feces; hemosiderin; lipofuscin; melanin; cytochromes (as in the liver); formalin-fixed or stale
hemoglobin/myoglobin; debris
Black... Carbon ("anthracotic pigment"); very abundant melanin; homogentisic acid ("alkapton"); formalin-fixed hemoglobin
turns dark
brown or black; dry gangrene
LOOKING AT CELLS
In your histology course, you learned basic light-microscopic anatomy, techniques of slide
preparation, and microscope use.
In this course, you will need to be able to tell what a cell was doing at the time it went into fixative.
Busy cells tend to have large nuclei and lots of euchromatin (since many of their genes are in use).
If they're synthesizing much protein, they will usually exhibit a nucleolus (where ribosomes are
made), and their cytoplasm will be bluish (from messenger, ribosomal, and transfer RNA).
Inactive cells will have smaller, darker nuclei and scanty cytoplasm. The body's least active cells
include the resting memory lymphocyte and the tendon fibroblast.
* For the curious: Heterochromatin is wound tight around nucleosomes. As genes are turned on, the
chromatin structure is remodelled (Nature 367: 576, 1994).
All nuclei don't look alike, and it's time to start noticing the differences. Soon, you'll even be able to
distinguish different kinds of white blood cells in tissue sections.
* PS: You'll learn "Death and the doctor" in other courses, i.e., how to break bad news, how to help
families, what problems they will face caring for a dying relative, and so forth. Don't expect
everybody to go through the classic five stages, especially where there is a living religious faith.
"Death education" isn't well done in most medical schools, at least the allopathic ones (Surgery 113:
163, 1993). Do yourself a favor and read a book by yourself over vacation.
If one person dies, it's a tragedy. If a million people die, it's a statistic.
Once the game is over, the king and the pawn go back into the same box.
O sons of men,
-- The Arabian Nights,
10th century
Life, like a dome of many-colored glass
In America today, the practices of medicine and law have so interfered with the dying process that
death has become a perversion of the natural process.
Nor dread nor hope attend
Socrates said, "O son of Hipponikos, the old proverb, 'Naught Without Labor' (chalepa ta kala), is
applicable to learning. And nomenclature is no small part of learning."
-- Plato, Cratylus
Life is a comedy to those who think, a tragedy to those who feel.
-- Horace Walpole
(usually misquoted and misattributed)
Chi-Lu asked Confucius how the spirits of the dead and the gods should be served. Confucius said,
"You are not even able to serve other living people. How can you serve the spirits?" "May I ask
about death?" said Chu-Li. "You do not understand even life. How can you understand death?"
-- Analects XI.12
To live will be an awfully big adventure!
-- Peter
Pan, last paragraph Get out! Get out! Last words are for fools who haven't said enough already!
{18601} skull, a familiar symbol of human mortality
 THE TESTABLE STUFF ON THIS HANDOUT STARTS HERE.
Scientific medicine is based around the concept of discrete diseases. This is the approach that works.
In today's world, only the charlatans and the fools deny that there are many distinct, identifiable
diseases with varying causes, or complain that studying disease objectively makes physicians care
less about "whole persons".
THE TESTABLE STUFF ON THIS HANDOUT STARTS HERE.
Scientific medicine is based around the concept of discrete diseases. This is the approach that works.
In today's world, only the charlatans and the fools deny that there are many distinct, identifiable
diseases with varying causes, or complain that studying disease objectively makes physicians care
less about "whole persons".
The most recent diatribe against the "disease model" is really
just about overtreatment
(Am. J. Med. 116: 179 & 186, 2004).
 The Greek word pathos actually covers a range of meanings from "experience" to "the human
condition" to "suffering", while nosos ("noxious", "nausea")
is the word for "disease" / "physically sick".
So Virchow's pathology considers
more than just the disease; we consider whatever human factors are involved, too.
The Greek word pathos actually covers a range of meanings from "experience" to "the human
condition" to "suffering", while nosos ("noxious", "nausea")
is the word for "disease" / "physically sick".
So Virchow's pathology considers
more than just the disease; we consider whatever human factors are involved, too.
Paleopathology is the study of disease as shown in human remains
from primitive societies. It's worth your attention, especially if you've
been told by an "alternative practitioner" that primitive people are amazingly healthy, or
have been taught in a left-wing college classroom that you shouldn't
appreciate today's scientific medicine and technology. (Uh, professor,
how would you like to die of a dental abscess as a young adult?)
 Skeletal analysis
Skeletal analysis
Nice introduction
British
 Paleopathology cases
Paleopathology cases
Virginia Commonwealth
For advanced students
Closed biopsy means the pathologist or clinicians put a needle
into the mass to obtain a few cells ("needle aspiration" or "aspiration biopsy")
or a bit of tissue ("needle biopsy" or "core biopsy").
* "The virtual autopsy", done by today's scanners, will probably
never replace the real thing as gold standard. Think about it: Science 302: 1890, 2003.
 Plague
Plague
Necrosis and more
French microbiology site
 HYPOXIC INJURY
HYPOXIC INJURY
* Less often, the nucleus may
become bloated with water ("degenerative nuclear swelling"), like the dying cell.
{17376} karyorrhexis / karyolysis (left half of field;
* this is TB)
{17379} dead renal tubular epithelial cells (within lumen of live tubule)
 Necrosis, nuclear changes
Necrosis, nuclear changes
Don't worry about the type of necrosis.
WebPath Photo
{07022} carbon tetrachloride toxicity to liver, microscopic (widespread hepatocyte loss;
note the paler centrilobular
areas where nothing is left except hepatic endothelial cells)
 Hydropic change
Hydropic change
Urbana Atlas of Pathology
{38782} fatty change in hepatocytes, oil red O stain;
note that
lipid vacuoles, being hydrophobic, are sharply demarcated from
the rest of the cytoplasm
{07021} putrefied corpse from the pond;
the tongue is swollen because of gas production postmortem
)window.location='http://www.pathguy.com/cob.jpg')
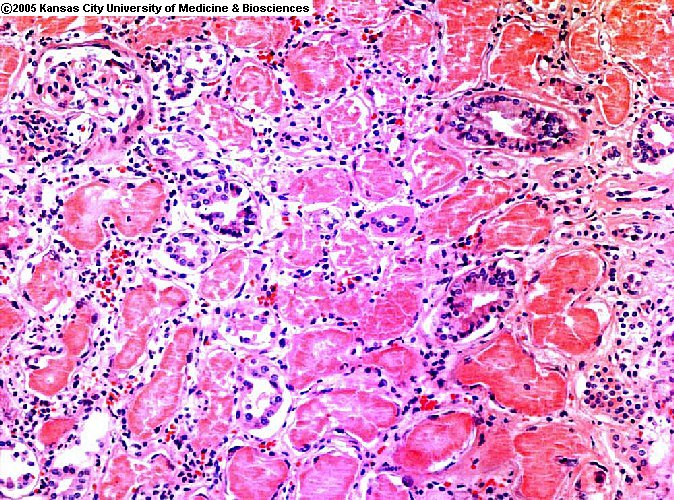 Coagulations necrosis
Coagulations necrosis
Proximal renal tubule
ERF/KCUMB
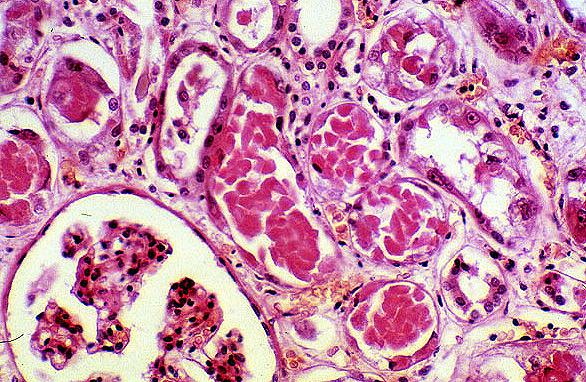 Mercury poisoning
Mercury poisoning
Striking coagulation mecrosis
of proximal tubules
KU Collection
Toxic epidermal necrolysis
Necrosis of the epidermis
Dermatlas
{39659} Necrosis of the hip, gross specimen with crumbling bone (Bo Jackson's disease)
{05956} Focal necrosis of hepatocytes. A glycogen-is-dark-red counterstain here makes the live
hepatocytes red, dead hepatocytes more pink
{08828} Widespread necrosis of hepatocytes; they're gone from most of the field, all that is left is
endothelial cells and Kupffer cells; there is a central vein in the center of the picture
{13320} Massive necrosis of the liver (limp liver;
nothing is left in the lobules except endothelial cells and reticulin)
{49266} Massive necrosis of the liver ("yellow atrophy");
we would want a histologic picture to confirm our gross impression
{13322} Massive necrosis of the liver with loss of most hepatocytes, histology, in fatal hepatitis
{16952} Necrosis of renal papillae (orange-yellow;
the bright yellow at the bottom is kidney fat)
{09578} Neuron, newly-dead ("red neuron")
{10571} Renal cortical necrosis (note yellow color)
{17389} Coagulation necrosis of renal tubules (left side)
* Your author is a Greek
language buff and since it's a real Greek word for "falling leaves", he pronounces both "p"'s like the
Greeks did, but some people say aa-poe-TOE-siss)
NOTE: There are surely other triggers. People with mutant fas
fail to rid themselves of autoreactive lymphocytes, but have normal fingers,
skin shedding, and so forth.
* Caspase inhibitors are now coming into clinical use to
prevent apoptosis, as for neuroprotection (Nat. Med. 5:
298, 1999; Science 288: 335, 2000).
 In apoptosis, the nucleus and cytoplasm condense (i.e., they shrivel and stain dark), and are likely to
fragment, but they will remain solid, and end up as mummified remnants ("apoptotic bodies").
In apoptosis, the nucleus and cytoplasm condense (i.e., they shrivel and stain dark), and are likely to
fragment, but they will remain solid, and end up as mummified remnants ("apoptotic bodies").
* Future pathologists: The chromatin in a cell
undergoing apoptosis tends to clump under the nuclear membrane, i.e.,
clockface.
{06651} contraction band necrosis in heart (there are also neutrophils)
Contraction bands.
Necrotic heart. Find them.
WebPath Photo
{17400} old liquefactive necrosis, brain, gross
Liquefaction necrosis
Pus pockets in the liver
WebPath Photo
Enzymatic fat necrosis
White flecks
WebPath Photo
{17403} enzymatic fat necrosis, microscopic (right side);
calcium imparts the blue tinge
{08348} enzymatic fat necrosis, microscopic (right side)
Caseous necrosis
TB -- it does look like cheese
WebPath Photo
)window.location='http://edcenter.med.cornell.edu/Pathology_Images/008.gif') Caseous necrosis
Caseous necrosis
At the center of a TB granuloma -- more about them later!
Cornell
{17395} pulmonary TB, caseous necrosis of the lung, gross
{17396} pulmonary TB, caseous necrosis of the lung, micro
(all is crumbly; on the left the nuclei are lost indicating that it is more advanced)
Exactly how anthrax toxin produces tissue injury is being worked out.
It includes an "edema factor" that causes cells to ooze their contents,
and perhaps this is why surface anthrax presents a black, dehydrated, dead "eschar".
Anthrax toxin: Nature 414: 225, 2001, Sci. Am. 286(3):
48, 2002.
{25451} dry gangrene
{25452} dry gangrene
{48075} dry gangrene
{48076} dry gangrene
{25453} early gangrene
{25454} wet gangrene (bacteria-rich)
{25455} gangrene of the toe, relatively early
{17393} gangrene of the bowel ("wet")
{10655} infarct of hand following embolus to brachial artery
{38590} gangrene of the fingers
Foot Gangrene
Australian Pathology Museum
High-tech gross photos
NOMA
World Health Organization
NOMA
Sarara marathon
{53545} fibrinoid necrosis, blood vessel, in a vasculitis syndrome
(fibrinoid is the pink center ring)
)window.location='http://edcenter.med.cornell.edu/Pathology_Images/034.gif') Fibrinoid necrosis; small patch of necrosis
Fibrinoid necrosis; small patch of necrosis
in a hypertensive's small renal artery
Cornell
-- Peter Pan (James Barrie)
-- Mark Twain
The boundaries that divide Life from Death are at best
shadowy and vague. Who shall say where the one ends,
and the other begins?
-- Edgar Allen Poe, "The Premature Burial"
* Amiodarone, the heart rhythm drug, binds to phosopholipids in
lysosomes and renders them insoluble.
 Syndactyly
Syndactyly
From a Saddam-era Iraqi
propaganda website (!)
Polydactyly
Skeleton
AFIP
 Polydactyly
Polydactyly
Source unknown
AFIP
{28889} cartilage and cuboidal cell hamartoma, lung, microscopic view (the right components,
i.e., cartilage and glands, but the
wrong arrangement)
{49278} bile duct hamartomas, liver (trust me)
{49638} cardiac muscle hamartomas ("rhabdomyomas", trust me), tuberous sclerosis patient;
identify the bumps without the normal heart muscle fiber pattern
{25560} mucous cyst, being excised
{25569} cysts of the breast
{09652} synovial cyst, ankle; it has been cut and the thick, gooey fluid has poured out
{12504} epidermoid inclusion ("sebaceous") cyst, beneath skin
{16982} polycystic kidney (football-sized; more about this later)
{16983} polycystic kidney
{49336} cyst of the epididymis (the testis is the white structure)
{49396} mucinous cystadenoma of the ovary; this might have weighed 30 pounds or more
{49471} thyroglossal duct cyst
{49472} thyroglossal duct cyst, filled with jelly-like thyroglobulin
)window.location='http://medic.med.uth.tmc.edu/edprog/Path/pedi/pedi-72.jpg') Polycystic kidney
Polycystic kidney
Note ruler
Texas A&M
{17445} atrophy of arm and chest muscles after nerve injury
{17446} atrophy of most muscle cells after nerve injury
{53704} atrophy of the left arm after a stroke
{14372} Werdnig-Hoffman disease of motor nerves; most muscle cells underwent atrophy
{25767} atrophy of a kidney supplied by a narrowed artery ("ischemic atrophy")
{17448} ischemic atrophy of renal tubules in a high blood pressure patient (left side)
{33047} ischemic atrophy of a cerebral hemisphere in chronic vascular disease
{34403} ischemic atrophy of a cerebral hemisphere in chronic vascular disease
{34478} brain "atrophy" (wide sulci, narrow gyri)
{34481} brain "atrophy" (wide sulci, narrow gyri)
{49554} atrophy of the cerebral peduncle following a stroke involving the motor cortex
{00086} "Testicular atrophy", adult man, no spermatogenesis whatsoever
Testicular atrophy.
Maybe mumps or old torsion.
WebPath Photo
{18642} "built up"; hypertrophied muscles
The left ventricle
of a healthy, sedentary adult human is never thicker than 1.5 cm.
{06380} cardiac hypertrophy (left), normal on right
{06383} cardiac hypertrophy (left), normal on right
{17454} cardiac hypertrophy (left), brown atrophy on right
 Myostatin-deficient cow
Myostatin-deficient cow
Muscle hypertrophy
Watch this one
* Gene activation as hypertrophy begins in heavily-worked muscle:
FASEB Journal 16: 207, 2002; J. Appl. Phys. 95: 1038, 2003; stain for myoD
to see whether muscles are bulking: Am. J. Phys. 278: C-1143 2000).
HYPERPLASIA: "An increase in the number of cells in a tissue or organ" -- Big Robbins.
Thyroid hyperplasia
in endemic goiter
Endometrial hyperplasia.
Latter portion of cycle.
WebPath Photo
Prostate hyperplasia.
Old guy. Lots of infolded glands.
WebPath Photo
 Sebaceous glands of the nose in rhinophyma ("W.C. Fields nose")
Sebaceous glands of the nose in rhinophyma ("W.C. Fields nose")
* It's now clear that the "stellate" muscle reserve cells contribute new nuclei
to the skeletal muscle fibers as they are being bulked (whether or not you're on
anabolic steroids: Med. Sci. Sports 31: 1528, 1999).
{19347} stomach mucosa with intestinal metaplasia (goblet cells, etc.)
Dysplasia, pap smear
Urbana Atlas of Pathology
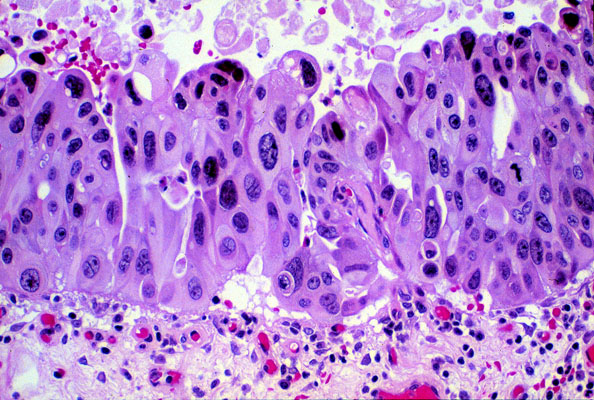 Bladder carcinoma in situ
Bladder carcinoma in situ
Very anaplastic, no invasion
KU Collection
 Anaplasia
Anaplasia
High-grade carcinoma
Dave Barber MD, KCUMB
{39605} dysplasia in the endocervix (note N/C ratio, failure of maturation)
{10079} carcinoma in situ of the bronchus
{11491} carcinoma in situ of the endocervix, replacing the columnar epithelium
You
see only what you know.
Savvy students seeing a gross specimen ask first, "Fresh or
formalin-fixed?"
Fresh will usually have red blood. Fixed will have the blood
dark-brown or black.
A healthy, sedentary 70 kg man who is killed
instantly in an accident will usually
have organ weights in these ranges:
Remember that the weight of the lungs can change by as much as a pound
in a few moments if (say) one of the mitral valve's papillary muscles
ruptures. Look at the appearances, consistencies and textures more than the numbers.
You can tell the nucleolus from the heterochromatin because
it's a little bit redder-staining and/or bigger and rounder.

-- Stalin
-- Italian Proverb
Lean death perches upon your shoulder
Looking down into your cup of wine,
Looking down on the breasts of your lady.
Your are caught in the web of the world
And the spider Nothing waits behind it.
Where are the men with towering hopes?
They have changed places with owls
Owls who lived in tombs
And now inhabit a palace.
Stains the white radiance of eternity
Until death tramples it to fragments.
-- Percy Shelley
-- Crit.
Care Clin. 9: 613, 1993
A dying animal;
A man awaits his end
Dreading and hoping all.
-- Yeats, "The Winding Stair"
It's interesting when you consider that the earth people
who can think are so frightened by those who cannot.
-- "Plan Nine from Outer Space"
--
Karl Marx's last words.
Medical mnemonics
Fun site maintained by
cyberfriend Robert O'Connor
 Autopsy
Autopsy
Dr. Evan Williamson,
then a medical student, dissects
Today's scientific pathology had its inception in 1859 with Virchow's work. For his time, Dr. Still's ideas about disease were reasonably enlightened. Today's oath of the osteopathic physician promises that physicians will work together in a spirit of "progressive cooperation", that they will "keep in mind always nature's laws", and that they will "further the application of basic biologic truths to the healing arts and to develop the principles of osteopathy which were first enunciated by Andrew Taylor Still."
This course will focus on understanding disease in light of nature's laws as they really are, i.e., the principles of rational inquiry, and the essentials of physics, chemistry, and basic biology. At the human level, your study of pathology will constantly correlate physical structure and the function of the human being at every level, just as Dr. Still tried to do in the late 1800's.
The oath also makes the promise that you will always "keep in mind... the body's inherent capacity for recovery." Most of pathology is the really study of this capacity. In this course, you will learn how and when the body tends to heal itself, and how it fights off infection and repairs wounds. You will always learn of situations in which the capacity to nourish and heal goes awry (atherosclerosis, hypertension, autoimmunity), situations in which some phase of the power to heal is lacking (hemophilia, immune deficiency), and situations in which the body does nothing to protect itself (prion disease, Huntington's disease). You will also learn how the body wears out (Alzheimer's disease), how damage accumulates and propagates itself (cancer), and how the body damages itself fighting invaders (suppuration, tuberculosis, rheumatic fever). You will come to understand when you can intervene with the expectation of curing, and when you can only palliate and help the person and family live with incurable illness.
Dr. Still believed that the principles of disease are relatively straightforward, and urged learners to use the hands-on approach. Your course features an abbreviated lecture series coupled to a whole-person oriented lab experience in which you will be continually active.
The osteopathic oath-taker also promises to "be ever vigilant in aiding the general welfare of the community." Since Virchow, pathologists have considered public health and the politics of disease to be part of our discipline. There may not be easy answers, but the content is important.
I would like to think that an osteopathic medical education offers a common-sense, humane, and rational basis for treating disease, not just a welter of scientific facts for doctor-technicians. This isn't just "pathology with an osteopathic spin". It is how I think the subject should be taught everywhere.


| Visitors to www.pathguy.com reset Jan. 30, 2005: |
Ed says, "This world would be a sorry place if
people like me who call ourselves Christians
didn't try to act as good as
other
good people
."
Prayer Request
 Teaching Pathology
Teaching Pathology
PathMax -- Shawn E. Cowper MD's
pathology education links
Ed's Autopsy Page
Notes for Good Lecturers
Small Group Teaching
Socratic
Teaching
Preventing "F"'s
Classroom Control
"I Hate Histology!"
Ed's Physiology Challenge
Pathology Identification
Keys ("Kansas City Field Guide to Pathology")
Ed's Basic Science
Trivia Quiz -- have a chuckle!
Rudolf
Virchow on Pathology Education -- humor
Curriculum Position Paper -- humor
The Pathology Blues
 Ed's Pathology Review for USMLE I
Ed's Pathology Review for USMLE I
![]()
![]()
 | Pathological Chess |
 |
Taser Video 83.4 MB 7:26 min |
 Necrosis I
Necrosis I
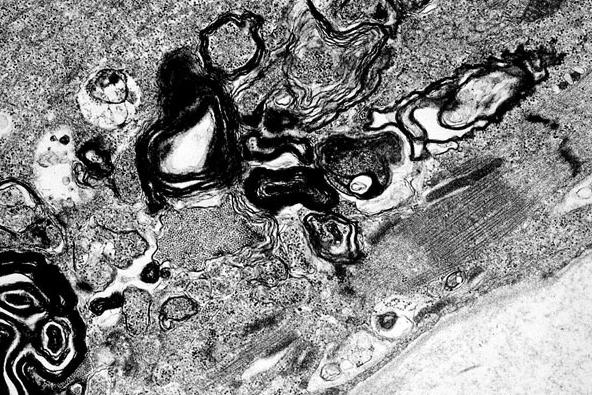 Myelin figures
Myelin figures)window.location='http://www.mdchoice.com/photo/img/img0032.jpg') Pit viper
Pit viper)window.location='http://www.mdchoice.com/photo/img/img0031.jpg') Pit viper envenomation
Pit viper envenomation)window.location='http://edcenter.med.cornell.edu/Pathology_Images/332.gif') Coagulation necrosis
Coagulation necrosis
)window.location='http://edcenter.med.cornell.edu/Pathology_Images/007.gif') Apoptotic cell (Councilman body)
Apoptotic cell (Councilman body))window.location='http://edcenter.med.cornell.edu/CUMC_PathNotes/Liver,GB,Pancreas/1913.gif') Apoptotic cell (Councilman body)
Apoptotic cell (Councilman body)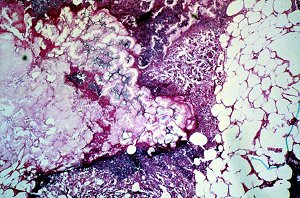 Enzymatic fat necrosis
Enzymatic fat necrosis)window.location='http://edcenter.med.cornell.edu/Pathology_Images/028.gif') Caseous necrosis
Caseous necrosis
 Tuberculosis
Tuberculosis)window.location='http://edcenter.med.cornell.edu/Pathology_Images/329.gif') Gangrene
Gangrene
 Anthrax
Anthrax Fournier's gangrene
Fournier's gangrene)window.location='http://edcenter.med.cornell.edu/Pathology_Images/295.gif') Fibrinoid necrosis
Fibrinoid necrosis
 Vascular adrenal cysts
Vascular adrenal cysts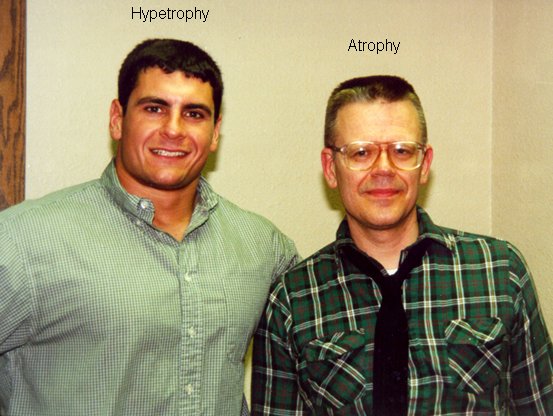 Hypertrophy and Atrophy
Hypertrophy and Atrophy)window.location='http://pathology.mc.duke.edu/neuropath/CNSlecture4/etohcerebellum.jpg') Superior vermal atrophy
Superior vermal atrophy)window.location='http://www.vetmed.wsu.edu/medsci520/images/ci/ci6.jpg') Metaplasia.
Metaplasia. Autopsy
Autopsy