Ed Friedlander, M.D., Pathologist
scalpel_blade@yahoo.com



Cyberfriends: The help you're looking for is probably here.
Welcome to Ed's Pathology Notes, placed here originally for the convenience of medical students at my school. You need to check the accuracy of any information, from any source, against other credible sources. I cannot diagnose or treat over the web, I cannot comment on the health care you have already received, and these notes cannot substitute for your own doctor's care. I am good at helping people find resources and answers. If you need me, send me an E-mail at scalpel_blade@yahoo.com Your confidentiality is completely respected.
DoctorGeorge.com is a larger, full-time service. There is also a fee site at myphysicians.com, and another at www.afraidtoask.com.
Translate this page automatically
 |
With one of four large boxes of "Pathguy" replies. |
 I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
Numbers in {curly braces} are from the magnificent Slice of Life videodisk. No medical student should be without access to this wonderful resource. Someday you may be able to access these pictures directly from this page.
Also:
Medmark Pathology -- massive listing of pathology sites
Freely have you received, freely give. -- Matthew 10:8. My
site receives an enormous amount of traffic, and I'm
handling about 200 requests for information weekly, all
as a public service.
Pathology's modern founder,
Rudolf
Virchow M.D., left a legacy
of realism and social conscience for the discipline. I am
a mainstream Christian, a man of science, and a proponent of
common sense and common kindness. I am an outspoken enemy
of all the make-believe and bunk that interfere with
peoples' health, reasonable freedom, and happiness. I
talk and write straight, and without apology.
Throughout these notes, I am speaking only
for myself, and not for any employer, organization,
or associate.
Special thanks to my friend and colleague,
Charles Wheeler M.D.,
pathologist and former Kansas City mayor. Thanks also
to the real Patch
Adams M.D., who wrote me encouragement when we were both
beginning our unusual medical careers.
If you're a private individual who's
enjoyed this site, and want to say, "Thank you, Ed!", then
what I'd like best is a contribution to the Episcopalian home for
abandoned, neglected, and abused kids in Nevada:
My home page
Especially if you're looking for
information on a disease with a name
that you know, here are a couple of
great places for you to go right now
and use Medline, which will
allow you to find every relevant
current scientific publication.
You owe it to yourself to learn to
use this invaluable internet resource.
Not only will you find some information
immediately, but you'll have references
to journal articles that you can obtain
by interlibrary loan, plus the names of
the world's foremost experts and their
institutions.
Alternative (complementary) medicine has made real progress since my
generally-unfavorable 1983 review linked below. If you are
interested in complementary medicine, then I would urge you
to visit my new
Alternative Medicine page.
If you are looking for something on complementary
medicine, please go first to
the American
Association of Naturopathic Physicians.
And for your enjoyment... here are some of my old pathology
exams
for medical school undergraduates.
I cannot examine every claim that my correspondents
share with me. Sometimes the independent thinkers
prove to be correct, and paradigms shift as a result.
You also know that extraordinary claims require
extraordinary evidence. When a discovery proves to
square with the observable world, scientists make
reputations by confirming it, and corporations
are soon making profits from it. When a
decades-old claim by a "persecuted genius"
finds no acceptance from mainstream science,
it probably failed some basic experimental tests designed
to eliminate self-deception. If you ask me about
something like this, I will simply invite you to
do some tests yourself, perhaps as a high-school
science project. Who knows? Perhaps
it'll be you who makes the next great discovery!
Our world is full of people who have found peace, fulfillment, and friendship
by suspending their own reasoning and
simply accepting a single authority that seems wise and good.
I've learned that they leave the movements when, and only when, they
discover they have been maliciously deceived.
In the meantime, nothing that I can say or do will
convince such people that I am a decent human being. I no longer
answer my crank mail.
This site is my hobby, and I presently have no sponsor.
This page was last updated February 6, 2006.
During the ten years my site has been online, it's proved to be
one of the most popular of all internet sites for undergraduate
physician and allied-health education. It is so well-known
that I'm not worried about borrowers.
I never refuse requests from colleagues for permission to
adapt or duplicate it for their own courses... and many do.
So, fellow-teachers,
help yourselves. Don't sell it for a profit, don't use it for a bad purpose,
and at some time in your course, mention me as author and KCUMB as my institution. Drop me a note about
your successes. And special
thanks to everyone who's helped and encouraged me, and especially the
people at KCUMB
for making it possible, and my teaching assistants over the years.
Whatever you're looking for on the web, I hope you find it,
here or elsewhere. Health and friendship!
A bone to the dog is not charity. Charity is the bone shared
with the dog, when you are just as hungry as the dog.
There is no love sincerer than the love of food.
-- Shaw, Man and Superman
If you say to people, "Go in peace, be warm and fed", but do
not give them what the body needs -- what good is it?
A hungry man is not a free man. If the misery of the poor be caused not by
the laws of nature but by our institutions,
great is our sin.
It is better to ask some of the questions than to know all of the answers.
QUIZBANK: Nutrition
LEARNING OBJECTIVES
Describe the causes, symptoms, signs, and impact of each of these epidemic deficiency diseases: Describe the anatomic pathology and pathophysiology
of obesity, and its real impact on health, distinguishing
fact from speculation and fiction.
Describe what is known, and what is not known, about the impact of diet
on cancer risk.
Describe the extent and impact of world hunger today, and trends
affecting the world food supply. Describe the great famines
of the 20th century.
Define these terms:
Rationally evaluate pop and media claims about "healthy eating", vitamin supplementation,
newly-discovered vitamins,
"ideal weight", biotech food, and world hunger as they arise.
This unit should upset you.
Your patients have plenty of good questions about food and disease. There are more fads and
nonsense about "nutrition" than about any other health subject, and surprisingly, there are still
some
basic "unknowns". Any study involving nutrition is "news", and is immediately distorted in the
media, ultimately hurting the credibility of science.
I have watched "official" recommendations for a "healthy diet"
change from "the four basic food groups" (promoted by the dairy industry)
to today's "food guide pyramid" (definitions of
what a "serving" is vary by over 100% from agency to agency, and the
recommendation to limit animal protein is obviously politics rather than science).
We have far more food in the U.S. than we need, and enough micronutrients.
You will have to decide for yourself about the ethics
of using nutritional supplements (even as placebos) in the absence of controlled studies
demonstrating, or a clear theoretical model explaining, their benefits.
Many of your patients are taking supplements, known or unknown to you. ("Americans have the
most expensive urine in the world.") Your lecturer is undecided on the value of these.
Anecdotal accounts are sometimes impressive, but series evidence for
their value isn't impressive, and in any case, you shouldn't have to spend much money. See
Geriatrics 47: 56, 1992, more recently
JAMA 287: 3116 & 3127, 2002
found only theoretical reasons to supplement ($10/year is plenty despite
all the hype that this article generated).
A new placebo-controlled study finally found some benefit in healthy folks
and especially in diabetics (Ann. Int. Med. 138: 365, 2003).
A study that got hyped extensively suggested that a daily vitamin
supplement slows the progression of HIV infection -- but this was in Tanzania,
where true vitamin deficiencies are rampant (NEJM 351: 23, 2004).
The riddle is to find the particular patient whose
health will be improved by a particular nutritional supplement. Keep your eyes and ears open.
By contrast, nutritional deficiencies are presently (and have usually been) the
poor nations' greatest single
health problem, far overshadowing AIDS or any other individual disease.
As used today "undernutrition" and "malnutrition" seem to be synonyms, both
implying a diet insufficient to allow normal growth and normal health.
The extent of malnutrition in a population is determined primarily by
physical measurements.
Simply passing out cheap vitamin supplements to children in the poor
nations has an amazingly favorable impact on their health: Am. J. Clin. Nutr. 77:
891, 2003). However, the practice allows local "anti-Western"
militants to blame
these supplements for causing any childhood deaths (from any cause)
that may follow, and many of the locals will want to believe them (Br. Med. J. 324:
791, 2002; Am. J. Clin. Nutr. 75: 659, 2002).
During a
fifty-minute pathology lecture, around 1500 people die worldwide from malnutrition.
The Food and Agriculture Organization's 2004 pronouncement that
5 million children die every year (one every five seconds) from hunger
is probably about right, but it misses the bigger picture.
More subtle, early undernutrition leads to permanent underdevelopment of the
brain, and diminished intellectual ability (Nutrition 16: 1056, 2000).
Contrary to what you've been told by ideologues,
hunger is not a zero-sum game.
During the 1950's, the world had 3 billion people, and one person in two went to bed hungry.
Today, with 6 billion people, only one person in seven goes to bed hungry,
average calorie intake is up about 800/day,
and the developed nations are even more prosperous.
The twentieth
century ended with the fulfillment of Virchow's prophecy of 150 years ago.
Wherever real
democracy and free enterprise have
been allowed to develop, the old cycle of oppression, rampant
government corruption,
poverty, hunger, and overpopulation has been broken. Today this is called
the "demographic transition".
We hear a tremendous amount today about "the widening gap between
the rich and the poor", especially by anti-globalization activists and
"progressive" opinion-shapers.
But no one is actually claiming
that the world's poor today are worse off than in the past.
Obviously, we cannot cover nutrition (or any other subject) in as much detail as we might like.
This handout will supply most of what you'll need to begin the practice
of clinical medicine on your own, and you should know it at the
recall level.
You'll also find answers to questions you'll be asked at
parties.
* In 1985, the National Research Council (a food-industry pressure group) made political capital by
complaining in the media that the MD licensure exams had only 4% of
their items on "nutrition-related topics", hence that young physicians' education was woefully
misdirected, etc., etc. See Am. J. Clin. Nutr. 65: 568, 1997 (more politicking, but more reasonable).
PROTEIN-ENERGY MALNUTRITION ("marasmus-kwashiorkor")
Marasmus ("wasting") is the result of deficiency of total calories, while kwashiorkor is the result of
deficiency in protein. Classically, the victims are children.
Kwashiorkor:
This often follows the birth of a younger sibling, which displaces the baby from the breast.
Lack of protein causes low serum albumin (contributing to edema -- worst in the legs "because of
the atrophic fat"), and deficiency of other essential proteins such as those that carry copper and iron,
and enable the liver to burn and export fat (i.e., these children become anemic, and develop fatty liver,
though not cirrhosis).
For one thing, these kids have almost no peroxisomes in their livers, which probably contributes to
the fatty change (Am. J. Clin. Nut. 54: 674,1991).
Children are edematous, dull, and apathetic, and may not eat even if protein-rich food is offered.
They may have abundant subcutaneous fat, reflecting sufficient calories.
Look also for depigmentation on the skin and hair (one version is that "kwashiorkor", a West
African word, means "red child"). The "flag sign" on the hair reflecting a period of poor nutrition,
and dermatitis ("paint flakes", probably pellagra from tryptophan deficiency), especially on the
shins.
Eventually, a vicious cycle between protein deprivation and loss of the villi, microvilli, and
disaccharidases (notably lactase) of the gut. This cycle may take several days to break when
re-feeding begins. (Future gastroenterologists: You may see this in working up adult malabsorption,
too.)
{46292} kwashiorkor
Marasmus:
These patients exhibit emaciation (i.e., extreme loss of muscle and fat), "monkey faces", extreme
growth failure, and extreme hunger. They remain alert.
{46291} marasmus
Marasmus and kwashiorkor tend to overlap, and to be exacerbated by the concurrent infections to
which the children are already more vulnerable. There is no agreement on the exact nature or extent
of brain damage that remains after adequate nutrition is restored; it is clearly substantial (Lancet
338: 1, 1991; Sci. Am. 274(3): 38, 1996).
Marasmus-kwashiorkor in Tibetan children: NEJM 344: 341, 2001.
No, the Red Chinese cannot simply blame the altitude for stunting and sickness
in these kids.
Even nowadays, older folks in the hospital can get protein-calorie
malnutrition from hospital fare, and/or being kept "nothing by mouth" without
another source of nutrition (JAMA 281: 2013, 1999).
This is an ongoing scandal in many "developed" nations (Curr. Op. Clin. Nutr. 5:
31, 2002; J. Hum. Nutr. 15: 49, 2002.
Even the American Dietetic Association takes the position that doctors
will do well to liberalize their "diet prescriptions" for oldfolks
in long-care facilities (JADA 105: 1955, 2005), as a quality-of-life
consideration and a means to improve nutrition. ("Real food! Real food!")
Likewise, children in the US may present with classic
kwashiorkor unrelated to
illness, because their parents adopt fad diets, believe pop claims
that cow's milk is bad for children,
or are massively ignorant and/or disorganized (Arch. Derm. 137: 630, 2001).
Future clinicians: Both surgeons (Br. J. Surg. 75: 729, 1988) and internists (Mayo Clin. Proc. 64:
476, 1989) pay special attention to serum albumin in the very sick. While not a perfect measure of
"nutritional status" (the ultimate test is probably still the history and physical exam), it remains a
useful prognostic indicator. (Also remember that serum albumin drops in most liver disease and
during the acute phase reaction.) Marasmus and kwashiorkor are routinely ignored in the elderly: J.
Am. Ger. Soc. 39: 1089, 1991.
Refeeding syndrome, a disturbance in biochemical parameters
seen when food intake is restored in hunger strikers, anorectics,
hunger victims, or throat cancer patients, remains controversial.
Some investigators describe a hypophosphatemia (perhaps because
parenteral diets are low in phosphate); others
describe a range of abnormalities (J. Am. Diet. Assoc. 98: 795, 1998),
and still others
describe nothing of any clinical significance (perhaps because this
population was otherwise-healthy hunger strikers,
Nutrition 17: 100, 2001).
The "Zen Macrobiotic Diet" (no relationship to real Zen or any other school of
Buddhism) is a restrictive diet, popular for the past thirty years among
left-wingers. The claim is that it prevents and cures cancer, though I have seen
nothing to make me believe this is true. What we do know is that it can and
does cause protein, cobalamin, vitamin D, calcium, and riboflavin deficiency in kids. The
result is problems with growth and mental development (Am. J. Clin. Nutr. 59(5S): 1187S, 1994).
The macrobiotic diet gurus of the 1990s were a husband-and-wife
team, Michio and Aveline Kushi; Aveline
died of cancer of the cervix in 2001.
* Dietary faddism is ever-changing.
A couple in Israel almost kills their baby by an almond-based fad diet: Clin. Nutr. 20: 259, 2001.
* The triumph of the body's wisdom:
the poorest refugees in Zaire's camps sold their donated
corn-and-grease for better-balanced diets (Lancet 351: 128,
1998), even though they got fewer calories.
Strachan's syndrome / neuropathy of malnutrition / Cuban epidemic neuropathy:
A distressing syndrome of peripheral neuropathy (mostly sensory, with pain and loss of position
sense) and/or optic nerve atrophy (blind spots, blindness). No one knows exactly
which nutritional
deficiency is to blame, but it's typically seen in folks accustomed to a good diet who suddenly go on
semi-starvation regimens.
First described in U.S. POW's in the tropics in WWII ("Strachan's"), it reappeared most famously in
Castro's Cuba in 1991, when the collapse of the Soviet Union removed Cuba's principal source of
food and money.
Cubans were more likely to be affected if they also smoked heavily (love those Havana cigars!)
and/or ate cassava (which contains cyanide). Since tobacco smoke also contains cyanide,
investigators got the idea that deficiency in methionine or folate or something prevented
detoxification of -CN moieties.
The grisly epidemic ended in June 1993, when the Cuban government started passing out vitamin
supplements. Read about this fiasco in NEJM 334: 1063, 1996; J. Neurol. 242: 629, 1995.
Thanks for once, Fidel.
Usually politicians do not act to remedy the diseases they cause.
* According to the Cuban pathologists, a
large majority of those with symptoms reportedly also had Coxsackie A9
or one of its kindred on board, whatever that means (Arch.
Path. Lab. Med. 121: 825, 1997.)
Strachen's (?) in a dietary eccentric (he can't have been a real "vegan"
since the pattern of deficiencies doesn't fit): NEJM 342: 897, 2000.
VITAMINS: catalysts that the body cannot synthesize by itself.
Today, the classic single-vitamin deficiencies (except vitamin A deficiency) are hard to find
anywhere. Mixed deficiencies are also rare in the U.S.
They are common in the poorer nations but are generally mixed with
other forms of malnutrition.
The fat-soluble vitamins are of course vitamins A, D, E & K. These are storable, but do not get
absorbed through the gut in biliary insufficiency and other forms of fat malabsorption (ask about
mineral oil use).
The water-soluble vitamins (B & C, and folic acid) are available in most any varied diet, though we
supposedly do not store them well. (This is obviously not true of all these vitamins; it
takes at least months to
develop vitamin B12 deficiency on a deficient diet alone.)
You will frequently hear the claim that people on the U.S. diet have "subclinical vitamin
deficiencies", for which they should take supplements. The RDA's for most vitamins (except
probably vitamin D) are set very high to allow for individual variations in needs, and benefits of
treating hypothetical "subclinical deficiencies" has been very hard to demonstrate (Lancet 2: 313,
1989; Lancet 335: 744, 1990.)
The one obvious exception is folic acid, especially in pregnant women and the mentally ill; for the
special problems concerned with iron supplementation, see below. * The one contraindication to routine iron and folic
acid supplementation may be endemic malaria; you are also nourishing
the parasites. See Lancet 367: 133, 2006.
The U.S. mandated that folic acid be added to all "enriched" foods beginning
Jan. 1, 1998.
The decision to supplement food with folic acid is intended to
prevent neural tube defects.
Some people
need quite a bit more folic acid than
others (partial enzyme deficiency: Lancet 346: 1070, 1995).
You can actually get folks (even the poor) to eat a lot more fruits
and vegetables simply by talking with them for a few minutes about
why it's a good idea (Br. Med. J. 326: 855, 2003).
But since many Americans won't eat a reasonable diet, it's easy
to think (but hard to prove experimentally) that some folks might benefit
from routine supplementation, as folk-wisdom has maintained for decades.
And because a person's annual supply of a reasonably-priced multi-vitamin-and-mineral
tablets costs only about $10, this seems reasonable (JAMA 287: 3116 & 3127, 2002).
* True-believers in "subclinical deficiencies" can read Lancet 337: 587, 1991, and Nature 350: 2 &
15, 1991 for claims of improved grade school performance. Before accepting this much-hyped
study uncritically, note that the principal investigator is a California criminologist who was also
promoting a nutritional supplement to make children smarter.
A widely-publicized article presenting evidence that vitamin supplements
slow the cognative loss caused by aging turned out to be a complete hoax
(Br. Med. J. 328: 67, 2004).
Since these are the only two studies supposedly showing a measurable benefit
for routine supplementation, and both are evidently by crooks,
I'm willing to draw an obvious conclusion. I could find nothing
more since this to support the "subclinical deficiencies" business.
Pharmacologic activities of vitamins (niacin for schizophrenia, pyridoxine for emotional illness
and premenstrual syndrome Br. Med. J. 318: 1375, 1999,
pyridoxine and folic acid to lower homocysteine and thus prevent atherosclerosis
(betaine is established for this purpose),
vitamin E for arthritis, coenzyme Q for any cardiomyopathy,
vitamin C for everything) are still under study. Anecdotal
evidence is interesting, and obviously no large pharmaceutical house will fund these studies.... But
as always, be skeptical about grandiose claims.
Most of the recent "big studies" on antioxidants to prevent cancer have shown
no or negative effect (Lancet 364: 1193, 2004), and a meta-analysis
actually showed some increased overall mortality in the groups taking the supplements.
Laetrile (amygdalin, vitamin B17) and the mythical substance "pangamic acid" (a variously-numbered "B vitamin";
the pills were glycine, sugar, or whatever) are make-believe vitamins. No
U.S. law forbids selling your belly-button lint and calling it "vitamin Z".
Vitamin A, made by your body from carotene in yellow vegetables, etc., exists as retinol, retinal,
retinoic acid, etc. Your body stores it in the liver and shuttles it around on
retinol-binding protein (* formerly
called "prealbumin" or "transthyretin").
Obvious deficiencies (and certainly some not-so-obvious deficiencies) are common in the poor
nations of the Far East and in northern Africa. The usual problem is deficient diet (Am. J. Clin.
Nutr. 59: 401, 1994), and providing supplements is cheap and easy, and saves lives, where it is
politically feasible.... (Lancet 1: 824, 1989; NEJM 323: 929, 1990; Lancet 338: 67, 1991; JAMA
269: 898, 1993).
In Nepal, simply supplementing the diet cut maternal mortality spectacularly
(Br. Med. J. 318: 570, 1999). Integrating
vitamin A supplements into immunization campaigns would save
one life for every $72 spent (Am. J. Pub. Health 90: 1526, 2000); it
is now underway.
"Miracle rice" is rich in vitamin A, and has been made available
in the hopes of preventing
preventing blindness, brain damage, and millions of deaths in the poor
nations. How it was done: Science 287: 303, 2000.
It also is enriched with iron, and has less of the phytates that
diminish iron absorption (Nutr. Rev. 61: S-101, 2003).
The scientists and biotechnology corporations actually donated this
to the world as a gift and gesture of goodwill.
Its use in
the poor nations is now widespeard and much appreciated.
See Nature Biotech. 21: 971, 2003
*
Thanks almost entirely to a campaign by Greenpeace,
attempts by the scientific community to provide
enhanced rice where it was most needed
was stalled for years (Sci. Am. 282(4): 42, 2000).
I have examined complaints by these people and other
"environmentalists" ("Frankenstein food!"
"Nazi science!" "Genetic contamination!").
When the supposedly-evil biotechnology corporations donated the rice
to the world, and Greenpeace got some deservedly bad publicity
for their activities, they switched their rhetoric to the
claim that the vitamin A was not bioavailable. It's clear this isn't so
(Am. J. Clin. Nutr. 81: 461, 2005), and that eating the rice
helps end night blindness, though of course liver and carrots are better.
I believe that any reasonable
person will conclude that, in this particular instance, they are
crying "Fire!" where
there clearly is none -- at the expense of the health and lives of
the world's poor, for whom the Left
has always claimed to speak. What's more, I believe the people who
actually wrote the anti-rice stuff (though perhaps not the leaders of Greenpeace)
know perfectly well that
they are deceiving the public.
What settles it for me is that the anti-biotech people don't even
take their campaign to the farmers and the poor folks
who they are supposedly protecting,
even when they are their neighbors (Nat. Biotech. 21: 9, 971).
The fact that the anti-rice stuff is
written for rich city-dwellers tells me it's all just a way for the left-wing
activists to make money and play politics.
This might be a good topic for an in-lab presentation.
In the U.S., the best-known cause is longstanding malabsorption (notably cystic
fibrosis). However, I believe that subclinical deficiency sufficient to
cause harm is widespread, especially
in the underclass (see J. Ped. 145: 99, 2004). Vegans who do not know exactly what they
are doing are at serious risk: Clin. Ped. 43: 107, 2004.
Vitamin A is responsible for maintaining the differentiation of certain special kinds of epithelium
(including many ducts), and in the deficiency state, epithelial surfaces of all kinds tend to undergo
squamous metaplasia and hyper-keratinize.
The best known symptoms of deficiency are xerophthalmia (from loss of differentiation of the mucus
cells of the cornea), Bitot's spots (masses of desquamated keratin on the cornea or conjunctiva; Am. J. Ophthal. 118:
792, 1994), keratomalacia (too much keratin on the cornea, which gets wet, macerated, and
infected), and ultimately blindness. At least 1.2 million people are permanently blinded each year
from vitamin A deficiency.
Other problems include kidney stones (from desquamation of transitional epithelium in the renal
pelvis), acne ("papular hyperkeratosis", from too much keratin plugging the follicles), lung
infections (no cilia), and poorly-understood immunodeficiency.
Vitamin A is also the precursor of visual pigments, on the other side of the eyeball, and the first
complaint in vitamin A deficiency is diminished vision in the dark.
Vitamin A and its receptor are transported to the nucleus, where they have something to do with
gene expression. Stay tuned here; this may have to do with its reputed anti-carcinoma properties.
(For example, some vitamin A compounds induce differentiation of neuroblastoma in tissue culture.)
Excess vitamin A ingestion (>100 x the RDA, i.e., accidental ingestion, faddism, polar-bear liver
eaters) produces increased intracranial pressure ("pseudotumor cerebri") with headache and nausea-vomiting, a special kind of
fatty liver (* stored in the "Ito cells"), and desquamation of the skin (as seen in those
taking Accutane, but worse). Remember that retinoids, but not carotenoids, are teratogens. More
than 10,000 U/day is bad for your unborn child: NEJM 333: 1369 & 1414, 1995; and that "Accutane"
may cause depression in teens at a time in life when nobody needs extra problems.
One clue to vitamin A overdose may be the same skin discoloration as in those of us who enjoy
carrots.
Thankfully,
you cannot metabolize carotene fast enough to get hypervitaminosis A. I happen to like to
eat carrots.
There's still vitamin A deficiency around, even in the rich nations (i.e., folks with gut problems: Br.
Med. J. 310: 1034, 1995). Vitamin A deficiency was common in the US
before the 20th century.
In the "developing world", the impact of vitamin A deficiency is devastating.
Indonesia: Am. J. Clin. Nutr. 68: 1068, 1998,
Am. J. Clin. Nutr. 71: 507, 2000. Bangladesh: Br. Med. J. 316:
422, 1998.
Vitamin D:
Vitamin D precursor is available in the diet, or from the action of ultraviolet light on
7-dehydrocholesterol in the skin. After 25-hydroxylation in the liver, it is completely activated by
1-hydroxylation in the kidney. You know its effects on calcium and phosphorus metabolism.
Review: Am. J. Kid. Dis. 32(2 S 2): S-13, 1998.
Vitamin D deficiency, once considered
rare in the U.S. except as part of the "tea and toast" syndrome among the
elderly, is actually common if you (sensibly) consider
people with serum PTH higher-than-you'd-expect to be deficient.
(The RDA of 200 IU/day may be low for older people in the winter: NEJM 321: 1777,
1989). Vitamin D deficiency
is a major problem worldwide, especially among the dark-skinned or at very high
latitudes.
All the sun exposure that's requird for a light-skinned person
is 5-10 minutes, 2-3x/week, arms-and-legs or arms-hands-face
(Am. J. Clin. Nutr. 80(S6): 1678-S, 2004.
* "The sunshine and vitamin D controversy" promises to engage the attention
of the public for the foreseeable future.
Since it involves race, vegetarianism, cancer fears,
people nagging their family members
that "sunshine is good" or "sunshine is bad", and even religious practices,
it is unpleasant.
The facts are: (1) there is a LOT of vitamin D deficiency, it is
serious, and it is almost
entirely preventable; (2) your needs
can be met easily by supplementation or diet without requiring any sun
exposure; (3) vegetarians who don't know
exactly what they are doing are at
greatly increased risk; (4) dark-skinned people need more sun exposure
to make their vitamin D than do light-skinned people; (5) sun exposure
invites photoaging and cancer, especially in doses much greater than a
non-supplementing vegan needs for vitamin D production. This is too much
to ask the public to sort out -- be ready to help.
There was lots of rickets in the US until recently, especially among
poor black children. OJ Simpson was supposedly affected.
It has resurfaced among black children in the US; "cultural practices"
causing rickets include veiling little girls (Moslem subsect)
and "natural diets without
additives" (Adventist subsect; Pediatrics 64: 871, 1979).
Worldwide, there is a resurgence in rickets (Lancet 362: 139, 2003);
at least part of the cause is the current fad for exclusive breast-feeding
of babies for long periods (especially when the mother herself is vitamin D deficient),
and the trend for less sun exposure (fear of cancer, Islamic veiling of women).
Breast-fed (i.e., no vitamin D supplementation), dark-skinned babies at high latitudes are at some
risk in the U.S., but rickets is not much in evidence (Am. J. Clin. Nut. 59(S2): 484-S, 1994.)
In Nigeria, supplementing calcium, with or without vitamin D,
actually works better than vitamin D alone (NEJM 341: 563, 1999). In other words,
a lot of the problem is calcium deficiency instead of vitamin D deficiency.
In renal failure with loss of the proximal tubular epithelium, there is inability to fully activate
vitamin D, and some of the bony problems that used to plague dialysis patients resulted form this
defect.
Unusual causes of vitamin D deficiency include malabsorption, nephrotic syndrome (loss of
vitamin D and its binding protein in the urine), antacid buffs, and some odd inborn errors of
metabolism (vitamin D resistant rickets; type I lacks 1-hydroxylase in the kidney, type II probably
lacks vitamin D receptors).
Actually, patients with persistent, nonspecific musculoskeletal pain
very often have vitamin D deficiency as the underlying cause. This is now
"painfully" obvious (Mayo Clin. Proc. 78: 1463, 2003), and is not just
confined to the groups that are "supposed" to be vitamin D deficient.
The bony lesions of vitamin D deficiency are called "rickets" in growing children, and
"osteomalacia" in grown-ups.
The essential lesion in both rickets and osteomalacia is failure of osteoid (bone matrix) to
mineralize.
In rickets, the epiphyseal cartilage does not even calcify. Instead, it overgrows (knobs, including the
"rachitic rosary" and other characteristic x-ray changes).
"Big Robbins" lists the terms for the bony abnormalities of rickets, including "craniotabes" (inward
buckling of skull bones), "frontal bossing" and "square head", the "rachitic rosary" (knobs on the
costochondral junctions), "pigeon breast" (anterior protrusion of the sternum, pulled forward by the
respiratory muscles), "Harrison's groove" form inward pull of the diaphragm, "lumbar lordosis" and
"bow legs", and pelvic deformities that caused "death during childbirth" in so many Northern
European city women in bygone days.
In osteomalacia, the non-calcified bone looks pale on x-ray, and tends to break. (* Future
radiologists: Little bone fractures are called "Looser's zones"). Yes, a vegetarian eating style (i.e.,
little meat or milk) does cause epidemic osteomalacia: QJM 83(302): 439, 1992.
Low bone mass in vegetarians, where it matters: Arch. Int. Med. 165:
684, 2005.
More about this when we talk about bones.
* Vitamin D deficiency, especially in people with mutated vitamin D receptors too,
is a risk factor for severe tuberculosis: Lancet 355: 618, 2000.
This is getting interesting.
Depending on your vitamin D receptor subtype, your need for the vitamin
may be greater. This is reflected in one's resistance to TB,
which requires adequate vitamin D effect (need it for
intracellular killing of the TB bug, Lancet 355: 588, 2000).
{12027} rickets, x-ray with bent bones
Excess vitamin D ingestion (i.e., taking too much) is in the differential diagnosis of hypercalcemia
and kidney stone formation, but is seldom encountered. * There is talk of this promoting
atherosclerosis ("abnormal calcification", a misconception), etc., I doubt this.
Vitamin E (review Lancet 345: 179, 1995): Ubiquitous in the diet. Today's deficiency victims have
malabsorption (it was also seen in the early days of total parenteral nutrition), and suffer
pigmentation and dysfunction of the gut (the presence of ceroid is a marker)
and sensory
pathways of the spinal cord.
Evidence of the usefulness of vitamin E in treating disease, staving off old age, or avoiding
mutagenesis from cosmic rays remains anecdotal. It is now used to cure the hemolytic anemia of
preemies, and perhaps also prevents preemie eye disease (J. Ped. 144: 801 & 827, 1989).
Vitamin E deficiency produces a considerable excess
of lipofuscin in experimental animals.
Cystic fibrosis babies are prone to vitamin E deficiency (why?) and get the same kind of hemolytic
anemia (Clin. Ped. 33: 2, 1994).
For preventing heart attack and stroke in people
at high risk, vitamin E supplementation was a flop: NEJM 342:
154, 2000.
* Children who lack of tocopherol transfer protein need huge amounts of vitamin E
or they develop ataxia (J. Ped. 134:
240, 1999; Neurology 55: 1584, 2000).
Vitamin K
This is the cofactor for the synthesis of gamma-carboxy glutamic acid, which is required for the
calcium-binding clotting factors II, VII, IX, and X, plus protein C, S, and * Z. Although our
intestinal flora make a little vitamin K for us, it is inadequate. Fortunately, vitamin K is hard to
avoid in the diet, we store several weeks' supply, and deficiency is seen mostly in newborns and in
those with lipid malabsorption.
Milk is relatively poor in vitamin K, and babies who do not receive prophylactic vitamin K and who
are fed mostly milk occasional run into problems with hemorrhage (J. Ped. 114: 602, 1989; Ped.
Emer. Care. 8: 143, 1992). An oral supplement that mothers would give during the first
few months of life is under consideration (Arch. Dis. Child. 82: F64, 2000).
Deficiency in vitamin K due to wiping out the bacterial flora with
antibiotics is much-discussed; it is not an obvious clinical problem.
Functional vitamin K deficiencies are seen in those on coumarin (the vitamin K antagonist
anticoagulant), and in severe liver disease. * Trivia: PIVKA is "protein induced in vitamin K's
absence", i.e., non-gamma-carboxylated versions of clotting factors. Vitamin K is given to preemies, newborns, and people in liver failure in the hopes of preventing
serious hemorrhages. Right now, the injected form seems preferable to oral dosing (CMAJ 140:
496, 1989). Some people now advocate it for all babies: Br. Med. J. 303: 1083, 1991.
{15932} infant purpura; vitamin K would have prevented this
Vitamin B1 (thiamine)
This vitamin (* as pyrophosphate) is the co-factor for burning α-keto-acids, and for
transketolase (the pentose phosphate shunt enzyme). Somehow it also maintains nerves. The
molecular biology of clinical thiamine deficiency remains elusive.
Thiamine deficiency was seen classically in people subsisting on polished rice, and today in
alcoholics, cancer victims who do not eat, women with extreme vomiting of pregnancy, and in
children and adults who have been starved.
Beware sudden carbohydrate loading of these people
prior to administering thiamine, for fear of triggering acute deficiency.
Thiamine deficiency produces:
Note the similarities of wet and dry beriberi to "alcoholic cardiomyopathy" and "alcoholic
neuropathy" respectively. While alcoholics are often thiamine-depleted, we now know this is not the
whole story.
Vitamin B2 (riboflavin)
This is the precursor for the cofactor FAD, from biochemistry. "Big Robbins" devotes excessive
space to this extremely rare problem, which (if it exists at all)
supposedly only affects alcoholics and the extremely malnourished.
Remember that "cheilosis" ("cheilitis", cracking around the angles of the mouth -- a much more
common cause is edentulousness), seborrheic-type dermatitis on the nose, cheeks, and hands ("glove
dermatitis"), and purple tongue. Why these specific signs occur (if any of this
really happens) is totally mysterious.
Vitamin B3 (niacin, nicotinic acid)
This is the precursor for the cofactor NAD, also from biochemistry. If there's not enough in your
diet, you can make it from spare tryptophan (* excess leucine, as in
diets with protein coming mostly from millet, blocks this).
It is ubiquitous in nature, but is sometimes unavailable. Niacin in maize ("corn") is poorly
absorbed, maize is low in tryptophan anyway, and pellagra (* Italian for "dry skin") used to be
endemic in our southern "corn belt" (the history, and how the riddle was solved:
South. Med. J. 93: 272, 2000).
Today if you see pellagra, it is probably in an alcoholic
(Mayo Clin. Proc. 76: 315, 2001) or a food faddist. The largest outbreak since
World War II involved thousands of refugees in Malawi (MMWR 40: 269, 1991).
* Rare causes include carcinoid syndrome, in which tryptophan is pre-empted to make serotonin, and
Hartnup disease, in which patients cannot absorb tryptophan from the gut.
Niacin deficiency ("pellagra") produces the "three D's":
Niacin remains a cheap and good way to lower LDL cholesterol.
The use of niacin for this effect is still widespread.
Vitamin B6 (pyridoxine)
This is the cofactor that is responsible for shuttling amino groups and amino acids around in
biochemistry. Deficiencies occur in alcoholics (* alcohol moves the factor off of its proteins and
encourages its degradation), and pregnant and lactating women. Functional deficiencies occur in
patients taking isoniazid, penicillamine, or * cycloserine.
Deficiencies in humans are probably rare and almost all subclinical, with minor neurologic and
mouth problems.
Well, maybe. Pyridoxine as prophylaxis for atherosclerosis, like
folic acid; both lower homocysteine levels: JAMA 279: 359, 1998. Definitely stay tuned.
Pyridoxine is also useful in treating several inborn errors of metabolism in which there is defective
binding of the vitamin to its site of action, or something similar. A pyridoxine-responsive
sideroblastic anemia
may result from overgrowth of a mutant clone; one known gene that is knocked
out is delta-amino levulinic acid synthetase (Am. J. Hem. 62: 112, 1999.)
Folic acid (* Vitamin P; update Br. Med. J. 328: 211, 2004)
The familiar cofactor that helps shuttle methyl groups through the biochemistry pathways. Our best
sources are uncooked vegetables and fruits. The clinical syndrome is a megaloblastic anemia
that you will
study later.
Deficiency is common in the U.S., and folic acid deficiency is very common in alcoholics, in
pregnant women (who have a tremendously increased need), people with malabsorption, and in
people taking phenytoin, and probably among the mentally ill (many of whom recover faster when it
is administered; Lancet 336: 392, 1990).
Although meat-eating is uncommon in India, and many people are vegetarians,
folic acid deficiency is rampant (and for some reason, so is B6 deficiency):
Asia Pacific J. Clin. Nutr. 10: 194, 2001; from India's National Institute of Nutrition.
* No one knows the real cause of tropical sprue, but folate therapy helps the patient heal.
For the neural tube defect story, see above. Women who have had more than one kid with a neural
tube defect may have a problem handling folic acid (Br. J. Ob. Gyn. 101: 197, 1994), and/or the
unborn children have a gene that causes them to require extra folic acid.
* In 2000, there was a silly flap about the vitamin
causing miscarriage; it doesn't (Lancet 358: 796, 2001).
Canada has apparently had the best experience, with a 78% reduction
in neural tube defects since supplementation was introduced: Br. Med. J. 324:
760, 2004.
Even a little deficiency in folic acid increases your serum homocystine, which is an arterial-wall
poison. We'll cover the low-folate / atherosclerosis connection when we talk about "Vessels". It's
BIG news.
Vitamin B12 (cobalamin, cyanocobalamin)
The other cofactor for handling methyl groups (i.e., making thymine/DNA and methionine).
Deficiency is seen in vegans (those who take no food of animal origin
because of moral convictions) who do not
supplement (it's still rampant: Am. J. Clin. Nutr. 78: 131, 2003; enough to affect
hematology parameters Eur. J. Haem. 69: 275, 2002; Adventist clergy Am. J. Clin. Nutr. 70(3S): 576S, 1999), in those with problems with
intrinsic factor ("classic pernicious anemia", etc.), fish tapeworm infestation, blind loop syndrome,
and inflammation of the terminal ileum (typically Crohn's disease).
Frankly, as a physician, the whole business worries me very much.
I hope that every
high-school idealist who decides to "become a vegan",
especially those who will get pregnant and/or raise "vegan" babies,
is presently obtaining the supplementation necessary for good health.
I very much doubt this is happening. I urge my fellow-physicians,
especially those in primary care, to talk frankly with young people about
this business. Even the vegan gurus, while promoting their diet for children,
emphasize the elaborate counselling and fortification of "special vegan foods"
that are required to keep kids from getting frightfully sick (J. Am. Diet. Assoc. 101:
661, 2001).
It's now obvious that even common amateur vegetarians can and do become
B12 deficient (review Am. C. Lin. Nutr. 78: 3, 2003).
In Germany, 60% have biochemically-obvious
B12 deficiency (elevated homocysteine / methylmalonic acid / holotranscobalamin II levels)
(Clin. Chim. Acta 326: 47, 2002).
* The traditional teaching is that B12 deficiency
is unlikely when there is even a little intake of food of animal origin.
I'm not so sure. Some newer studies from the Third World show low levels
in children whose anemias are unresponsive to iron (Am. J. Clin. Nutr. 71: 1485, 2000).
You will study the megaloblastic anemia and the neuropsychiatric syndromes (Alzheimer-like
dementia, "subacute
combined degeneration of the spinal cord", etc.) later in the course. The latter is probably missed
frequently (NEJM 319: 1733, 1988; neurobiology of cobalamin deficiency: Medicine 70: 229,
1991).
* Many patients demand cobalamin injections for a variety of illness without any clear indication. I
have long considered this lousy medicine; recently somebody's noticed that 12% of older folks have
chemical (high methylmalonic and/or homocysteine levels) and/or hematologic (low hematocrit,
high MCV) levels, which indicate either B12 and/or folate deficiency; tough to sort these out; but
the group blamed cobalamin; I thought (and still think) the problem is really deficient folic acid.
Ultimately, the decision about giving hokey B12 shots is yours (JAMA 261: 1920, 1989).
Easy to overlook: Mothers who are breast-feeding while they are
(perhaps subclinically) B12 deficient place their children at grave
risk for permanent brain damage (Arch. Dis. Child. 78:
398, 1998). With young mothers going in for radical vegetarianism
(Muscle and Nerve 22: 252, 1999), there will be plenty
more of this in the future. The literature has been silent on
this situation for decades, probably for reasons of
political correctness
("You're against breast feeding! You're against
vegetarianism!")
Biotin: Remember that "avidin" in raw eggs is very effective at blocking absorption of biotin
(* "Rocky Balboa" take note).
Pyrroloquinoline quinone was found to be an essential
nutrient in the early 2000's; we await a deficiency syndrome in humans.
Humans, a few other primates, guinea pigs, and fruit-eating bats cannot synthesize this redox
cofactor, which is involved in developing and maintaining collagen, synthesizing chondroitin sulfate,
as well as a variety of other important things.
* It's supposed to be a weak antihistamine, perhaps accounting for the mild effect on colds and
allergies. Ignore R&F's oxymoron "evolutionary quirk" -- biology makes sense. We tend to lose (or
weren't given) pathways we don't need, and humans seek a varied diet.
The deficiency syndrome is "scurvy", which occurs only in people who eat very poorly for several
weeks. (The original "Zen Macrobiotic Diet" caused a cluster of deaths from
scurvy.) In the poor nations, scurvy occurs in children whose mothers feed them with un-supplemented formula.
There is much talk about stress (especially the stress of surgery, as well as wound healing) as
producing an added requirement for vitamin C. Decide for yourself.
Scurvy is a distinctive clinical syndrome related, at least in part, to problems with osteoid synthesis
and collagen support of the blood vessels.
In children, the osteoblasts lay down scanty, poor-quality osteoid. The end result is radiographs and
deformities similar to rickets.
In both children and adults, the capillaries weaken. Patients bruise easily, and bleed spontaneously.
Check the gums, and look for petechiae around the hair follicles. The body hairs often become
curled like corkscrews; hemorrhages around these corkscrew hairs give
you the diagnosis.
Eventually, hemorrhages beneath the periosteum develop, making this the most painful of the
deficiency diseases.
Of course, wounds heal poorly, and old ones reopen.
A secondary functional folic acid deficiency develops, because vitamin C is responsible for
maintaining folate in its reduced state.
Tales of scurvy on the high seas are horrible. Vitamin C availability was the
limiting factor on global exploration until physicians persuaded admirals to provide lime juice for
sailors (hence the British term "limey" for sailor). James Lind solved the problem
in 1754 ("A Treatise on the Scurvy" -- he even used controls), but the British
government was so penny-wise-and-pound-foolish that they declared
the cask of lime juice "too expensive", and only made it mandatory 50 years later.
* A US serviceman gives himself scurvy by deciding to live on
nothing but skinless chicken, cola drinks, and candy bars (Orthopedics 25:
689, 2002).
{05940} scurvy, mouth
"Mega-dose vitamin C" (a gram or more daily) is being used by many of your patients to "prevent
cancer", "cure colds", etc., etc.
In the absence of renal insufficiency, fatalities occur at 20-40 gm/day, from calcium oxalate
deposition in the heart.
It also gives false-negative tests for glucose and occult blood in urine and stool, and promotes
over-absorption of iron by the gut (well maybe, see below). These are most likely to cause problems
if the user's physician is not aware of that the patient is taking the substance.
* The popular "rose hip vitamin C" is synthetic vitamin C with a tiny amount of rose pulp added,
sold at inflated prices.
* Some volunteers were hospitalized at the NIH and rendered vitamin C-poor by diet (heroes' award),
then loaded up.
Pee-out of the unaltered vitamin began at 100 mg/day, and everything above 400 mg/day simply
went through the people; at 1000 mg/day and above, the serum oxalate and urate levels began to
climb. Read Proc. Nat. Acad. Sci. 93: 3704, 1996.
There are some interesting new findings about vitamin C's varied biologic activities, but nothing
definitive. Stay tuned here, but don't be disappointed if miracles are not forthcoming (Ann. Int.
Med. 114: 909, 1991).
Scurvy in Afghanistan under the Taliban: Lancet 359: 1044, 2002.
MINERALS
Iron
This element is absorbed by the duodenum, which regulates the total body load (2-6 gm). Iron
deficiency is the most common nutritional deficiency almost everywhere.
Amateur vegetarians can expect to have their iron status compromised
unless they know exactly what they are doing. It is quite possible
to follow a vegetarian diet without becoming iron-deficient (Am. J. Clin. Nutr.
59(5-S): 1233-S, 1994), but nowadays it's obvious that people
are jeopardizing their health by making themselves iron-deficient (Eur. J. Hem. 69:
275, 2002 -- reminds us that the microcytosis of iron deficiency and the
macrocytosis of B12 deficiency will mask each other)
Iron deficiency is rampant among poor children in the Third World, and a history of iron deficiency
(perhaps evidence of other things lacking in the diet) is a marker for stunted intellectual
development later in life (NEJM 325: 687, 1991). Simply distributing iron cooking
skillets helps children grow and be healthy: Lancet 353: 712, 1999.
Iron deficiency among inner-city British babies fed unsupplemented cow's
milk is probably a major cause of developmental slowing:
Br. Med. J. 318: 693, 1999.
One Georgia teen in three is iron-deficient (South. Med. J. 87: 1132, 1994).
* Curiously, iron deficiency itself seems to promote pica, including
soil-eating, which remits after successful therapy with iron.
Possibly there is an instinct for iron-deficient folks
to eat soil, which might be rich
in iron (as well as lead, mercury, elemental phosphorus,
and other things that are bad for us). This in turn may have become
part of the cultures of poor areas; for example, in areas of the US
southeast where there has historically been a lot of hookworm,
one can still buy packages of earth (with warning labels, "do not
eat") at convenience stores.
Classically, iron deficiency is a microcytic, hypochromic anemia. The actual anemia reflects a late
stage, and we currently think that some metabolic derangements precede this, since iron is involved
in many enzymes.
Texts talk about cheilitis, esophageal webs, etc., in iron deficiency, and about cravings to eat clay,
chew ice, eat starch, etc. (Perhaps the pica is really the cause instead.) The link with esophageal
webs ("Plummer-Vinson syndrome") is now considered very dubious.
One can get a good measure of body iron stores by checking the serum ferritin. Another popular
screening test is measuring serum iron (will be low)
and serum total iron-binding capacity (mostly transferrin, will be high), and
calculating saturation (Fe/TIBC). More about this later.
Yet another worthwhile technique, especially for screening kids, is to look at zinc protoporphyrin
levels in the blood; these are high in the iron-deficient (Clin. Ped. 33: 473, 1994).
Iron deficiency is easily treated. (Remember that we absorb "heme" iron much better than "iron
pills".) However, it is malpractice to merely treat iron deficiency without seeking a cause of blood
loss, especially in someone who is not menstruating.
There's an old tale about vitamin C enhancing iron absorption through the gut; lately
Uncle Sam tested this, and the effect, if any, is minimal: Am. J. Clin. Nutr. 59: 1381, 1994.
* "Special molasses" touted at the health-food store as "an excellent natural source of iron and
copper" acquires both from the machinery in which the sugar is processed.
Zinc
Zinc is not super-abundant in the U.S. diet. Deficiency has occurred, mostly in patients with
malabsorption (disease, inborn error, patients in the early days of total parenteral nutrition). The
most distinctive feature is "acrodermatitis enteropathica", a rash that is also seen in other illnesses.
You can decide for yourself about the usefulness of zinc supplementation in wound healing (i.e., in
wartime, after surgery).
* Zinc deficiency also produces night-blindness, perhaps potentiating any concurrent
vitamin A deficiency (Am. J. Clin. Nutr. 73: 1045, 2001).
Endemic zinc deficiency with dwarfism
has occurred among clay-eaters in certain near-Eastern populations
(Nutrition 17: 67, 2001). Zinc is also in short supply in breast milk: Lancet 340: 683, 1992.
Copper deficiency
This can occur in preemies and in starvation, and in patients on total parenteral
nutrition. Since zinc competes with copper for absorption, people taking the
new over-the-counter zinc pills are coming in with copper deficiency (J. Ped. 136: 688, 2000;
also Am. J. Gastroent. 95: 2975, 2000 for the guy who likes the taste of
those new zinc pennies). * There is a curious syndrome
("myelodysplasia" and "subacute combined
degeneration of the cord with normal B12 levels")
in adults with near-zero copper levels and high zinc levels
with normal diet (Mayo Clin. Proc. 80: 943, 2005); your lecturer
predicts they will be found to have a copper-zinc transporter
with higher affinity for zinc. Because copper is required:
* In the 1990's, the Environmental Protection Agency and World Health Organization
came out with guideline values for "too much copper in the drinking water."
Although there have been outbreaks of copper toxicity at very high levels,
the "official" stuff was immediately recognized as junk science (Am. J. Clin. Nutr. 67(5S): 1098S, 1998.
Selenium deficiency:
Fortunately rare in the democracies, this was the basic cause of China's endemic "Keshan disease", a heart failure syndrome
of young people (Biomed. Env. Sci. 4: 359, 1991) that
rendered people much more susceptible to coxsackieviruses
(J. Clin. Microb. 38: 3538, 2000; J. Inf. Dis. 182 S-1: S93, 2000).
The histopathology was miliary patches of
hyaline necrosis through the heart muscle.
Selenium deficiency resurfaced in Africa as a cause of post-partum cardiomyopathy (Int. J. Card. 36: 57, 1992).
Watch for more of the same.
The myopathy, better known in animals, is "white muscle disease".
Selenium deficiency is now sometimes seen in long-term hyperalimentation patients (so is chromium deficiency; NEJM
322: 829, 1990)
More recently (and confusingly), selenium deficiency and fulvic acid (from rotting junk) in the
drinking water have been found to cause epidemic Kashin-Beck osteoarthritis in central Asia.
Review: NEJM 339: 1112, 1998.
* Selenium poisoning in China in the 1960's: Am. J. Clin. Nutr. 37:
872, 1983.
We'll talk more about this under "thyroid disease".
Iodination of salt has virtually eliminated iodine-deficiency as a cause in the U.S., though not, of
course, in all the poor nations.
To my knowledge, there isn't even a crackpot anti-iodized salt movement.
For now, remember that 5.7 million children are brain-damaged ("cretins") yearly from lack of
iodine (Med. J. Aust. 154: 227, 1991); if it were not for politics, this problem could be entirely
eliminated (NEJM 326: 236 & 267, 1992).
Epidemiologists look for a large thyroid gland, low iodine excretion
after loading, and low serum thyroglobulin (J. Clin. Endo. Metab. 86:
3599, 2001).
Iodine is probably the element in shortest supply in
much of the inland world, and has placed a limit on the growth of populations there (J. Clin. End.
Met. 77: 878, 1993). Iodine deficiency in "democratic" Algeria (you know the problems): J. Clin.
End. Nutr. 79: 20, 1994. Haiti: Am. J. Trop. Med. 64: 56, 2001.
Benin: Am. J. Clin. Nutr. 72: 1179, 2000.
South Africa: Am. J. Clin. Nutr. 69: 497, 1999 and 71:
75, 2000. Ivory Coast Am. J. Pub. Health 89: 1857, 1999.
Iodine deficiency in Mainland China ("the people's paradise"): Am. J. Clin.
Nutr. 57(S2): 264S, 1993; NEJM 331: 1739, 1994; addressing the problem cost a whopping 12 cents
per person per year (Lancet 344: 107, 1994).
Tibetan children: Am. J. Clin. Nutr. 78: 137, 2003.
When mismanagement closed down the iodized salt program
in Morocco, hypothyroidism in children recurs in a few months: Am. J. Clin. Nutr. 79: 642, 2004.
Iodine deficiency in the preemie nursery: Arch. Dis. Child. 71: F-184, 1994.
Iodine deficiency in Europe's vegetarians and especially vegans (80%
-- it doesn't have to be this way): Ann. Nutr. Metab. 47: 183, 2003.
* For the very strange political
story of why Tasmania is presently iodine deficient,
see J. Clin. Endo. Metab. 85: 1513, 2000. For movies of the real
Tasmanian devil, the largest surviving marsupial carnivore,
click here
or here.
Manganese deficiency: Ultra-rare. Remember that manganese poisoning simulates Parkinsonism.
OBESITY
They are as sick that surfeit with too much as they that starve with nothing.
-- The Merchant of Venice, I ii 5 {07135} obesity
In America, even the beggars ("Homeless, hungry") are mostly well-fed, and many are fat;
and the poor are average much fatter than the rich (Am. J. Clin. Nutr. 79:
6, 2004).
Today's
late-teens and young-adult men average an inch taller than the US soldiers of WWII,
and two inches taller than the "doughboys" of WWI.
Any adult American who's "hungry" or has hungry children
either isn't taking advantage of the dole, or trading the food for drugs and
alcohol (J. Am. Diet. Assoc. 94: 749, 1994; article contains euphemisms). Yet our women (at least)
are leaner and more physically fit than their counterparts in poor nations (Columbia, at least; Am. J.
Clin. Nut. 60: 279, 1994). Even in most of the poorest nations,
overweight now exceeds underweight, especially among women
(Am. J. Clin. Nutr. 81: 714, 2005).
Of course our older children and
teenagers are getting fatter,
but those in the poor nations
are rapidly catching up
(Am. J. Clin. Nutr. 75: 971, 2002; Brazil and China).
I don't really think anyone was surprised to read that
sitting for hours and watching TV makes kids fat: JAMA 298: 1785, 2003.
Supposedly 64% of Americans are obese (Lancet 363: 339, 2004), etc., etc.
Your lecturer is not an expert on obesity and "bariatric medicine"
(probably the least-respected medical specialty, maybe unfairly), and can only contribute a few facts
to the perennial discussion....
Despite elaborate discussions of metabolic pathways (for example, Lancet 340: 404, 1992), the
fundamental laws of nature tell us that the bottom line on obesity is "calories in" (good food, junk
food, alcohol) versus "calories out" (basal metabolism, heat loss from the skin, work of breathing
and circulation, exercise, malabsorption, vomiting, tumor burden, chronic bronchitis and other nasty
diseases,
uncoupled oxidative phosphorylation, and just carrying around all that extra fat). Note
that carrying around fat takes work, maybe 9 calories per kg per day; this may be some of the reason
that most people find an equilibrium (NEJM 332: 621, 1995).
Distribution of body fat is determined by heredity and especially by steroid hormones (men get beer
guts, women get fat hips, Cushingism people get buffalo humps, etc.)
Factors in overeating include heredity, upbringing, real or hypothetical hypothalamic lesions
(Froehlich's, others), "peptides that regulate appetite" (pre-leptin era discussions sound plain-silly
nowadays), drugs (anabolic steroids, depot progesterone, and marijuana cause "munchies", while
"speed" and heroin
suppress appetite), and possibly "differences in metabolism" (i.e., thermogenesis, are your
mitochondria uncoupled? "non-exercise activity thermogenesis"
varies tenfold between lean and fat people: Science 283:
212, 1999 -- this seems to be holding up, and under the control of a vast
array of new hormones, including adiponectin, somehow acting on the nervous
system). Also, alcohol has calories and can make you fat (gee whiz!! NEJM 326: 983,
1992). Teaching obesity (by a crew who emphasize restricting fatty food): Lancet 340: 409, 1992.
Obese patients who "don't eat hardly anything", "exercise heavily" and are sure they have a problem
with their "glands" have long been suspected of harboring a subtle metabolic problem with
thermogenesis. In fact, almost all of them are kidding themselves and you about food and exercise
(NEJM 327: 1893, 1992).
* You aren't going to get people to comply with a weight-reduction diet that you prescribe.
There are some new medications that work on neurotransmitters,
but today's physicians are leery because of past fiascoes.
We now have pancreatic lipase inhibitors
to produce malabsorption (orlistat, others: Lancet 352:
160, 1998). The big deal in bariatrics is the discovery (Science 269: 475, 540, 543 & 546, 1995; NEJM 332:
679, 1995; Br. Med. J. 313: 953, 1996; Proc. Nat. Acad. Sci. 94: 4242,
1997;
Lancet 351: 737, 1998;
Ann. Int. Med. 130: 671, 1999) of leptin, a major
body hormone. It's the product of the Ob gene.
Injected, leptin makes rats eat less and lose weight, whether or not they are already obese. (The Ob+
obese rat, ob/ob, does not make the product. The Db- obese rat, db/db, lacks a proper leptin
receptor
in the brain: Proc. Nat. Acad. Sci. 93: 6231, 1996; Science 271: 913 & 994, 1995; NEJM 334: 324
1996.) Both rats overeat, get fat, and become diabetic.
Leptin is produced by the body's fat cells. It has three major known functions:
We are now starting Phase III trials of injectable leptin
to treat obesity; so far, results haven't been good and there's
been inflammation at the injection sites. Rats have been made to produce extra leptin
by gene therapy (!), and this renders them permanently slender
and the adipocytes actually de-differentiate (Proc. Nat. Acad. Sci.
96: 2391, 1999).
People with lipodystrophy (genetic or acquired loss of most of the adipocytes)
often are highly insulin-resistant and have hepatic steatosis as well,
and these tend to respond very favorably to leptin administration
(NEJM 346: 570, 2002).
When the business gets sorted out, I expect that we'll discover that we can adjust the adipostat setting
by exercise (which we've been doing for years) and drugs (which we've also been doing for years,
but we'll have safer ones).
I'll add the prediction that the tendency to overeat will correlate with abnormalities of the leptin
ligand-receptor system, and that we'll look back on "moral" and "educational" efforts to control
overeating as having been as futile as exhortations not to scratch when we itch.
Already we've shown that most human overeaters are
at least somewhat resistant to the effects of leptin on appetite
(NEJM 334: 293, 1996).
Mutant (ineffective) leptin is rare in humans
and results in extreme obesity beginning in infancy
(Endocrinology 140: 1718, 1999,
Nature 387: 903, 1997); of course they
are also insulin resistant. They respond
very well to injectable leptin (NEJM 341: 879, 1999).
* New information about obesity genetics keeps cropping up from the most
surprising places, for example your 5-HT2C serotonin receptor allele determines
whether you will get fat from taking antischizophrenic medicine (Lancet 359:
2086, 2002).
Around 5-10% of overweight humans are probably deficient in leptin,
despite the gene being normal (Proc. Nat.
Acad. Sci. 95: 11846, 1998). There's a new study suggesting that a
drop in plasma leptin (i.e., your fat stops making enough) precedes your middle-age blimp-up, at
least in one ethnic group (Nat. Med. 3: 238, 1997).
* Peptide YY administration suppresses appetite in obese humans,
and endogenous PYY levels are low in obese patients, suggesting that obesity
may have to do with deficiency in this hormone (NEJM 349: 941, 2003;
J. Clin. Endo. Metab. 90: 6386, 2005).
This is definitely one to watch.
* Watch neuropeptide Y, and its receptor, as permitting the normal
action of leptin to suppress appetite (Nat. Med. 5: 1085, 1096, & 1188, 1999.)
* Melanocortin 4 receptor mutations seem to produce binge eating (NEJM 348:
1085 & 1096, 2003; Nat. Med. 10: 35, 2004).
* Also watch ghrelin, an appetite stimulant and growth-hormone-secretogogue
produced by the stomach. Supposedly the presence of food in the stomach
stimulates its production at least in some folks.
(Perhaps it exists so people will fatten up when food is plentiful;
this isn't something we need nowadays.)
Ghrelin may explain why people lose weight after gastric surgery (bypass, other).
J. Neuroend. 14: 83, 2002; Endocrinology 143: 1353, 2002.
Obestatin is a newly-discovered hormone from the same prohormone
as ghrelin, but an appetite suppressant (Science 310:
996, 2005).
* Also watch small molecules derived from fragments on insulin
as appetite suppressants. Insulin receptors in the brain, when stimulated,
reduce appetite; mice lacking these are hyperphagic and obese but this is
corrected when they are given "small molecule insulin mimetics", which
work even orally (Nat. Med. 8: 179, 2002).
The uncoupling proteins are BIG news in themselves (Nat. Genet. 15: 269,
1997). We FINALLY
have a basis for saying "This person has a faster / less efficient metabolism" or "This drug / herb /
supplement burns fat". (NOTE: If this were really MOST of the obesity story, then the obese people
in the cafeteria wouldn't have more food on their trays than the skinnies. Go look.)
"Big Robbins" and "R&F" both define obesity to be "body weight 20% or more above the norm",
and by this standard, 20% of middle-aged men and 40% of middle-aged women in the U.S. are
"obese".
This generates many absurdities -- for example, it makes the best bodybuilders "obese". (In 1994,
the Kansas City Police tried to remove all "overweight" officers from duty, provoking successful
protests from the bodybuilders. As I've told you before, misapplied "science" hurts people.)
"Scientific" attempts to measure the "percentage of body fat" by measuring water displacement will
be severely affected by the amount of air in the lungs and gas in the bowel, and seem moronic to this
armchair non-expert (though patients may enjoy the swim; I'd like to see the effect of passing gas in
the swimming pool, always a pleasure, on the results of an individual's immersion study).
The recommendation that "your ideal weight was your weight at age 25" seems just as senseless,
and the loss of muscle and bone in old age masking obesity is only the
beginning of the problems.
The "ideal weight" graphs in popular books were adjusted up in the 1980's "to allow for the excess
mortality among people with very little body fat". This would put everyone on the track, swimming
and wrestling teams, and middle-aged folks who stay trim, at grave risk of premature death (which
of course, they aren't). And why the numbers should change so much with age baffles me. I looked
over some of the "evidence" and decided that the framers of these figures had averaged the cancer
patients, AIDS patients, and terminal alcoholics in with everybody else. Talk about stupid.
Since we're talking about bunk anyway, I offer the following without apology. I learned this
rule of "thumb": To determine your "build", wrap your thumb and index finger around the opposite
wrist.
* Another classic measure is "Quetlet's index" / "body mass index": If your weight in kilograms divided by the square of
your height in meters is greater than 30, you are so fat that it will probably shorten your life (Br.
Med. J. 302: 803, 1991). Of course, you'd think the index applies only to sedentary people with
scanty muscle mass. This has been the World Health Organization's standard
for decades, and is a poor choice since both exercising (good) and overeating (bad)
raise the index (Lancet 363: 157, 2004).
Yeah, this never made any sense and now most people
have gone back to
measuring waistlines (Br. Med. J. 326: 624, 2003).
* Yet another is "abdominal adiposity", i.e., his waist is bigger-around than his hips, i.e., the
dude's pants come down and you can see the crack in his behind when he
bends forward.
This is alleged to be a coronary risk factor. ("Metabolic syndrome X" and all that.
Watch the newly-discovered hormone resistin
as etiologic.)
On the other hand, many men (and some modern women) consider themselves obese if they cannot
see their muscle definition (tendinous inscriptions, etc.) as on the best athletes (who clearly are
healthy; a good abdominal "washboard" / "six-pack" / "ravioli" / "ice cube tray" is much sought-after by gym types).
{18645} muscle definition
The most sensible measure of body fat would seem to be the thickness of the triceps skin fold, and
that is how it is generally measured (the cited upper limit of good ranges from 1 cm to 1 inch).
Rather than define "obesity" or "excess body fat", let's just review the problems that fat causes:
Many cultures consider body fat to be un-aesthetic on one or both sexes. Other (less well-fed?)
cultures think it's gorgeous on one or both sexes.
Musculoskeletal problems (bad back, hips, knees) result from the sheet weight of fat. According to
contemporary studies, this is the most troublesome aspect of being fat (Br. Med. J. 301: 835, 1990).
For some reason, obesity seems to contribute to high blood pressure, and losing weight makes high
blood pressure easier to control. Nobody knows why (the explanations I've read seem pretty far-fetched.)
Lots of fat contributes to insulin resistance, and can unmask type II (insulin resistance) diabetes.
Nobody knows how this works, either.
Obesity somehow contributes to the development of gallstones.
"Fat is the surgeon's enemy", making surgery more of a physical problem, and perhaps delaying
healing (J. Am. Coll. Surg. 185: 593, 1997; idea dismissed Lancet 361: 2032, 2003).
Very obese people have trouble keeping their airways open, especially during sleep ("Pickwickian
syndrome", not the whole story).
The curious complex of insulin resistance, obesity, low HDL, androgen excess,
hirsutism,
secondary amenorrhea, and atherosclerosis risk remains baffling
and an important life-shortener
(Am. J. Med. 98(1A): 27-S, 1995, many others).
Obesity contributes to uterine cancer by enhancing activation of estrogens. (Supposedly. For the
same reason, women with very little body fat do not menstruate and are at extra risk for
osteoporosis.) By contrast, however, obese older women often have scanty or absent menstrual
periods "because the fat binds all the estrogens". (* Sound dubious to you, too?)
In extreme obesity, there is often a little fatty change in the liver, but nothing serious.
Somehow obesity supposedly raises serum uric acid levels and increases the risk for gout.
It is harder for a fat person to keep the intertriginous regions of the skin dry and clean, and skin
breakdown and superficial fungus infections are common here.
The physics of being fat may contribute to varicose veins.
Obesity supposedly also lowers HDL cholesterol, possibly causes left ventricular hypertrophy
(JAMA 266: 231, 1991, maybe from extra work carrying all that bulk; I'm not aware that this is necessarily
bad) and correlates with lack of
exercise and perhaps smoking and/or "stress"; all these (plus hypertension and diabetes) are "bad for
the coronaries", and losing weight reverses some of this effect.
Obesity pretty much disappears as a coronary risk factor when you control
for high cholesterol, high blood pressure, smoking, diabetes, and lack
of exercise.
Ask your internist. (The
claim that "fat makes the heart work harder because of the extra blood vessels" is basically a myth,
since these vessels are usually closed. You are lugging around more physical
weight. The epicardial fat pads are NOT atherosclerosis.)
There's a popular claim that adiposity, apart from hypertension, diabetes, tobacco, and so forth is an
independent risk factor. It usually doesn't hold up (Am. J. Pub. Health 84: 14, 1994).
It's true that really fat people seldom live to be very old. But even the latest
"big study" (Ann. Int. Med. 138: 24, 2003) controlled for smoking
but DID NOT control for high
blood pressure, diabetes, or failure to exercise. And it's hard to control
for the fact that somebody who's overweight may otherwise not be so health-conscious.
Given all the above, I have seen no clear evidence that being moderately fatter than the next person is,
by itself, anything more than a cosmetic problem.
When someone asks me, "Doctor, what is my
ideal weight?", my "unscientific" answer is, "Whatever looks and feels right to you".
HUNGER IN THE U.S.
Malnutrition is a common finding in the chronically sick (who may have malabsorption, may not
feel like eating, may not be able to afford good food, or may need help that
is not available)
In alcoholism, look first for folate and thiamine deficiency and protein-calorie malnutrition.
Vitamin A and vitamin B6, listed in "Big Robbins", are less obvious. The two cases of scurvy that I
have seen were both in chronic alcoholics.
Poverty, ignorance, stupidity, indifference and child abuse
are the causes of malnutrition of healthy
children. Simply putting single moms on the dole does not help if they are
physically or mentally sick (Am. J. Pub. Health 94: 109, 2004 -- documents what has
long been common knowledge.)
Prosecuting Texas parents who starve their children: Pediatrics 116:
1309, 2005.
Fad diets are seldom dangerous unless they are extreme (i.e., the "liquid protein" diets of the 1970's,
certain "macrobiotic" diets, the old "nothing but pineapple" diet, etc.). WORLD HUNGER (See CMAJ 173: 279, 2005):
Still our
world's most serious problem.
It is very difficult to 'love thy neighbor' when basic resources such as clean water, energy, land,
work, health care, and food are severely limited. These resources become daily more scarce because
of the policies of the leaders of [---] and [---]. A huge "underclass" exists on a global scale and is
evolving even within the richest nations. To organize an equitable distribution of basics worldwide
seems impossible; and we face a future of even more nationalism, racism, ethnic and religious
fanaticism, and ecological disaster. How to solve these problems nobody knows, but one thing is
clear -- that the larger the world population, the more difficult it will be to achieve peace and justice
on earth. Neglect of an effective birth control policy is a never-failing source of poverty
which in turn is the
parent of instability and crime.
All wars arise from population pressures.
Beyond a critical point within a finite space, freedom diminishes
as numbers increase. This is as true of humans in the finite space
of a planetary ecosystem as it is of gas molecules in a sealed flask.
The human question is not how many can possibly survive within
the system but what kind of existence is possible for those who do survive.
Perhaps the most important event of the twentieth century was the
demographic transition, the change in a population
from high-fertility and high-mortality
to low-fertility and low-mortality. In most of today's world, people now have a
reasonable expectation of living, and having their children live,
through healthy middle age. And there is far greater personal security
and many more opportunities
for a person to choose his or her path through life.
Antibiotics, safe surgery, sanitation, immunization, and reliable
birth control have made this possible. And of course real democracy
is at the heart of the change. As a result, fertility drops to
zero-total-growth. Today, the populations of the US, Northern Europe,
and Australia-New Zealand grow
only by immigration. And as less-developed countries such as
Mexico, Brazil, India, and Indonesia urbanize, the fertility rate has
been dropping dramatically.
In 1950, half the people in the world went to bed hungry.
Today, only about 1 person in 7 goes to bed hungry.
In 1960, the average person got 1900 calories per day; in 2000, it was up to 2700.
In the developing world, grain production per capita has grown from 155 kg/person
in 1960 to 225 kg/person today; the rise has been
basically steady. Much of this is the result of
the "green revolution" of the 1970's that
developed and introduced strains of
staple plants that grow more food when subjected to intensive irrigation and fertilization.
* We are often told that the prosperity
of the developed nations (including the health and opportunities
that we enjoy) is built upon, and depends upon, the poverty
of the rest of the world.
This is dogma in many "progressive"
circles. (It's a favorite claim of many of my fellow-Anglicans.)
And it is noxious falsehood.
It's true that many countries use natural resources to produce
luxury goods for export while they still have hungry citizens.
But this contributes very little to the prosperity of the developed
world, which is based on the rule of law and government policies
that promote a strong economy and opportunity for anyone willing
to work hard.
No one has been able to explain to me how
I am enriched by
the hunger of a child in a kleptocracy where being honest, smart and
hard-working gets you nothing (or gets you in trouble or dead) -- a fact
that the Left simply ignores.
More on this below.
Only a fool or an ideologue could believe that we could feed our 6 billion people
without chemicals and other technology. And the Green Revolution has not been without its problems.
Radical
irrigation programs have contributed to the expansion of the world's deserts.
So has the kind of overcultivation that leads to the washing
away of soils. And even fertilizers, of course, damage soil over the long run.
You'll hear many different claims about just how serious this is; I have noticed
that very little is being written in refereed scientific journals about
soil depletion as a long-term threat.
I do expect that there will be some new conflicts over water availability
in the next decade, especially in India, Pakistan, North China, and the
Middle East.
When (not "if")
we run out of petroleum, we will need an alternative
source of
cheap energy to continue producing fertilizer. (I'm hoping for controllable nuclear fusion, but this may never be possible.
Perhaps I'll live long enough to see construction begin on the huge solar panel in the Sahara...)
Most
of the suffering is borne by children (Br. Med. J. 304: 1423, 1992); in fact,
as recently as the 1980's,
around 40% of the children in the developing world
died before reaching age 5 (Med. J. Aust. 154: 227, 1991), and in
the large majority of cases, malnutrition is at least a major contributing factor.
In some poor
countries, population has doubled every 17 years (Lancet 33: 1705, 1990), with hunger providing the
principal brake on an even more rapid rate of increase. Although the U.S., Canada, Northern
Europe, and Australia have populations that grow only by immigration, the world's population is
now increasing at the rate of 96 million per year. We learn with
hope of a spectacular
drop in fertility during the 1990's throughout
the historically poor nations of Asia and Latin America
as young adults see
a future of greater
economic opportunity and personal freedom in the new democracies.
We can hope that someday that this will be true everywhere.
The average woman in Senegal has seven children
(Science 266: 771, 1994), and this is typical for sub-Saharan Africa, where the problem
is by far the worst.
Allow around 40% child mortality from malnutrition, and the population there still doubles every
generation, about every 25 years. In Jamaica (in our own back yard),
simply alleviating hunger in the classroom makes for vast improvements
in learning (Am. J. Clin. Nut. 67: 790-S, 1998).
In the early 1990's, health care and quality-of-life
standards plummeted as sub-Saharan Africa went broke (Lancet 345: 182,
1995).
There was talk about "the malthusian ceiling"
being approached (Lancet 341: 669, 1993). And not surprisingly,
famine,
epidemic disease, and race wars followed.
In the early 1990's, the single country with the worst numbers was Rwanda
(Br. Med. J. 311: 1651, 1996); we all saw what happened, and more of the same will happen soon
in the area. In the 1994 edition of these notes, I predicted
the explosion in Sierra Leone, which soon followed and
which the world ignored.
(The "rebels" in this weird war
had a special fetish for performing machete
amputations on children. War crimes trial began 2004.)
The Taliban kept the ordinary people of Afghanistan under-nourished
(JAMA 286: 2723, 2001).
In the past few years, several of the sub-Saharan countries
have made dramatic turn-arounds.
In 2000, crop failures in Ethiopia were massive but there
was no famine as the world relief agencies were able to
come in unhindered (JAMA 286: 563, 2001; Lancet 358:
498, 2001; Lancet 362: 1808,
2003).
Rescuing children from famine in Guinea-Bissau: Am. J. Clin. Nutr. 80: 1036, 2004.
At the same time, Kabila's famine claimed the lives of
at least 2.5 million people in the Congo alone, where misgovernment,
population pressures,
famine, economic
collapse, and civil war perpetuate one another. Now it's Mugabe's famine
in Zimbabwe, Mwanawasa's famine in Zambia, the genocide in Darfur (NEJM 351: 2574, 2004;
Br. Med. J. 330: 110, 2005; Lancet 364: 1315, 2004; JAMA 293:
2212, 2005), and the Niger famine (the world's poorest country;
the aid from 2004 was taken
by profiteers and sold to the highest bidder: Lancet 366: 1067, 2005..
Starvation in "the new South Africa": Lancet 363: 1110, 2004.
The rest of the world does not even seem to be paying attention.
The world has only recently begun talking straight about the problem,
especially in sub-Saharan Africa. As recently as the 1990's,
there were still outcries from extremists on both Right and Left against
condom distribution. (The last bastion of anti-condom activism now resorts
to obviously false claims, i.e., that sperms and HIV viruses easily
penetrate the membrane: Nat. Genet. 9: 1443, 2003).
Events like the 1992 "Earth
Summit" produce enormous documents about how to "conserve the environment", "maintain
wilderness areas", and "preserve species diversity" while keeping strict politick silence on population
growth to please certain powerful politician-ideologues. One spectacular change
was the embracing of thoughtful population-control policies by mainstream
Islam:
Lancet 343: 583, 1994. Today, the Islamic Republic of Iran has an extremely strong
and highly successful family-planning program: Stud. Fam. Plan. 31: 19, 2000.) The taboo about talking of population:
Br. Med. J. 315: 1441, 1997.
Under this misgovernment, a large family offers the only economic security or
opportunity for personal satisfaction, and a family's survival often
depends upon child labor (especially in rural areas, Sci. Am.
272(2): 40, 1995). Here only 1 couple in 3 uses any kind of birth control (reports vary widely, though,
from nation to nation; for example, in Nigeria the large majority of teenaged girls are sexually
active, only 5% have ever used a modern contraceptive, and 25% have had an elective abortion:
Lancet 345: 300, 1995).
Overpopulation, hunger, and poor health clearly work in
the interests of the hoodlum governments. On the flip side, the people now running
most of the world (i.e.,
the capitalists of the global economy) are quite content with widespread poverty
and hunger, since it keeps labor costs down in the sweatshops where the poor
people make the rich people's luxury goods.
Most rich and most poor people want access to birth control,
regardless of their religion (Lancet 342: 447, 1993; article contains blunt talk); yet certain religious
denominations use their political clout in the poor nations to make this hard-to-get (Lancet 342: 473,
1993; more blunt talk; this article sparked a fire-storm and was part of the basis for review by
the
Islamic leaders). The world's most prominent proponent of "the consistently pro-life ethic"
(which I admire) appears to be
more upset by stem cell research, capital punishment, and artificial contraception than
by world hunger (despite lip service to "the need for development").
This saddens me. Population policy in the poor nations (whatever else, we
need to diminish their need-desire for large families): Science 263: 71, 1994.
In addition to overt protein-calorie malnutrition, hungry people are more subject to a host of
infectious diseases, including measles, malaria (Am. J. Trop. Med. 71(S2): 55, 2004),
and the parasitic infestations.
As used by social scientists, poverty means a total income less than three times the cost of a healthy,
varied diet. Absolute poverty means a total income less than the cost of a diet sufficient to allow the
person to work at his or her maximum capacity. Presently, one human being in seven lives in absolute
poverty.
As with all discussions of science and policy, public discussion of world hunger is marred by
disinformation campaigns by the "right", the "left" and the "greens". In particular, you will hear the
current "green / animal rights / vegetarian" claims that world hunger is caused largely by animal farming. It's
clearly not true (Nature 355: 582, 1992).
If you can't see through the disinformation campaigns
(Sci. Rev. Alt. Med. 1: 36, 1998), you don't know basic
biology.
Today there is actually a global
grain surplus, which is fed to animals.
It is still dogma in many left-wing circles that cattle ranching
is the basis of both world hunger and global warming.
And this is obvious disinformation.
What do you plan to do with semiarid range land if you do not raise
grazing animals?
Think about the alternatives (i.e., millions of unmanaged herd animals, dying of
old age and rotting where they fall -- while hungry children starve
in the rest of the world. What's this about "cruelty"?)
And
even the one scientific publication I could find on the subject
of methane in cattle flatus causing the greenhouse effect
estimated the contribution at "a little less than 2%" of the total
(J. Animal Sci. 73: 2483, 1995). And the much-missed buffalo herds didn't f*rt?
And so forth,
ad nauseam.
Of course, ideology has had a terrible impact on global hunger.
The greatest famines of modern times were
brought about by the stupidity of the Communist superstates.
Stalin's biology
guru was Thaddeus Lysenko, a left-wing kook
who was repelled by scientific biology's vision of a competitive world
(too much like capitalism). Lysenko (and Stalin) believed that "living things strive for higher
perfection" (harmony-in-nature, cabbages want to be good socialists,
etc., etc). Stalin killed the bioscientists
who dared to disagree. Lysenko's beautiful mysticism led to
moronic agricultural
policies (much of Russia was planted with crops --
including some weird hybrids -- that could not
possibly have grown where they were planted), enormous crop failures, and the deaths of around
10,000,000 Soviets. During Mao Zedong's "Great Leap Forward" in 1959-1961,
between 36 and 50 million Chinese died as a result of similar
ill-advised land-management policies, frustrating Mao's intention
to overpopulate China and use the surplus
as cannon-fodder as he had done so successfully in Korea.
(The awful population increase
came later, with government policies encouraging large families.)
Mao sought (as he put it himself) to "conquer nature".
Mao actually
announced that he was going to exterminate sparrows and field mice.
Lysenko sought "harmony with nature".
Neither actually understood nature.
I'd welcome a talk in lab (instead of doing a patient case) on this
important topic.
The North Korean famine of the 1990's was also caused by government policies
that seem to be deliberate: Lancet 345: 291, 1999.
Less ideological...
Saddam Hussein prevents good people from bringing food to Iraqi children
in order to mobilize world opposition to sanctions against his regime:
Ann. Int. Med. 132: 155, 2000; Lancet 355: 1851, 2000.
And malnutrition among Palestinian children
in the Gaza strip is far worse than in most other poor
nations (Br. Med. J. 325: 1057, 2002).
In 1989, I was told by one influential Kansas "bioethicist" (a non-scientist and
quasi-Marxist "liberation theologian" of sorts, who shall remain nameless here), "If we
just had 'economic justice', our world could easily support 50,000,000,000 people." Get real.
Likewise, only an
ideologue would agree with the Reagan administration's right-wing
1984 pronouncement that world population
growth is not a problem, but a "neutral phenomenon".
One may admire what one hears about Mother Teresa's
work with the orphans of Calcutta,
and it is hard to escape the irony -- her
strong opposition to all forms of birth control was well-known. (A
horrifying account of Mother
Teresa's "charitable work"
from a physician who actually saw it firsthand: Lancet 344: 807, 1994).
The answers to world hunger have come from
science, reasonable security, and reasonable freedom.
Mainland China's introduction of limited
free enterprise resulted in greatly increased agricultural output.
Food production literally doubled as soon as individual farmers were allowed to manage their
own farms and make a small profit; Vietnam had the same thing happen beginning in 1986, when
private farming replaced collective farming. (So much for Marxist revolutionary
"economic justice", huh?)
China is now self-sufficient, feeding 1/5 of the world's population
on 1/15 of the farmland.
The result has been substantial growth for its children (NEJM 335: 400, 1996. The
left-wing authors of this curious paper do not see this reflecting the awful truth about socialist
government, but spend most of their paper complaining the "improvement has not been equitable",
i.e., many kids are still growth-stunted in the communist rural zones but few kids are stunted in the
capitalist urban zones.)
In Cairo (1994, review Lancet 353: 315, 1999),
most of the world (even the kleptocracies) paid lip-service to population control,
sought cost-effective forms of birth-control and laughed (publicly) at the anti-contraception
religionists. Curiously, delegates didn't complain much (though some did) about "Western cultural
imperialism" as the cause of the worldwide "redefining of sexual roles" (i.e., a woman can decide
whether or not to have sex before marriage, who and whether she will
marry, and about birth control inside or outside of marriage).
We'll hear about the "Cairo Mandate" in the future, and it may help.
I would prefer real democracy (i.e., the ability of the world's poor to
force their governments to become representative) to any other solution.
You will need to decide for yourself about the current
left-wing "good cause" of debt-relief without accountability
for past or present kleptocracies,
in the hopes they will
pass the benefits along. The late unlamented Mobutu Sese Seko's
$5 billion dollar estate would be enough to pay the current
foreign debt of the Congo, the nation that he looted
during his decades in power.
Even the Africans now say that the past two decades of "neoliberal
policy" (i.e., the developed nations
providing financial support for the corrupt governments) is
a major cause of the declining standards of health and nutrtion,
and that the current "debt relief initiative" is just more of the same
(Int. J. Health Serv. 33: 607, 2003).
By contrast, debt relief
for governments that actually give evidence
of governing responsibly and caring
for their people is an established
fact, supported by a major act of Congress and occupying much of the
focus of the International Monetary Fund and World Bank
(Health Policy & Planning 18: 138, 2003; Bull. WHO 80: 151, 2002).
In the next decade, pay special attention to individual nations, and how
government policies affect hunger. When individuals are guaranteed the right
to their own land and to the profits from farming, the demographic transition
will take place, and the world will be astonished. When governments (using whatever
excuses) interfere, expect continued famine. I would hope that the world financial
institutions do what they can to make governments choose the right path for their people.
Ultimately, I
would hope for a world in which it is the norm for people to be able to find satisfaction, fulfillment,
and security without having babies they can't afford to raise, and enjoy a reasonable chance for a
healthy life. Dr. Virchow's prescription of "true and complete democracy" is also my prescription.
There has never been a famine in a real democracy, no matter how poor.
Democratization requires breaking the cycle of poverty, tyranny, corruption,
maladministration, frustration, violence, and
stupid right-wing and left-wing ideologies. Can this happen? After
25 years as a physician, I think I'm finally seeing it. And so do others
(Am. J. Pub. Health. 90: 1838 & 1841, 2000). But I do know that
physicians are the natural leaders in understanding and clarifying the problems that cause world
hunger, and in finding solutions.
LAST STUFF Irradiating food to kill microbes is a well-established technology
and is obviously safe. For decades, the anti-nuclear
movement had succeeded in blocking
radiation of food, even though it will go a long way to prevent the 2000-odd annual
US deaths from salmonellosis and lower the 20% spoilage loss of
food in the poor nations. Of course, the problem
was ideology (and of course expense),
rather than any realistic health dangers of "nuked food".
"Environmentalist" broadsides merely cite the possibility of a
radiation leak (so should
we close down the cesium-137 treatment units in hospitals, Ralph?), and alleged
production of trace amounts of a single suspected carcinogen (so are
you going to stop eating pepper, Ralph?)
Even the folks who have found
"scientific evidence" of the health risks of such things as
agent orange and electrical power lines never published on this.
For reviews, see JADA 96: 59, 1996; Am. Fam. Phys. 47: 1064, 1993.
Dairy Queen introduced nuked burgers in the early 2000's,
and thankfully this attracted almost no attention from the mainstream.
We have already reviewed "Diet and Cancer" under "Neoplasia". The material in "Big Robbins" is
highly speculative. Worth remembering for USMLE/COMLEX:
There's a fairly convincing link between low-roughage diet (i.e., less complex-carbohydrate, not less
cellulose) and colon cancer. Whatever it is in the vegetables that's protective, it's not the vitamin C
or the vitamin E (NEJM 331: 141, 1994).
High animal-fat diet was never plausibly linked to breast cancer, and the idea now seems to be
discredited. (More about this later.)
A group in Hawaii looked at lung cancer and found no correlation whatever with anything whatever
in the diet (Arch. Env. Health. 48: 69, 1993).
The epidemic Chinese throat cancer has been tentatively linked to ingestion of a fungus-rich, pickled
salt-fish ethnic delicacy.
Bad diet (lots of iron, lots of aflatoxin) conspires with hepatitis B infection to produce liver cancer in
poorer nations.
Women who have very low levels of vitamin A are indeed at greater risk for breast cancer, but
beyond this, there's no apparent benefit from extra vitamin A in preventing breast cancer. No
relationship between vitamin C and breast cancer could be found (NEJM 329: 234, 1993).
* A huge study in a Red Chinese population with a tremendous prevalence of esophageal and
stomach cancer found a small reduction of these tumors in patients supplemented with tablets
containing vitamin A, vitamin E, and selenium. No effect was demonstrated for retinol plus zinc,
riboflavin plus niacin, or vitamin C plus molybdenum. JNCI 85: 1483, 1993.
* Calorie restriction in experimental animals, notably Li-Fraumeni mice, delays the average onset
time of their cancers. Nobody has any idea why, unless perhaps epithelial cells turn over less in
hungry critters (Proc. Nat. Acad. Sci. 91: 7036, 1994).
NOTE: Do yourselves a favor and read a chapter on nutrition in a good "path" book. I especially
recommend the sections in "Big Robbins" on diet and systemic disease, and diet and cancer, for your
own interest. Decide for yourself about the questions raised, after reviewing the evidence in the
references. If you want nitrites removed from food, please either get hot dogs banned altogether or
find another way of preventing botulism. I believe "Big Robbins" is being over-cautious in
questioning the usefulness of dietary modification in preventing and reversing atherosclerosis.
NOTE: In recent years, the single clear instance of "a poisonous chemical in our food" was 1,1'-ethylidenebis[tryptophan].
This impurity caused the gruesome eosinophilia-myalgia syndrome in
hundreds of health food store patrons (Review: Mayo Clin. Proc. 66: 535, 1991).
 I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
Pathology Education Instructional Resource -- U. of Alabama; includes a digital library
Houston Pathology -- loads of great pictures for student doctors
Pathopic -- Swiss site; great resource for the truly hard-core
Syracuse -- pathology cases
Walter Reed -- surgical cases
Alabama's Interactive Pathology Lab
"Companion to Big Robbins" -- very little here yet
Alberta
Pathology Images --hard-core!
Cornell
Image Collection -- great site
Bristol Biomedical
Image Archive
EMBBS Clinical
Photo Library
Chilean Image Bank -- General Pathology -- en Español
Chilean Image Bank -- Systemic Pathology -- en Español
Connecticut
Virtual Pathology Museum
y
Australian
Interactive Pathology Museum
Semmelweis U.,
Budapest -- enormous pathology photo collection
Iowa Skin
Pathology
Loyola
Dermatology
History of Medicine -- National Library of Medicine
KU
Pathology Home
Page -- friends of mine
The Medical Algorithms Project -- not so much pathology, but worth a visit
National Museum of Health & Medicine -- Armed Forces Institute of Pathology
Telmeds -- brilliant site by the medical students of Panama (Spanish language)
U of
Iowa Dermatology Images
U Wash
Cytogenetics Image Gallery
Urbana
Atlas of Pathology -- great site
Visible
Human Project at NLM
WebPath:
Internet Pathology
Laboratory -- great site My team:
My team:Ed Lulo's Pathology Gallery
Bryan Lee's Pathology Museum
Dino Laporte: Pathology Museum
Tom Demark: Pathology Museum
Dan Hammoudi's Site
Claude Roofian's Site
Pathology Handout -- Korean student-generated site; I am pleased to permit their use of my cartoons
Estimating the Time of Death -- computer program right on a webpage
Pathology Field Guide -- recognizing anatomic lesions, no pictures

St.
Jude's Ranch for Children
I've spent time there and they are good. Write "Thanks
Ed" on your check.
PO Box 60100
Boulder City, NV 89006--0100
More of my notes
My medical students
Clinical
Queries -- PubMed from the National Institutes of Health.
Take your questions here first.
HealthWorld
Yahoo! Medline lists other sites that may work well for you

We comply with the
HONcode standard for health trust worthy
information:
verify
here. 

![]()
-- Frederic Bastiat
-- James 2:16
-- Adlai E. Stevenson
--
Charles Darwin
--
James Thurber
Describe the epidemiology, anatomic pathology, pathophysiology, and overall
impact on the human race of each of the following:
total calorie malnutrition (marasmus)
protein malnutrition (kwashiorkor)
vitamin A deficiency
vitamin A toxicity
vitamin D deficiency
vitamin D toxicity
vitamin E deficiency
vitamin K deficiency
thiamine deficiency
niacin deficiency
biotin deficiency
pyridoxine deficiency
cyanocobalamin deficiency
vitamin C deficiency
vitamin C toxicity
folic acid deficiency
iron deficiency
zinc deficiency
copper deficiency
selenium deficiency
iodine deficiency
endemic goiter
Kashin-Beck epidemic osteoarthritis
Keshan epidemic cardiomyopathy
Strachen's epidemic polyneuropathy
poverty
absolute poverty
demographic transition
 INTRODUCTION
INTRODUCTION
For example... In my 20-plus years as a medical school teacher, I have never taught (or believed)
that fat / saturated fat in the diet is "bad" for
ordinary folks. Nor, despite decades of trying,
is there any hard evidence that this is true. How this longstanding
crock was perpetrated
on the public: Science 291: 2536, 2001.
With the welfare cutbacks of the mid-1990's, hunger began
prompting more of the poor to seek hospital admission. The authors
of the major study concluded that if you have an income of less than $10,000
or were on drugs, you might not always have enough to eat
(JAMA 279: 1211, 1998). Similarly, poor diabetics
getting sick from skipping meals is becoming much more common
(JAMA, same source).
Underclass children are now going hungry
even in oh-so-progressive Massachusets (Pediatrics 110: e41, 2002).
In the U.S., faddism by parents can and does cause kwashiorkor in children:
Arch. Derm. 137: 630, 2001.
{46293} kwashiorkor
{46294} fatty liver in kwashiorkor
Vitamins in general:
"Recommended daily allowances" are just that. Researchers see how much
a person needs to take daily in order to reach maximum plasma levels,
and perhaps saturate white cell cytoplasms (Proc. Nat. Acad. Sci. 98:
9942, 2001). Obviously this is easier for the water-soluble vitamins than
for the fat-soluble ones.
In the poor nations, no reasonable person doubts the value of iron plus folic acid
for pregnant women. Adding other nutrients seems to offer no advantage (Br. Med. J. 326:
571, 2003).
 Vitamin A (Lancet 345: 31, 1995)
Vitamin A (Lancet 345: 31, 1995)
Vitamin A deficiency also makes the eye more vulnerable to trachoma.
Long-believed, this is now proved: Lancet 357: 1676, 2001.
Obviously, the pop idea that eating carrots further enhances healthy
night vision is erroneous. The fact that this idea persists suggests how
extensive vitamin A deficiency was until the late 20th century.
Women
in countries where they are required to remain veiled
when they go outdoors are at greatly increased risk
for rickets (Eur. J. Clin. Nutr. 50: 315, 1996; in sunny
Kuwait, can you believe it?!).
{15919} rickets, sub-periosteal bone is forming strangely
{15921} rickets, rib; that growth area just doesn't look right....
{38183} rickets, bow-legs
* The silly flap over vitamin K injections in babies
causing leukemia: Br. Med. J. 316: 173,
1998. Of COURSE not. Nowell's law
triumphs once again.
* Thiamine deficiency in contemporary Thailand:
Lancet 353: 546, 1999.
 Pellagra
Pellagra
Patient had diarrhea, mental changes also
McGill Center for Tropical Disease
By now, the usefulness of folate supplementation in preventing neural
tube defects is obvious.

The vegan community itself is well-aware of the risk of permanent brain damage
from the diet, especially among children (Am. J. Clin. Nutr. 71: 1211, 2000).
Still, horrendous cases happen (J. Ped. Heme. 26: 270, 2004).
It is hard to sort out the effects of an unsupplemented vegan childhood
from continuing deficiency despite some supplementation, but the effects
are measurable:
Am. J. Clin. Nutr. 69: 664, 1999 (biochemistry); Am. J. Clin. Nutr. 72:
762, 2000 (biochemistry and cognitive function tests).
* The B12-IF receptor is cubilin, which of course has other functions:
Nat. Med. 5: 656, 1999.
 Vitamin C (ascorbic acid)
Vitamin C (ascorbic acid)

Jacques Cartier and his fellow-explorers suffered terribly from scurvy
during the cold Canadian winter of 1535-6. They would probably have died
had the local Indians not taught them how to brew tea from a local
evergreen.
{46398} scurvy, sub-periosteal hematoma; this hurts
{38195} scurvy case, bone, osteoid has formed poorly (tiny trabeculae), there is a bleed
 Scurvy
Scurvy
Scorbutic rosary, bleeding gums
McGill Center for Tropical Disease
Victims include
menstruating women on inadequate diets (junk food, fast food -- NEJM 321: 752, 1989 -- poverty),
anybody on the strict "macrobiotic" vegetarian diet,
rapidly growing youngsters, infants fed only milk (Arch. Ped. Adol. Med. 159:
1038, 2005), pregnant women (the
fetus is a potent drain on iron), people with known (blood donor) or unknown (ulcers, GI cancers,
hookworm, self-induced illness, etc., etc.) blood loss, and people who eat iron-binding substances
(laundry starch, clay).
* Fatal zinc toxicity from somebody who ate a bunch of US pennies, which
are now mostly zinc: AJFMP 18: 148, 1997.
Worth mentioning: In Menkes' kinky hair
disease, copper is not used properly by the body. (* Victims of this gruesome rarity cannot
weave keratin or collagen, or pigment their hair. They die of a scurvy-like disease early in
childhood. Gene cloned Nature 361: 98, 1993).
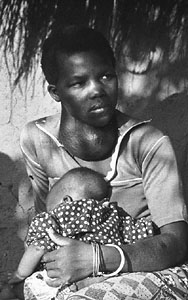 Iodine deficiency
Iodine deficiency
I have more flesh than another man, and therefore more frailty.
-- Shakespeare's Falstaff, I Henry IV III iii 187
The first thing a successful dieter must learn is to distinguish hunger ("I'm physically hungry right
now") from appetite ("Ummm, that's looks good!"; "Because of what's happening to me right now,
I'd like the emotional solace of putting something in my stomach.") Chubbier people tend to be
those who do not satiate after eating fat (Am. J. Clin. Nut. 60: 476, 1994) or who depend on
carbohydrate to keep their serotonin levels up (?! -- get out the Prozac, Am. J. Clin. Nutr. 60: 476,
1994).
)window.location='http://artchive.com/artchive/R/rubens/bacchus.jpg.html')
 ob/ob mouse
ob/ob mouse
Fat mouse cannot make leptin
Source unknown
* Watch these proteins. Tumor necrosis factor also induces them,
accounting for its thermogenic and weight-reducing effects
(Eur. J. Clin. Bioch. 29: 76, 1999).
* In fact, I have taught the politically incorrect idea that non-extreme obesity, by itself
and not as an indicator of otherwise-poor self-care,
is not a health risk ever since I started in the late 1970's.
But it's common sense.
This now has strong empirical support despite all the government and pop-culture
hoopla. Americans are fatter than we were even in the 1950's. But where is
the excess mortality? Live expectancy rises, and incidence and deaths from stroke and heart attack
drop steadily even as we get fatter and fatter. Finally, full-time scientists
are saying the same thing. See especially Sci. Am. 252(6): 70, June 2005, "Obesity: An Overblown
Epidemic", which reviews what I've always believed and give you the facts so
that you can begin thinking about how this particular crock was perpetrated on
the American public.
(Uh, you decide.
The business people couldn't be trying to sell us anything, could they?
The entertainment industry, showing us skinny "beautiful people", couldn't
be trying to get business for sponsors, could it?
The government couldn't be trying to take our minds off something else, could they?)
* Note: The "Mayo Clinic
Diet", based around grapefruit, has nothing to do with the Mayo Clinic, whose lawyer tells me that
they do indeed go after the diet's proponents whenever they use the name.
-- Lancet 342: 473, 1993 (read it all)
-- Aristotle, The Politics, c. 334 B.C.
-- Robert Heinlein
-- Frank Herbert, Dune
 "Big Robbins" eloquently describes the problem of people simply not having
enough to eat. There is a great deal of bad information about the causes
and possible remedies for world hunger, and there are many opportunities
for people with agendas to lie with statistics.
"Big Robbins" eloquently describes the problem of people simply not having
enough to eat. There is a great deal of bad information about the causes
and possible remedies for world hunger, and there are many opportunities
for people with agendas to lie with statistics.* Average grain production per person worldwide
peaked in 1984 at 344 kg/person and has been declining slightly
ever since. The real reason is that people in the developed nations
simply cannot eat any more, or even feed any more to the animals we eat.
And there are many more people in the developing world.
This statistic is often cited by "environmentalists" as a sign of
impending disaster. Do you see the fallacy?

The bottom line is that in today's world, all hunger is political, i.e., there is plenty
of food to feed everyone, including the
children.
The problem is in the distribution -- and herein lies the ongoing problem.
Yes, it's baffling (J. Am. Diet. Assoc. 103: 1046, 2003) -- especially
if you don't think the near-unthinkable.
Right or wrong (or
neither), hunger remains the major means of keeping people under control
throughout the poor nations.
Wherever there is widespread hunger, it is because people
with guns are preventing good
people from the rest of the world from bringing in food.
Following Virchow, and most reasonable people nowadays, I place
most of the blame for today's world hunger on misgovernment in the
poor nations.
Today's medical literature is no longer keeping silent, either:
Lancet 359: 2030, 2002.
The economic disparities between rich and
poor in today's kleptocracies far exceeds those under colonialism.
Too many countries are still governed by hoodlums
toting cast-off U.S. and Soviet-made machine guns.
Governments are indifferent to the
well-being of the governed, "Aid for International Development" usually doesn't reach the
poor (Br. Med. J. 311: 72, 1995).
Our military
campaign in Somalia ("Operation Restore Hope") was undertaken to end a famine,
and ended with our realizing the horrible truth -- tyrants
don't want famine to end. See JAMA 272: 386, 1994,
CMAJ 149: 1522, 1993; Lancet 342: 190, 1993.
Zimbabwe's Mugabe collapsed his own country's economy
by calling for "justice" and
seizing the productive land for his family and
friends (CMAJ 163: 1616, 2000; Lancet 359: 455, 2002).
And in 2002, during a famine in his country, Zambia's
president Levy Mwanawasa simply impounded the maize that the US donated and let
it rot. Of course, he claimed to be outraged because the maize had been
genetically modified, just the same as people in the United States
and Canada eat every day. ("I refuse to allow my people to be used as
guinea pigs." "There's no justification for feeding people 'poison'."
"We may be poor and experiencing severe food shortages, but we aren't ready
to expose our people to ill-defined risks.")
See Lancet 360: 1261, 2002, and draw your own conclusions.

* Even the postmodernists
and super-multculturalists have wised-up to
the abuse of aid: see "The Symphony of the Damned: Racial Discourse, Complex Political
Emergencies, and Humanitarian Aid", Disasters 20: 173, 1996, which describes third-world
hoodlums demanding "justice"
and putting the Free World's disaster relief into their
private bank accounts; "This functional ignorance has allowed a widespread incorporation of
humanitarian aid into the fabric of political violence. Developmentalism is an essential
underpinning for the growing organizational accommodation to ongoing conflict and eroding
standards of justice and accountability".


| 2005: |
Ed says, "This world would be a sorry place if
people like me who call ourselves Christians
didn't try to act as good as
other
good people
."
Prayer Request
 Teaching Pathology
Teaching Pathology
PathMax -- Shawn E. Cowper MD's
pathology education links
Ed's Autopsy Page
Notes for Good Lecturers
Small Group Teaching
Socratic
Teaching
Preventing "F"'s
Classroom Control
"I Hate Histology!"
Ed's Physiology Challenge
Pathology Identification
Keys ("Kansas City Field Guide to Pathology")
Ed's Basic Science
Trivia Quiz -- have a chuckle!
Rudolf
Virchow on Pathology Education -- humor
Curriculum Position Paper -- humor
The Pathology Blues
 Ed's Pathology Review for USMLE I
Ed's Pathology Review for USMLE I
![]()
![]()
 | Pathological Chess |  |
 |
Taser Video 83.4 MB 7:26 min |

 Vitamin A deficiency
Vitamin A deficiency Scurvy
Scurvy Iodine deficiency
Iodine deficiency