Ed Friedlander, M.D., Pathologist
scalpel_blade@yahoo.com



Cyberfriends: The help you're looking for is probably here.
Welcome to Ed's Pathology Notes, placed here originally for the convenience of medical students at my school. You need to check the accuracy of any information, from any source, against other credible sources. I cannot diagnose or treat over the web, I cannot comment on the health care you have already received, and these notes cannot substitute for your own doctor's care. I am good at helping people find resources and answers. If you need me, send me an E-mail at scalpel_blade@yahoo.com Your confidentiality is completely respected.
 DoctorGeorge.com is a larger, full-time service.
There is also a fee site at myphysicians.com,
and another at www.afraidtoask.com.
DoctorGeorge.com is a larger, full-time service.
There is also a fee site at myphysicians.com,
and another at www.afraidtoask.com.
Translate this page automatically
 |
With one of four large boxes of "Pathguy" replies. |
 I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
Numbers in {curly braces} are from the magnificent Slice of Life videodisk. No medical student should be without access to this wonderful resource. Someday you may be able to access these pictures directly from this page.
Also:
Medmark Pathology -- massive listing of pathology sites
Freely have you received, freely give. -- Matthew 10:8. My
site receives an enormous amount of traffic, and I'm
handling about 200 requests for information weekly, all
as a public service.
Pathology's modern founder,
Rudolf
Virchow M.D., left a legacy
of realism and social conscience for the discipline. I am
a mainstream Christian, a man of science, and a proponent of
common sense and common kindness. I am an outspoken enemy
of all the make-believe and bunk that interfere with
peoples' health, reasonable freedom, and happiness. I
talk and write straight, and without apology.
Throughout these notes, I am speaking only
for myself, and not for any employer, organization,
or associate.
Special thanks to my friend and colleague,
Charles Wheeler M.D.,
pathologist and former Kansas City mayor. Thanks also
to the real Patch
Adams M.D., who wrote me encouragement when we were both
beginning our unusual medical careers.
If you're a private individual who's
enjoyed this site, and want to say, "Thank you, Ed!", then
what I'd like best is a contribution to the Episcopalian home for
abandoned, neglected, and abused kids in Nevada:
My home page
Especially if you're looking for
information on a disease with a name
that you know, here are a couple of
great places for you to go right now
and use Medline, which will
allow you to find every relevant
current scientific publication.
You owe it to yourself to learn to
use this invaluable internet resource.
Not only will you find some information
immediately, but you'll have references
to journal articles that you can obtain
by interlibrary loan, plus the names of
the world's foremost experts and their
institutions.
Alternative (complementary) medicine has made real progress since my
generally-unfavorable 1983 review linked below. If you are
interested in complementary medicine, then I would urge you
to visit my new
Alternative Medicine page.
If you are looking for something on complementary
medicine, please go first to
the American
Association of Naturopathic Physicians.
And for your enjoyment... here are some of my old pathology
exams
for medical school undergraduates.
I cannot examine every claim that my correspondents
share with me. Sometimes the independent thinkers
prove to be correct, and paradigms shift as a result.
You also know that extraordinary claims require
extraordinary evidence. When a discovery proves to
square with the observable world, scientists make
reputations by confirming it, and corporations
are soon making profits from it. When a
decades-old claim by a "persecuted genius"
finds no acceptance from mainstream science,
it probably failed some basic experimental tests designed
to eliminate self-deception. If you ask me about
something like this, I will simply invite you to
do some tests yourself, perhaps as a high-school
science project. Who knows? Perhaps
it'll be you who makes the next great discovery!
Our world is full of people who have found peace, fulfillment, and friendship
by suspending their own reasoning and
simply accepting a single authority that seems wise and good.
I've learned that they leave the movements when, and only when, they
discover they have been maliciously deceived.
In the meantime, nothing that I can say or do will
convince such people that I am a decent human being. I no longer
answer my crank mail.
This site is my hobby, and I presently have no sponsor.
This page was last updated February 6, 2006.
During the ten years my site has been online, it's proved to be
one of the most popular of all internet sites for undergraduate
physician and allied-health education. It is so well-known
that I'm not worried about borrowers.
I never refuse requests from colleagues for permission to
adapt or duplicate it for their own courses... and many do.
So, fellow-teachers,
help yourselves. Don't sell it for a profit, don't use it for a bad purpose,
and at some time in your course, mention me as author and KCUMB as my institution. Drop me a note about
your successes. And special
thanks to everyone who's helped and encouraged me, and especially the
people at KCUMB
for making it possible, and my teaching assistants over the years.
Whatever you're looking for on the web, I hope you find it,
here or elsewhere. Health and friendship!
As men draw near the common goal,
Keep The Water Flowing.
QUIZBANK:
Lower urinary (all)
OBJECTIVES: The student will give a reasonable account of the origins,
symptoms, signs, epidemiology,
and anatomic pathology of the common bladder lesions.
The student will recognize the common cystoscopic and biopsy
lesions.
INTRODUCTION: Easy unit.
{15588} normal bladder, gross
You remember that normal transitional epithelium (better, "urothelium")
is designed to cover surfaces that change their
areas rapidly.
Urothelium
should be six or fewer cells thick (really, strata of nuclei), perhaps less when the
bladder is full. The superficial layer exhibits the famous protective
layer of broad, flat "umbrella cells", while the basal layer is
famous for its ability to flatten out.
* Urothelium usually produces a bit of mucin,
which explains those few bubbles in the toilet bowl.
Often tumors that arise from
urothelium produce mucin also. This does not make them
"adenocarcinomas".
When urothelium turns to urothelial papilloma-carcinoma, it tends to do so in
multiple places (Nowell's law
again). Forty percent of tumors are multiple at presentation.
This has a lot to do with "frequent recurrences after surgery".
{14941} normal urothelium
A stricture is fibrous tissue partially or totally occluding the lumen of a narrow hollow organ,
usually the ureter or urethra. They may be congenital, but is more often
post-injury scarring (gonorrhea, instrumentation,
stone).
URETER PROBLEMS
You know the anatomy. Acute obstruction causes renal colic, which is often excruciating. Chronic
obstruction is usually asymptomatic, though the kidney won't function and will eventually atrophy.
Places where stones, etc., hang up are (1) the pyelo-ureteric junction; (2) the pelvic brim; (3) the
ureterovesical junction.
Double ureter (bifid ureter) is whole or partial duplication, with two pelvises in the kidney. Big
deal. A few percent of folks have this minor variant.
{15711} bifid ureter, gross
Any obstruction to urinary flow (in the ureter or elsewhere) during fetal life will result in cystic
dysplasia of the portion of the kidney that isn't being properly drained.
An incompetent ureterovesical valve is a common birth defect that causes reflux and predisposes
to kidney infections. It may stay open all the time, or open during micturition.
How to manage these children remains controversial.
Many of these children undergo surgical repair, but the benefit of
surgery over simply treating infection is not clear (Lancet 357:
1329. 2001).
The kidney disease is a mix of renal dysplasia (which is part of the birth
defect) and actual damage from the bacterial infections.
Hydroureter (i.e., dilated ureter) has several causes
Congenital
Pregnancy ("estrogen relaxes smooth muscle", etc.)
Obstruction
Ureter cancer
Chagas's disease
{18791} pyelonephrosis and pyoureters, gross
A very large ureter is called a mega(lo)ureter.
*"Follicular ureteritis" is just big lymph nodules. "Ureteritis cystica" and "Brunn's nests" match their
counterparts in the urinary bladder.
Almost all cancer of the ureter is "urothelial carcinoma", a better
term than the old name "transitional cell carcinoma". Like cancer of the renal pelvis, this is a
variation on bladder cancer, with the same risk factors and a tendency to arise multifocally over
the urothelium.
{10580} urothelial carcinoma, ureter
NON-NEOPLASTIC DISEASE OF THE URINARY BLADDER
Anatomic and clinical pathology have not explained "overactive
bladder", a common problem especially in older women, with discomfort,
frequency, urgency, and/or urge incontinence.
Exstrophy of the urinary bladder results from failure of the pubis to form properly. This is a messy
problem for the surgeon to repair, and of course, infection and poor hygiene are terrible problems.
{10742} exstrophy of the urinary bladder
Persistent urachus, if it is or becomes patent, results in urine dribbling out the navel. More often, urachal cysts
remain. When an adenocarcinoma arises deep in the front of the bladder
wall, it has probably arisen from urachal remnants.
Cystocele is drooping of a portion of the urinary bladder downward into the more caudal areas of the
pelvis. This usually follows childbirth. This may remain filled with urine after voiding, or obstruct
the outlet, inviting infection in either case.
Hypertrophy of the bladder wall results from obstruction, usually from prostatism. The muscle
bundles ("trabeculae") become much more visible ("trabeculation").
{24445} hypertrophy of the bladder from prostatism, gross
Diverticula of the bladder may be congenital, but more often result from a portion of the mucosa
pooching out ("pulsion diverticulum") between two strands of hypertrophied muscle in a person
suffering from chronic obstruction. This may produce the famous "double urination" (* pis à deux,
they call it in France),
and/or a place for stasis, inviting infection, and/or a place
where bladder stones can form.
Purists: Obviously pulsion diverticula of the bladder are pseudodiverticula, just like in the colon.
If a cancer forms here, it has been
considered very serious, since there is no muscularis propria
to slow the invasion. New numbers with fairly good survival statistics (i.e.,
it's the malignant potential of the tumor rather than the presence or
absence of a barrier): Urol. 50: 697, 1997; J. Urol. 170: 1761, 2003.
Bladder stones usually result from infection, and are composed of magnesium ammonium
phosphate.
{21030} bladder stones
Cystitis is usually of bacterial origin, and has the same story as common pyelonephritis, which it
precedes. Urosepsis still kills many adults of both sexes.
The pathology is what you'd expect. Neutrophils abound in the acute
phase. In longstanding disease, there is a chronic inflammatory infiltrate
and there may be much fibrosis.
* Polypoid cystitis is not a tumor at all, but a reactive
overgrowth (collagen and/or extra ground substance) in response to
ongoing inflammation. It may be bullous (i.e., look like blobs) or
papillary (i.e., look like weeds).
The folk wisdom that cranberry juice prevents and helps cure bladder infections is
clearly true (JAMA 271: 751, 1994, others). It prevents
E. coli from forming fimbriae (J. Urol. 159: 559, 1998),
so they cannot bind to their sanctuaries on the bladder mucosa.
It's
the proanthocyanidins (NEJM 339: 1085, 1998).
*The uncommon "emphysematous cystitis" is an unfortunate term for infections with bugs that have
formed gas. "Bullous cystitis" has so much edema between the epithelium and the muscularis
propria that it looks like water balloons. "Encrusted cystitis" is due to urea-splitters and features
magnesium ammonium phosphate plastered over the bladder mucosa.
*All about symptomatic urinary tract infections on young women, with the risk factors of recent
intercourse, use of diaphragm and spermicide, and past history of urinary tract infections: NEJM
335: 468, 1996.
During the 1980's, there was a push to antibiotic-treat all little girls with
asymptomatic bacteriuria, often for a long time. This never made much
sense to me and now it's not much discussed.
Chemotherapy cystitis results from cyclophosphamide ("Cytoxan") or busulfan ("Myleran")
administration, and radiation to the pelvic area can also produce a vicious cystitis.
*"Giant cell cystitis" is a non-disease, merely describing the presence
of giant cells in patients who have had radiation or chemotherapy.
Hunner's interstitial / ulcerative cystitis (Urology 49(5A):
14, 1997) is a poorly-understood process in which all three layers of the
bladder become chronically inflamed.
No histopathologic lesion is diagnostic, but most distinctive is
a marked increase in mast cells.
Patients are mostly women, and they often have considerable
pain and urgency. The pain is probably due, at least in part, to
excess permeability of the urothelium to the potassium in the urine
(Urology 57: 428, 2001; the same is apparently true of the equally-mysterious,
painful
"urethral syndrome".
"Hunner's ulcer" is the advanced stage,
with mucosal breakdown.
The disease is poorly understood, difficult to treat, and probably represents a
common response to any of a variety of immune (?) problems (J. Urol. 153: 629, 1995). The epithelial
cells seem to come apart, and they remain abnormal in culture (J. Urol. 153: 243, 1995).
Malakoplakia is a curious macrophage-rich response to proteus infections. The cells seem to have
some problem phagocytizing the bugs.
Microscopically, you'll see foamy, lipid-laden (*"von Hensemann's) macrophages with calcified
spherules ("Michaelis-Gutmann bodies"). Nobody knows much about this.
*The cure is to use an antibiotic that penetrates macrophages (Lancet 339: 148, 1992); quinolones
seem best (Arch. Int. Med. 156: 577, 1996).
* Brunn's nests are little balls of urothelial-type cells in the lamina propria of the bladder. Cystitis
cystica is like Brunn's nests, only with a hole in the middle. Both are found in a majority of bladders
and mean nothing. In cystitis glandularis, the cells of cystitis cystica produce mucin.
These are all pathologists' curiosities rather than something to worry
about. They suggest that
there's been some inflammation going on.
{25279} Brunn's nests, histology
Squamous metaplasia in endemic areas
usually results from infestation with S. hematobium. This is a terrible public
health problem, and the bladder can be ruined by all the eggs in the muscularis propria.
{09863} Schistosoma hematobium egg, bladder
{24020} urothelial dysplasia with squamous metaplasia; in the background
of urothelial neoplasia, squamous metaplasia
means little or nothing
Don't forget amyloid and amyloidoma as causes of hematuria (the brittle amyloid-laden vessels
crack.)
* Stress incontinence ("I lose urine when I cough")
is a common problem, especially in women who have borne children. The problem
is usually in the structures that support the bladder outlet.
Surgery
often helps.
*Rupture of the bladder from trauma is very serious. (Remember
Fatty Arbuckle and the soda pop / champagne bottle? To this day nobody knows
exactly why
Virginia Rappe's bladder ruptured, but this pathologist can't
believe the
prosecutor's claim that Mr. Arbuckle inserted a bottle into the
lady's bladder without either of them realizing it.)
{25306} amyloidoma, gross
BLADDER TUMORS
Urothelial carcinoma is the usual "bladder cancer" of older adults. It strikes around 40,000
men per year (4th most common cancer), and 14,000 women (9th most common cancer). Around
1/3 of cases eventually prove fatal.
{18788} urothelial carcinoma, gross
The new WHO/International
Society of Urologic Pathologists system is now standard. Urothelial tumors are either flat
or papillary.
For some reason, and unlike most other cancers,
the grade of a urothelial carcinoma is unlikely to
get worse over time; after therapy, it may even get better (i.e., we killed
off all the really anaplastic cells): J. Urol. 169: 2106, 2003.
Bladder cancer genetics update: J. Urol. 171: 419, 2004.
The papillary lesions are most likely to present with hematuria,
either grossly or on microscopic urinalysis. Of course this results
from papillary fronds twisting off and bleeding slightly. Of course,
any mass lesion (papillary or otherwise) can obstruct.
As long as this is the only problem, it doesn't
mean much, other than
Nowell's law is probably operating.
Usually when the number of cell layers is increased,
you'll also see some coarsening of the nuclear chromatin in these cells,
and perhaps a mitosis or two.
If that's all, and the umbrella cells are still
present, pathologists
will describe atypical hyperplasia when this is present.
We don't even know whether really increases the risk of subsequent
cancer.
On cystoscopy, if it is visible
at all, it looks
smooth and red (i.e., the lamina propria is inflamed because
substances from urine leak through) or is sometimes detected only by sampling of the mucosa
by biopsy.
Carcinoma in situ is notoriously unpredictable, and much more
ominous than an actual mass lesion without invasion (J. Urol. 172: 882, 2004).
Around 20-50% of known cases of
carcinoma in situ turn into invasive cancer within five years
(Am. J. Clin. Onc. 21: 217, 1998),
and it can sometimes metastasize without an identifiable invasive mass.
We believe that many (most?) invasive
cancers start here rather than in papillary lesions;
the numbers are still being sorted out.
Papillary urothelial tumors Urothelial papillomas (grade 0 tumors) grow
up from the mucosa ("like a glove with fingers"),
and are covered with normal
urothelium.
Unless they bleed, you'll never know they're there. (WHO regulations specify that if the
epithelium is more than 6-8 nuclear layers thick, you must call it grade I cancer; not everybody believes this.)
Papillary tumors of low malignant potential (Grade I)
is
papillary lesions
in which the surface epithelium is merely hyperplastic and/or the cells
show minimal anaplasia. Nowadays
all of the latter be given "Grade I". Be this as it may, these tumors
almost never turn invasive. Low-grade urothelial carcinomas (Grade II)
tend to assume a papillary growth pattern, and turn invasive
only after many years (if ever). There is a bit more anaplasia
than in a Grade I, the chromatin is coarser, there may be little
nucleoli visible, and you may even find rare mitotic figures.
Often the only
marker for malignancy is a slight increase in N/C ratio and
slight loss of nuclear orientation.
Even the umbrella layer is often intact in
one of these "low-grade" tumors. Another helpful sign of cancer is loss of
the usual "clear cytoplasm" seen in some cells in a normal urothelium. These little
cancers usually remain asymptomatic for years, and probably most of them never invade.
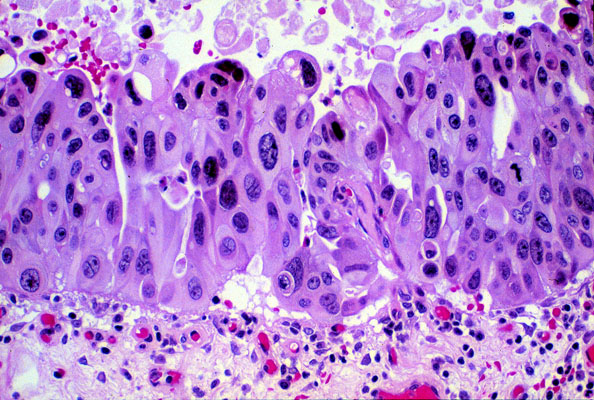
High-grade urothelial carcinomas (Grade III) tend to be invasive when they become
symptomatic, and to progress rapidly
to death.
If discovered early, though, only a minority invade (Br. J. Urol. 83:
957, 1999).
As you'd expect, bladder discomfort, painless hematuria, and infection are typical
presentations. A few authorities add "Grade IV" if there is necrosis and/or
you can't really tell it's urothelial, for what it's worth.
Regardless of grade, urothelial carcinomas are "superficial" until they extend among
the inmost fibers of the muscularis propria. (There is seldom an obvious a muscularis
mucosae in the bladder; if there is, invasion of this doesn't count against
the tumor being "superficial".)
Spotting superficial infasion:
Aggressive papillary lesions can be identified
by staining for p53, high division index (Ki-67), and
having cytokeratin 20-positivity throughout the epithelium rather
just in the surface (as in normal urothelium).
Great photos: Am. J. Clin. Path. 121: 679, 2004; Cancer 97:
1876, 2003.
The correlation with the new grading system is excellent.
One piece of big news in bladder cancer is the discovery that even the
precursor lesions usually stain with Lewis X antigen. This allows
easy screening of urine samples (J. Urol. 159: 384 & 389, 1998).
Watch this one.
Finding the malignant areas to biopsy using laser-induced
autofluorescence: J. Urol. 159: 1871, 1998. Risk factors for urothelial carcinoma include cigaret smoking (2-4x base risk),
exposure to certain chemicals in industry (outstandingly the dye industry,
outstandingly such aromatic amines as α-naphthylamine,
auramine, and benzidine), abuse
of phenacetin,
carbon black (Lancet 358: 562, 2001),
that now-infamous Aristolochia Chinese herbal "weight loss" pill from
the early 1990's (NEJM 342: 1686, 2000 -- most of
the victims now have urothelial dysplasia or worse, didn't get to the US),
exposure to cyclophosphamide, Lynch's nonpolyposis colon cancer
family syndrome (x14, J. Urol. 160: 466, 1998),
and having a longstanding indwelling
catheter (i.e., paraplegics and quadriplegics).
The urothelium, of course, is exposed to many carcinogens, which we
may think are concentrated in the urine; nobody should be surprised to learn
that the more water you drink, the lower your risk of bladder cancer
(NEJM 340: 1390, 1999).
Your lecturer, after reviewing the evidence, believes that allegations that
cyclamates and saccharine cause bladder cancer in humans are
rubbish, and the ban resulted from
junk science and politics-as-usual. These were given in preposterously large doses to experimental animals,
and nobody has been able to show the expected epidemiologic links.
* Future pathologists: How to "gross in" a bladder: J. Urol. 171: 1823, 2004; Cancer 100:
2470, 2004; Arch. Path. Lab. Med. 127: 1263, 2003.
Adenocarcinoma of the bladder is uncommon. Two types are
distinguished by location, one arising from where the urachus used to
be, high on the front of the bladder,
the other arising around the trigone
(usually) from "cystitis glandularis" (maybe) or "colonic metaplasia" (known to be
premalignant).
Squamous cell carcinoma of the bladder usually arises in squamous metaplastic
epithelium, i.e., the patient has schistosomiasis. This is the great cancer menace in
Egypt, and it is extremely aggressive and lethal. Even a significant amount
of real squamous metaplasia in a urothelial carcinoma is ominous.
Pheochromocytoma: Urinating turns from a pleasure to a headache. Uncommon, but
memorable.
*Children are prone to exotic mesenchymal tumors, especially
rhabdomyosarcomas. To diagnose a rhabdo here, you'll want
to see plenty of anaplasia, a cambium layer,
and at least a few good round rhabdomyoblasts.
* Small-cell carcinoma of the bladder, which often arises
in a more conventional-style bladder cancer, looks like oat-cell carcinoma
of the lung on microscopy and electron microscopy, and is aggressive as you'd expect,
though cures aren't unknown.
* Nephrogenic adenoma is a papillary mass of loose,
inflamed connective tissue
with hobnail cells all over its surface.
It's probably a curious reparative response rather than a true
tumor, since it usually follows injury.
Tubules resembling kidney collecting
ducts and Henle's loops penetrate deep into it. As you would expect, patients
present with bleeding.
URETHRA
In either sex: Patients complaining of urethritis symptoms need to be questioned about
consumption of jalepiño peppers.
Posterior stricture: A man's problem. Often congenital. The urologist can help you.
Urethral caruncle: A woman's problem, often developing later in life, near the opening
of the urethra. Perhaps it begins with plugging of the ducts of the glands.
It is an uncomfortable
lesion with mixed inflammation of the lamina propria, and often with
pseudoepitheliomatous hyperplasia of the overlying squamous
epithelium.
{14937} ureter (cross section), normal
 I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
Pathology Education Instructional Resource -- U. of Alabama; includes a digital library
Houston Pathology -- loads of great pictures for student doctors
Pathopic -- Swiss site; great resource for the truly hard-core
Syracuse -- pathology cases
Walter Reed -- surgical cases
Alabama's Interactive Pathology Lab
"Companion to Big Robbins" -- very little here yet
Alberta
Pathology Images --hard-core!
Cornell
Image Collection -- great site
Bristol Biomedical
Image Archive
EMBBS Clinical
Photo Library
Chilean Image Bank -- General Pathology -- en Español
Chilean Image Bank -- Systemic Pathology -- en Español
Connecticut
Virtual Pathology Museum
Australian
Interactive Pathology Museum
Interactive Pathology Museum
Semmelweis U.,
Budapest -- enormous pathology photo collection
Iowa Skin
Pathology
Loyola
Dermatology
History of Medicine -- National Library of Medicine
KU
Pathology Home
Page -- friends of mine
The Medical Algorithms Project -- not so much pathology, but worth a visit
National Museum of Health & Medicine -- Armed Forces Institute of Pathology
Telmeds -- brilliant site by the medical students of Panama (Spanish language)
U of
Iowa Dermatology Images
U Wash
Cytogenetics Image Gallery
Urbana
Atlas of Pathology -- great site
Visible
Human Project at NLM
WebPath:
Internet Pathology
Laboratory -- great site My team:
My team:Ed Lulo's Pathology Gallery
Bryan Lee's Pathology Museum
Dino Laporte: Pathology Museum
Tom Demark: Pathology Museum
Dan Hammoudi's Site
Claude Roofian's Site
Pathology Handout -- Korean student-generated site; I am pleased to permit their use of my cartoons
Estimating the Time of Death -- computer program right on a webpage
Pathology Field Guide -- recognizing anatomic lesions, no pictures

St.
Jude's Ranch for Children
I've spent time there and they are good. Write "Thanks
Ed" on your check.
PO Box 60100
Boulder City, NV 89006--0100
More of my notes
My medical students
Clinical
Queries -- PubMed from the National Institutes of Health.
Take your questions here first.
HealthWorld
Yahoo! Medline lists other sites that may work well for you

We comply with the
HONcode standard for health trust worthy
information:
verify
here. 

![]()
Could anything be sadder
Than he who, master of his soul,
Is servant of his bladder?
-- Anonymous!
-- "The First Principle of Urology"
 Bladder Exhibit
Bladder Exhibit
Virtual Pathology Museum
University of Connecticut
{15771} normal bladder, gross
{15772} normal bladder, gross
{15587} normal bladder and prostate, gross
{15114} normal bladder, histology
{15120} normal bladder, histology
{15326} normal bladder, histology
{25266} normal bladder histology
Normally,
it takes about a year to replace itself, so you're unlikely to see any mitotic figures until there's
serious disease.
{14937} normal ureter histology
{10022} normal urothelial, cytology
This is a very important cause of kidney failure in children.
Bladder cancer
Prostate cancer
Cervix cancer
Metastases in the para-aortic lymph nodes
Etc.
 You learned in physiology and neuroscience class about the various problems with voiding when the
cortex and bladder are separated. When the bladder is inflamed, urinating can be uncomfortable,
and often the bladder contracts with excessive force (urgency). See "Big Robbins" for a common-sense list of causes of bladder
outlet obstruction.
You learned in physiology and neuroscience class about the various problems with voiding when the
cortex and bladder are separated. When the bladder is inflamed, urinating can be uncomfortable,
and often the bladder contracts with excessive force (urgency). See "Big Robbins" for a common-sense list of causes of bladder
outlet obstruction.
*Future pathologists: You'll learn to recognize "cytoxan cells",
which have big hyperchromatic nuclei and scanty cytoplasm, but smudgy
nuclear chromatin that lets you know they're not cancer.
 Grossly, you'll see soft ("malakos" in Greek) yellow plaques.
Grossly, you'll see soft ("malakos" in Greek) yellow plaques.
{25276} malakoplakia, histology
{24004} malakoplakia, Michaelis-Gutmann bodies
{25280} cystitis cystica, histology
{24007} cystitis glandularis, histology
Having a catheter in the bladder for a long time can cause protective
squamous metaplasia of the urothelium. Squamous cell carcinoma has been
an under-recognized problem in these people (J. Urol. 161:
1106, 1999.)
{25307} amyloidoma, histology (including congo Red)

{21029} urothelial carcinoma, gross
{08858} urothelial carcinoma, histology
{08859} urothelial carcinoma, histology
{08860} urothelial carcinoma, histology
{08861} urothelial carcinoma, histology
{17200} urothelial carcinoma, histology
{17202} urothelial carcinoma, histology
{23987} urothelial carcinoma, histology
{24019} urothelial carcinoma, histology
{24082} urothelial carcinoma, cytology
{24083} urothelial carcinoma, cytology
{10034} urothelial carcinoma, cytology
{10040} urothelial carcinoma, cytology
 Bladder carcinoma in situ
Bladder carcinoma in situ
Very anaplastic, no invasion
KU Collection
Naming urothelial tumors is confusing and aggravating because no one truly knows
the natural history of lesions that are always removed as soon
as they are discovered, and where it isn't really possible to tell a recurrence
from a second primary (and 70% of survivors will get a second
urothelial primary).
Hence, there have been several different systems
of nomenclature, and certain lesions that are "benign" in some
are "malignant" in others.
The flat lesions are most likely to present with discomfort,
if they are symptomatic at all. The reason for this is that the integrity
of the epithelial barrier is somewhat compromised, and salty urine
contacts the nerves of the mucosa. (Remember how much potassium hurts
when it contacts an exposed nerve?)
Flat urothelium:Hyperplasia of urothelium is said to be present when it
is "flat and >6 cells thick" (i.e., there are
more than 6 layers of nuclei; the number depends on who you believe).
Carcinoma in situ of the bladder is defined to be replacement of the flat
urothelium by obviously anaplastic cells that have not invaded. Usually
asymptomatic, it may be uncomfortable if it allows backleak of electrolytes, since the
salty urine stimulates pain fibers in the submucosa.
One of my favorites is the inverted papilloma, a smooth-surfaced
bump with
epithelium complexly infolded deep within it. ("A glove with the fingers
pushed inside and collapsed.") There is no atypia, no desmoplasia,
and there's a good top layer to the epithelium. So it shouldn't be mistaken
for cancer.
* Future pathologists: The stroma of a Grade I may be very delicate,
like wispy seaweed; a Grade 0 will be more substantial.
You'll learn the new staging systems on rotations.
One of the common tough calls in pathology is, "Is this papillary
urothelial carcinoma of the bladder still confined to the
epithelium (Ta) or down into the lamina propria (T1)?"
* Immunohistopathology helps make the hard calls.
You need to know of a few other bladder tumors.
Carcinoma in situ is likely to stain for p53 and/or
cytokeratin 20,
and to have a high division index as shown by MIB-1 / Ki-67.
Long-term use of hair dye, or being a long-term hairdresser,
seem to be risk factors (2x and 5x respectively: Mut. Res. 506: 21, 2002;
Int. J. Ca. 91: 575, 2001).
Patients with superficial bladder
cancer usually do well, especially with today's treatment, which often
includes intravesical BCG. Prognosis in urothelial carcinoma depends on grade-and-stage (correlate pretty
well most of the time). For the less-ugly, low-stage cancers, prognosis correlates
with other markers of malignancy, including loss of ABO antigens (*demonstrated
by some of your lecturer's Chicago friends), aneuploidy, and activation of known
oncogenes.
 Rhabdomyosarcoma of bladder
Rhabdomyosarcoma of bladder
Virtual Hospital
I peed in the Rhine.
--George S. Patton
Marginal note, March 1945
 * SLICE OF LIFE REVIEW
* SLICE OF LIFE REVIEW
{14938} ureter (cross section), normal
{14939} ureter (epithelium), normal
{14940} urinary bladder, normal
{14941} urothelium, normal
{15032} urethra, normal
{15033} urethra, normal
{15108} ureter
{15109} ureter
{15111} ureter
{15112} ureter
{15113} bladder, urinary
{15114} bladder, urinary
{15119} bladder, urinary
{15120} bladder, urinary
{15122} bladder, urinary
{15325} ureter, normal
{15326} bladder, normal
{15327} bladder, normal
{15588} bladder, normal
{15771} bladder normal unfixed, inner surface
{15772} bladder normal unfixed, inner surface
{20930} urethra
{20931} urinary bladder
{25172} urethra, normal
{25174} urethra, normal
{25266} bladder, normal


| Visitors to www.pathguy.com reset Jan. 30, 2005: |
Ed says, "This world would be a sorry place if
people like me who call ourselves Christians
didn't try to act as good as
other
good people
."
Prayer Request
 Teaching Pathology
Teaching Pathology
PathMax -- Shawn E. Cowper MD's
pathology education links
Ed's Autopsy Page
Notes for Good Lecturers
Small Group Teaching
Socratic
Teaching
Preventing "F"'s
Classroom Control
"I Hate Histology!"
Ed's Physiology Challenge
Pathology Identification
Keys ("Kansas City Field Guide to Pathology")
Ed's Basic Science
Trivia Quiz -- have a chuckle!
Rudolf
Virchow on Pathology Education -- humor
Curriculum Position Paper -- humor
The Pathology Blues
 Ed's Pathology Review for USMLE I
Ed's Pathology Review for USMLE I
![]()
![]()
 | Pathological Chess |
 |
Taser Video 83.4 MB 7:26 min |

 Bladder
Bladder Ureteritis cystica
Ureteritis cystica Cloacal malformation
Cloacal malformation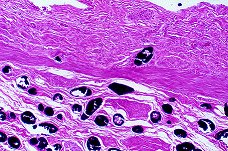 Bladder schistosomiasis
Bladder schistosomiasis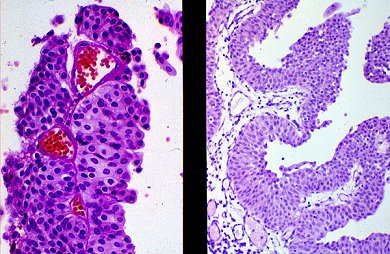 Papillary urothelial carcinoma
Papillary urothelial carcinoma Urothelial carcinoma
Urothelial carcinoma